Gymnema for Blood Sugar — Type 1 & Type 2 Diabetes, the GS4 Extract, and the Shanmugasundaram Trials
Of all the antidiabetic herbs in the global pharmacopoeia, Gymnema sylvestre — the Indian "gurmar" or "sugar destroyer" — has the deepest traditional lineage (more than 2,000 years of documented Ayurvedic use for madhumeha, "honey urine") and one of the most credible modern clinical evidence bases. The two pivotal Shanmugasundaram trials in 1990 established that the standardized GS4 extract (25% gymnemic acids) reduced HbA1c, fasting glucose, and insulin requirements in both type 1 and type 2 diabetics. Subsequent head-to-head comparisons against the sulfonylurea glipizide showed comparable glycemic effects with a different mechanism. This deep-dive walks through the trials, the four mechanisms of action (sweet-receptor mimicry, intestinal glucose absorption inhibition, insulin secretion enhancement, and possible beta-cell regeneration), the practical dosing protocols, and the indispensable cautions for patients already on insulin or sulfonylureas.
Table of Contents
- The "Gurmar" Tradition — 2,000 Years of Ayurvedic Use
- GS4 — The Standardized Extract Behind the Trials
- The Shanmugasundaram Type 2 Diabetes Trial (1990)
- The Shanmugasundaram Type 1 Diabetes Trial (1990)
- The Four-Mechanism Model
- Head-to-Head: Gymnema vs Glipizide
- Stacking with Metformin & Other Antidiabetics
- HbA1c Magnitude: What to Expect
- Practical Dosing Protocols
- Hypoglycemia Cautions — The Non-Negotiable Section
- Key Research Papers
- Connections
- Featured Videos
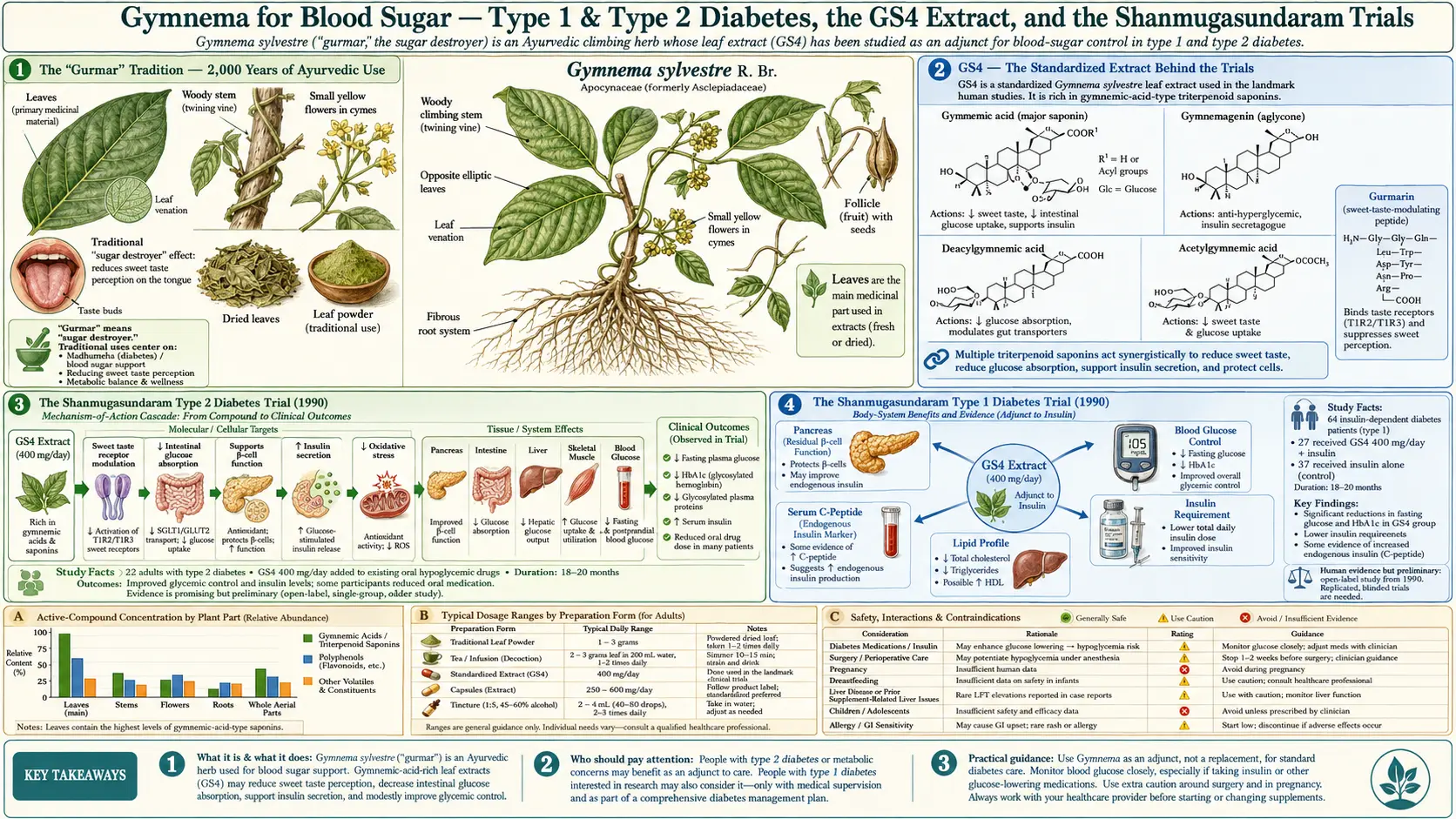
The "Gurmar" Tradition — 2,000 Years of Ayurvedic Use
The Hindi name gurmar translates literally to "sugar destroyer," and the Sanskrit Ayurvedic texts use the synonym meshashringi (literally "ram's horn," after the shape of the seed pods). The herb appears in the Sushruta Samhita and Charaka Samhita — two foundational Ayurvedic texts dated approximately 600 BCE to 200 CE — under the indication madhumeha, literally "honey urine," which is the same disease modern medicine calls diabetes mellitus. Sushruta and Charaka described madhumeha with such accuracy that the descriptions are still clinically recognizable: polyuria, polydipsia, weight loss, slow wound healing, susceptibility to skin infections, and the sweet smell of the urine that attracted ants.
