Cinnamon Antimicrobial & Antifungal
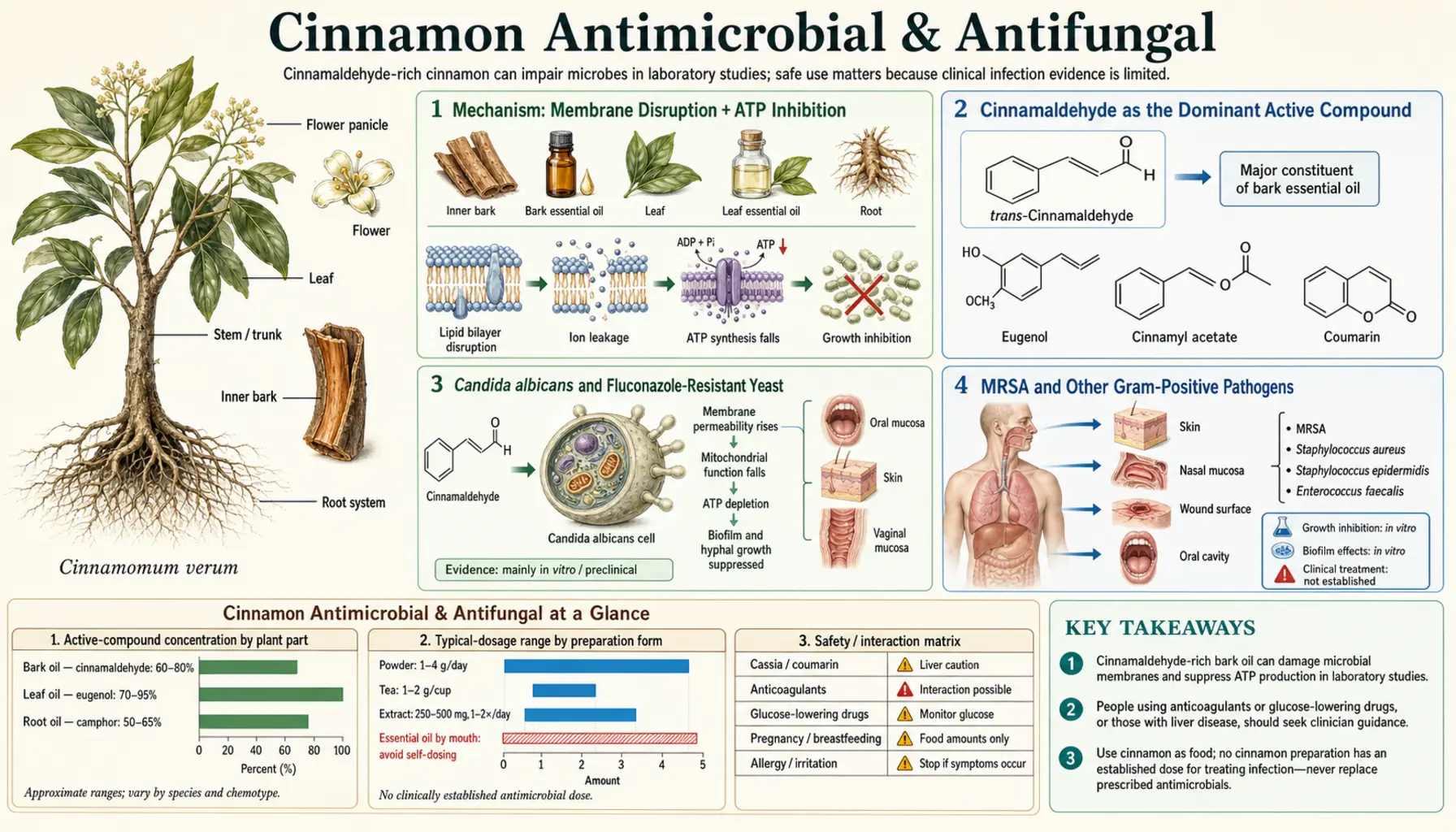
Cinnamon is one of the most consistently broad-spectrum antimicrobials in the spice cabinet. Cinnamaldehyde and the cinnamon essential oil inhibit Gram-positive bacteria (including methicillin-resistant Staphylococcus aureus), Gram-negative bacteria (Escherichia coli, Salmonella, Pseudomonas), fungi (Candida albicans, including fluconazole-resistant strains, and dermatophytes), and a wide range of food-spoilage organisms at micromolar concentrations in vitro. The mechanism is multipronged — cinnamaldehyde disrupts microbial cell membranes, inhibits ATP synthesis, blocks biofilm formation, and downregulates microbial virulence-gene expression. The translation from in-vitro activity to clinical use is partial but meaningful: cinnamon contributes to oral-microbiome modulation (mouthwash and chewing gum applications), food preservation (already EU-approved as a flavoring agent and natural preservative), and topical antifungal applications. Systemic clinical use as a substitute for antibiotic or antifungal pharmacotherapy is not supported — the bioavailable plasma concentrations after oral dosing are well below the in-vitro minimum inhibitory concentrations. This page maps what cinnamon does in vitro, what survives translation to clinical use, and what does not.