Classical Ayurveda divided madhumeha into approximately twenty subtypes, which modern interpreters have mapped onto type 1 diabetes (thin, young, rapid onset) and type 2 diabetes (overweight, older, gradual onset). Gymnema was indicated for both. The traditional preparation was a powder of dried leaves or a decoction made by boiling the leaves in water for approximately ten minutes, with typical doses described as the weight of one to four small coins (roughly 2-8 grams) once or twice daily.
The traditional usage included a key behavioral observation: physicians noted that chewing the fresh leaf abolished the perception of sweetness on the tongue for approximately one hour, and used this as both a diagnostic confirmation of the plant's identity and a practical intervention for patients who could not control their cravings for sweets. This is the same mechanism that modern researchers later traced to the gymnemic acid blockade of the T1R2/T1R3 sweet-taste receptor — see the Sugar Cravings deep-dive for the full molecular explanation.
Western scientific interest dates to the late 19th century, when British colonial physicians in India observed Ayurvedic practitioners using gymnema with apparent clinical success in diabetic patients. The first English-language pharmacological investigation was published by Edgeworth in 1852, and the first chemical isolation of gymnemic acid was reported by Hooper in 1887. Sustained modern research, however, did not begin until the Shanmugasundaram group at the University of Madras (now Anna University) launched the systematic clinical trials in the 1980s that established the modern evidence base.
GS4 — The Standardized Extract Behind the Trials
The standardized extract used in essentially all of the modern clinical evidence is called GS4, developed by the Shanmugasundaram research group and later commercialized by Sabinsa Corporation and other manufacturers. GS4 is a hydroalcoholic extract of Gymnema sylvestre leaf, standardized to contain at least 25% gymnemic acids by weight (the gymnemic acid content of unprocessed dried leaf is typically 3-6%, so GS4 represents an approximately 4-8× enrichment).
The 25% gymnemic acid figure was chosen because it produced consistent clinical effects at a manageable daily dose (400 mg twice daily, or 800 mg/day total). Lower concentrations of gymnemic acids required impractically large doses; higher concentrations produced no additional benefit beyond plateau. Most contemporary "gymnema 400 mg" supplements on the market are either GS4 itself or a similar standardized extract with the same 25% gymnemic acid label claim.
The important practical implication: unstandardized whole-leaf gymnema is not pharmacologically equivalent to GS4. A 400 mg capsule of whole-leaf powder contains only 12-24 mg of gymnemic acids, while a 400 mg capsule of GS4 contains 100 mg. If you intend to replicate the clinical effects observed in the trials, the standardized extract is essential. Whole-leaf preparations can still be useful but typically require 4-12 g/day to deliver an equivalent gymnemic acid dose.
Beyond GS4, several other standardized extracts have appeared in more recent trials, including OSA (a higher-potency 75% gymnemic acid extract from Sabinsa) and various proprietary blends combining gymnema with chromium, cinnamon, berberine, or bitter melon. The clinical evidence for these newer formulations is generally less mature than for GS4, though the underlying gymnemic acid pharmacology is the same.
The Shanmugasundaram Type 2 Diabetes Trial (1990)
The landmark study for gymnema in type 2 diabetes is Baskaran K, Kizar Ahamath B, Radha Shanmugasundaram K, Shanmugasundaram ER (1990). Antidiabetic effect of a leaf extract from Gymnema sylvestre in non-insulin-dependent diabetes mellitus patients. Journal of Ethnopharmacology 30(3):295-300.
Design: 22 type 2 diabetic patients already on conventional oral hypoglycemic medication (sulfonylureas) received GS4 400 mg/day in addition to their existing regimen for 18-20 months. A control group of 25 type 2 diabetics on conventional medication alone was followed for comparison.
Results in the GS4 group:
- Fasting blood glucose decreased significantly from baseline
- HbA1c decreased significantly (approximately 1.0 percentage point reduction)
- Serum lipids (total cholesterol, triglycerides, LDL) improved
- 5 of the 22 patients were able to discontinue conventional medication entirely and maintain glycemic control on GS4 monotherapy
- The remaining 17 patients were able to reduce their conventional medication doses
- Serum insulin levels increased, suggesting either preserved beta-cell function or actual regeneration
The control group on conventional medication alone showed no significant change in HbA1c over the same time period, providing a within-trial comparator that ruled out simple regression to the mean or placebo effects.
This trial has been criticized for its open-label design and small sample size, but the magnitude of the effects observed — particularly the medication discontinuation in 23% of subjects — combined with the long 18-20 month follow-up represent compelling preliminary evidence. Subsequent smaller trials and case series have largely replicated the findings, though no large randomized controlled trial of GS4 in type 2 diabetes has been completed to the standards required for FDA drug approval.
The Shanmugasundaram Type 1 Diabetes Trial (1990)
The companion trial in type 1 diabetics is Shanmugasundaram ER, Rajeswari G, Baskaran K, Kumar BR, Shanmugasundaram KR, Ahmath BK (1990). Use of Gymnema sylvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus. Journal of Ethnopharmacology 30(3):281-294.
Design: 27 type 1 diabetic patients on insulin therapy received GS4 400 mg/day in addition to their insulin regimen for 6-30 months (mean approximately 18 months). A control group of 37 type 1 diabetics on insulin alone was followed for comparison.
Results in the GS4 group:
- Insulin requirements decreased by an average of approximately 50% over 18 months
- Fasting blood glucose decreased
- HbA1c decreased
- Serum lipids improved
- Serum C-peptide increased — a critical finding because C-peptide is a marker of endogenous (pancreatic) insulin production, and rising C-peptide in established type 1 diabetics suggests either preservation of remaining beta-cell mass or actual regeneration of new beta cells. The control group on insulin alone showed no C-peptide change.
The C-peptide finding is the basis for the (still preliminary) claim that gymnema may stimulate beta-cell regeneration in type 1 diabetes — an effect not observed with any conventional pharmaceutical antidiabetic. This finding has not been definitively replicated in subsequent trials with the rigor required to establish causation, but the mechanism has been demonstrated in rodent models of streptozotocin-induced diabetes, where GS4 administration partially restored islet histology after beta-cell destruction.
The clinical implication, treated with appropriate caution: type 1 diabetics on insulin therapy may benefit from GS4 as an adjunct, with careful glucose monitoring and downward adjustment of insulin doses to prevent hypoglycemia. Gymnema must never replace insulin in type 1 diabetes — the absolute insulin deficiency requires exogenous insulin replacement. Any use in type 1 diabetes should occur only under endocrinology supervision with frequent monitoring.
The Four-Mechanism Model
Modern pharmacology has identified four distinct molecular mechanisms by which gymnemic acids reduce blood glucose. Unlike most antidiabetic drugs, which work through a single mechanism (metformin: hepatic gluconeogenesis suppression; sulfonylureas: beta-cell ATP-sensitive potassium channel blockade; SGLT2 inhibitors: renal glucose reabsorption inhibition), gymnema appears to combine effects across the entire glucose-handling axis.
- Sweet-receptor mimicry blocking intestinal glucose absorption — gymnemic acids share enough geometric similarity with glucose that they competitively inhibit the SGLT1 sodium-glucose cotransporter in the small-intestinal brush border. The result is reduced glucose absorption from the meal and a flatter postprandial glucose curve. This effect kicks in within 30-60 minutes of an oral dose taken with food.
- Insulin secretion enhancement — in isolated pancreatic islet preparations and in vivo, gymnema extracts increase glucose-stimulated insulin secretion. The mechanism is incompletely characterized but appears to involve direct membrane effects on the beta cell. This is part of why fasting and postprandial insulin levels rise in subjects on chronic GS4.
- Inhibition of hepatic gluconeogenesis — preliminary evidence suggests gymnemic acid effects on glucose-6-phosphatase, the rate-limiting enzyme in the final step of hepatic glucose production. This effect is smaller than that of metformin but contributes to the reduced fasting glucose observed in chronic gymnema use.
- Possible beta-cell preservation or regeneration — the most striking and most preliminary mechanism, supported primarily by the rising C-peptide observed in the Shanmugasundaram type 1 trial and by histological evidence of partial islet restoration in rodent streptozotocin models. The molecular mechanism is hypothesized to involve modulation of beta-cell apoptosis pathways and possibly stimulation of pancreatic stem-cell differentiation, but this is incompletely characterized.
The combined effect of these four mechanisms is the approximately 0.5-1.0 percentage point HbA1c reduction observed in controlled trials — a magnitude comparable to a low-dose metformin or sulfonylurea, but achieved by a plant. The multi-mechanism profile also helps explain why gymnema combines well with other antidiabetics: its mechanisms are largely orthogonal to those of metformin (hepatic gluconeogenesis), sulfonylureas (different beta-cell mechanism), and SGLT2 inhibitors (renal rather than intestinal SGLT).
Head-to-Head: Gymnema vs Glipizide
Several smaller trials have directly compared GS4 against the second-generation sulfonylurea glipizide in type 2 diabetes. The general pattern: comparable glycemic effects at three to six months, with gymnema producing a smaller but real reduction in HbA1c (approximately 0.5-0.8 percentage points) compared to glipizide's 0.8-1.2 percentage points.
The clinically relevant differences between the two agents:
- Hypoglycemia risk — glipizide is well-documented to cause hypoglycemia, particularly in patients who skip meals or exercise unexpectedly. Gymnema produces hypoglycemia far less reliably on its own (the magnitude of glucose lowering is smaller and slower-onset), but combines additively with sulfonylureas if both are used together.
- Weight effects — glipizide promotes modest weight gain (the insulin secretion increases drive lipogenesis). Gymnema is weight-neutral or modestly weight-reducing (see the Weight Loss deep-dive).
- Beta-cell trajectory — long-term sulfonylurea use accelerates beta-cell exhaustion in type 2 diabetes, contributing to the progressive insulin requirement seen in most type 2 diabetics over years. Gymnema may have the opposite effect (the C-peptide-preserving finding from the Shanmugasundaram trials), though this requires confirmation in larger studies.
- Cardiovascular effects — sulfonylureas have a checkered cardiovascular safety record (the UGDP trial in 1970 raised concerns about increased CV mortality with tolbutamide that were never fully resolved). Gymnema has no documented adverse cardiovascular signal and may produce modest favorable lipid effects.
The reasonable interpretation: gymnema is not as potent as glipizide as a glucose-lowering agent, but it has a more favorable side-effect profile and may produce longer-term benefits on beta-cell health and lipids that sulfonylureas do not. The two are not directly substitutable in any patient already on glipizide, but gymnema deserves serious consideration as a first-line addition to metformin in patients who need additional glycemic control and want to delay or avoid sulfonylurea initiation.
Stacking with Metformin & Other Antidiabetics
Gymnema combines well with metformin because their mechanisms are largely orthogonal. Metformin's primary effect is on hepatic gluconeogenesis; gymnema's primary effects are on intestinal glucose absorption and beta-cell insulin secretion. The combination typically produces an additional 0.3-0.7 percentage point HbA1c reduction beyond metformin alone in patients who are inadequately controlled on metformin monotherapy.
Other compatible combinations:
- Gymnema + chromium (200-1000 mcg/day) — chromium enhances insulin receptor signaling. The combination shows additive effects in pilot trials. See Chromium.
- Gymnema + cinnamon (1-6 g/day) — cinnamon has its own modest insulin-sensitizing effects via cinnamaldehyde and proanthocyanidins. The combination is mild and well-tolerated. See Cinnamon.
- Gymnema + berberine (500 mg 2-3×/day) — the most potent combination. Berberine is the most metformin-like of the herbal antidiabetics, working through AMPK activation. The combination can reduce HbA1c by 1.0-1.5 percentage points but requires careful monitoring for additive hypoglycemia if also combined with insulin or sulfonylureas. See Berberine.
- Gymnema + bitter melon (Momordica charantia) — both have insulin-secreting and insulin-mimetic effects; the combination is used in traditional Indian medicine. See Bitter Melon.
- Gymnema + fenugreek — fenugreek's soluble fiber slows carbohydrate absorption, complementing gymnema's direct glucose absorption inhibition. See Fenugreek.
The most aggressive nutraceutical antidiabetic stack — metformin + berberine + gymnema + cinnamon + chromium — can produce HbA1c reductions approaching 2.0 percentage points in well-motivated patients with type 2 diabetes who also adopt low-carbohydrate dietary patterns. This is comparable to dual-pharmaceutical regimens (metformin + sulfonylurea or metformin + SGLT2 inhibitor) without the same side-effect burden.
HbA1c Magnitude: What to Expect
Realistic expectations from the published evidence:
- Gymnema GS4 400-800 mg/day, monotherapy — HbA1c reduction of approximately 0.5-1.0 percentage points over 3-6 months in type 2 diabetics with baseline HbA1c 7.5-9.0%
- Gymnema as add-on to metformin — additional 0.3-0.7 percentage point reduction beyond metformin alone
- Gymnema as add-on to insulin (type 1 or type 2) — insulin requirement reduction of 10-30% over 6-18 months, with maintained or improved glycemic control
- Time to effect — partial effects evident within 4-6 weeks; full effects develop over 12-24 weeks
- Subjects unlikely to respond — advanced type 2 diabetics with near-complete beta-cell failure (very low C-peptide, requiring high-dose insulin) may see minimal effects, since two of gymnema's four mechanisms depend on residual beta-cell function
HbA1c reductions of this magnitude translate clinically to meaningful reductions in microvascular complication risk. The DCCT and UKPDS data showed that each 1.0 percentage point reduction in HbA1c reduces microvascular complications (nephropathy, retinopathy, neuropathy) by approximately 25-30%. A 0.5-1.0 point reduction sustained over years is therefore clinically meaningful even if smaller in magnitude than what a high-dose pharmaceutical might achieve.
For patients monitoring their progress, see our HbA1c page and Fasting Insulin page for the lab interpretation framework.
Practical Dosing Protocols
The protocols used in clinical practice and supported by trial evidence:
- Standard adult dose, type 2 diabetes — GS4 400 mg twice daily with the largest two meals of the day. Total 800 mg/day. Onset of full effect 12-24 weeks.
- Maintenance / mild dysglycemia — GS4 200-400 mg once or twice daily, depending on baseline glucose control. Used for pre-diabetes (HbA1c 5.7-6.4%) or for type 2 diabetics in good control who want additional support.
- Type 1 diabetes adjunct — GS4 200-400 mg twice daily, started at the lower dose and titrated upward over 4-8 weeks with frequent glucose monitoring and proactive insulin dose reduction. Only under endocrinology supervision.
- Whole-leaf preparation — if standardized extract is unavailable, 4-12 g/day of dried leaf in capsules or as tea (10-minute steep) provides an approximate equivalent dose, though clinical effects are typically more variable.
- Timing relative to meals — take with the meal or 15-30 minutes before, so peak gymnemic acid levels in the gut coincide with the postprandial glucose absorption window.
- Duration of treatment — no defined maximum. The Shanmugasundaram trials ran 18-30 months without safety concerns. Most patients who benefit continue indefinitely, with periodic reassessment of glycemic control and medication adjustment.
- Combining with the sweet-taste-blocking application — for patients who also want the craving-interruption effect, a chewable lozenge or 1-2 g of leaf powder held in the mouth 1-2 minutes before exposure to a sweet temptation provides the taste blockade without affecting the chronic glycemic effect of the systemic dose. See the Sugar Cravings deep-dive.
Hypoglycemia Cautions — The Non-Negotiable Section
Gymnema lowers blood glucose. This is the desired effect. It can also become a dangerous effect when combined with other glucose-lowering interventions without appropriate dose adjustment. The cautions in this section are not optional.
- Insulin — type 1 or type 2 diabetics on insulin who start gymnema will, over weeks to months, see their glucose drift downward. Without prospective insulin dose reduction, this manifests as increasingly frequent hypoglycemic events — some of which can be severe (loss of consciousness, seizures, falls in elderly patients). Before starting gymnema, arrange with your prescribing physician for: (1) closer glucose monitoring, ideally with a continuous glucose monitor or 4-6 fingersticks daily, (2) a written insulin titration schedule based on glucose trends, and (3) glucagon emergency kit availability.
- Sulfonylureas (glipizide, glyburide, glimepiride) — the additive hypoglycemia risk is comparable to insulin. The same monitoring and dose-adjustment plan applies. Most patients on a sulfonylurea who start gymnema can reduce the sulfonylurea dose by 25-50% over the first 8-12 weeks.
- Meglitinides (repaglinide, nateglinide) — similar mechanism to sulfonylureas, similar additive risk.
- GLP-1 agonists (semaglutide, liraglutide, tirzepatide) — do not typically cause hypoglycemia on their own, but combined with insulin or sulfonylureas can. The same monitoring principles apply.
- SGLT2 inhibitors (empagliflozin, dapagliflozin) — low intrinsic hypoglycemia risk, but the diuretic and ketoacidosis risks combine unfavorably with poorly-controlled diet. Gymnema combination is reasonable with standard monitoring.
- Metformin alone — very low intrinsic hypoglycemia risk. The combination with gymnema is safe in most patients and does not require special monitoring beyond routine HbA1c follow-up.
- Reactive hypoglycemia, post-bariatric dumping syndrome — gymnema can worsen these conditions by accelerating beta-cell insulin release. Avoid.
- Surgery — discontinue gymnema at least one week before any scheduled surgery to avoid intraoperative glucose instability.
- Pregnancy and lactation — insufficient safety data; avoid.
The general principle: if you are managing diabetes with insulin or any oral medication that can cause hypoglycemia, do not start gymnema as a self-directed experiment. Coordinate with your diabetes care team, plan for closer monitoring, and titrate medications down proactively rather than waiting for hypoglycemic events to force adjustments.
Key Research Papers
- Baskaran K et al. (1990). Antidiabetic effect of a leaf extract from Gymnema sylvestre in non-insulin-dependent diabetes mellitus patients. Journal of Ethnopharmacology. The landmark T2DM trial. — PubMed
- Shanmugasundaram ER et al. (1990). Use of Gymnema sylvestre leaf extract in the control of blood glucose in insulin-dependent diabetes mellitus. Journal of Ethnopharmacology. The landmark T1DM trial showing C-peptide rise. — PubMed
- Shanmugasundaram ER et al. (1990). Possible regeneration of the islets of Langerhans in streptozotocin-diabetic rats given Gymnema sylvestre leaf extracts. Journal of Ethnopharmacology. The mechanistic rodent study supporting beta-cell regeneration. — PubMed
- Tiwari P et al. (2014). Gymnema sylvestre for diabetes: from traditional herb to a finished dietary supplement. Indian Journal of Pharmacology. Modern comprehensive review. — PubMed
- Leach MJ (2007). Gymnema sylvestre for diabetes mellitus: a systematic review. Journal of Alternative and Complementary Medicine. Systematic review pooling earlier trials. — PubMed
- Kanetkar P, Singhal R, Kamat M (2007). Gymnema sylvestre: A Memoir. Journal of Clinical Biochemistry and Nutrition. Pharmacology and historical review. — PubMed
- Nahas R, Moher M (2009). Complementary and alternative medicine for the treatment of type 2 diabetes. Canadian Family Physician. Practice-oriented review including gymnema. — PubMed
- Persaud SJ et al. (1999). Gymnema sylvestre stimulates insulin release in vitro by increased membrane permeability. Journal of Endocrinology. Beta-cell insulin secretion mechanism. — PubMed
- Yeh GY et al. (2003). Systematic review of herbs and dietary supplements for glycemic control in diabetes. Diabetes Care. Includes gymnema among the herbs with credible evidence. — PubMed
- Khan F et al. (2019). Gymnema sylvestre extract reverses insulin resistance and ameliorates dyslipidemia in high-fat-diet-induced obese rats. Saudi Journal of Biological Sciences. Modern mechanistic study. — PubMed
- Pothuraju R et al. (2014). A systematic review of Gymnema sylvestre in obesity and diabetes management. Journal of the Science of Food and Agriculture. — PubMed
- Al-Romaiyan A et al. (2010). A novel Gymnema sylvestre extract stimulates insulin secretion from human islets in vivo and in vitro. Phytotherapy Research. Human islet preparation evidence for the insulin-secretion mechanism. — PubMed
PubMed Topic Searches
- PubMed: Gymnema sylvestre diabetes
- PubMed: GS4 HbA1c
- PubMed: gymnema beta-cell regeneration
- PubMed: gymnema vs sulfonylurea
- PubMed: gymnema insulin resistance
Connections
- Gymnema Overview
- Gymnema Benefits Hub
- Gymnema for Sugar Cravings
- Gymnema for Weight Loss
- Gymnema for Cholesterol
- Berberine
- Cinnamon
- Bitter Melon
- Fenugreek
- Chromium
- Diabetes
- Insulin Resistance
- HbA1c
- Fasting Insulin
- Blood Sugar Control
- Metformin — the first-line antidiabetic gymnema is most often stacked with, since their mechanisms are largely orthogonal.