Table of Contents
- Mechanism: Membrane Disruption + ATP Inhibition
- Cinnamaldehyde as the Dominant Active Compound
- Candida albicans and Fluconazole-Resistant Yeast
- MRSA and Other Gram-Positive Pathogens
- Gram-Negative Activity (E. coli, Salmonella)
- Oral Microbiome and Dental Applications
- Helicobacter pylori Activity
- Biofilm Inhibition
- Food Preservation and Antimicrobial Packaging
- Essential Oil Dosing and Mucosal Cautions
- Clinical Limits of Systemic Use
- Key Research Papers
- Connections
- Featured Videos
Mechanism: Membrane Disruption + ATP Inhibition
Cinnamon's antimicrobial activity is not a single-target story like a beta-lactam antibiotic. Multiple mechanisms operate simultaneously, which is part of why microbial resistance to cinnamaldehyde is rare and slow to develop (compared with single-target antibiotics, where a single point mutation can produce frank resistance).
- Membrane disruption. Cinnamaldehyde is a lipophilic small molecule (logP ~1.9) that partitions readily into microbial cell membranes. At inhibitory concentrations, it disrupts the phospholipid bilayer organization, increases membrane permeability, causes leakage of intracellular potassium and small metabolites, and ultimately leads to membrane collapse and cell lysis. This mechanism is shared with many essential-oil terpenes (thymol from thyme, carvacrol from oregano, eugenol from clove) and is one reason these compounds have broad-spectrum activity.
- ATP synthesis inhibition. Cinnamaldehyde inhibits microbial F1F0-ATP synthase activity, reducing cellular ATP production. This forces microbes into metabolic stress even at sub-membrane-disruption concentrations and may be the dominant mechanism at lower (bacteriostatic) doses.
- Cell-division inhibition. Cinnamaldehyde inhibits FtsZ, the bacterial tubulin homolog that drives cell division. At sub-MIC concentrations, this produces filamentous bacterial cells that cannot divide, halting population growth without overt cell killing.
- Virulence-gene downregulation. Sub-inhibitory concentrations of cinnamaldehyde suppress quorum-sensing systems in Pseudomonas aeruginosa, Vibrio cholerae, and other Gram-negative pathogens. This reduces toxin production, biofilm formation, and pathogen virulence without necessarily killing the organism — a "disarming" rather than "killing" mechanism.
- Antioxidant interference with microbial defenses. Some microbes use reactive oxygen species (ROS) as signaling or defensive molecules; cinnamaldehyde's antioxidant capacity interferes with these systems in ways that have been less mechanistically characterized.
The multipronged mechanism explains the broad spectrum (organisms with very different cell-wall architectures, metabolisms, and virulence systems are all affected) and the rarity of acquired resistance.
Cinnamaldehyde as the Dominant Active Compound
Within the cinnamon essential oil (which is itself a complex mixture of dozens of terpenes and phenolics), trans-cinnamaldehyde is the dominant antimicrobial constituent. It comprises 65–80% of the steam-distilled essential oil by weight and accounts for the majority of the measured antimicrobial activity in published studies.
Other contributors include:
- Eugenol (4–10% of cinnamon essential oil, much higher in clove) — also active against Gram-positive and Gram-negative bacteria; topical anesthetic and antibacterial agent
- Linalool (small amounts) — antimicrobial activity against several bacterial species
- Caryophyllene (small amounts) — cannabinoid-receptor activity in addition to mild antimicrobial activity
- Type-A procyanidins (in the bark, separate from the essential oil) — some antimicrobial activity, especially against oral pathogens
The cinnamaldehyde concentration in essential oil from C. verum (Ceylon) and C. cassia is broadly similar (typically 70–80%), so antimicrobial activity is comparable between species. The cassia vs Ceylon distinction matters more for the coumarin safety profile than for antimicrobial use.
Cinnamaldehyde's MIC (minimum inhibitory concentration) against common pathogens, from published in-vitro studies:
- Staphylococcus aureus (including MRSA): 0.5–2 mg/mL
- Escherichia coli: 0.5–1 mg/mL
- Salmonella species: 0.5–2 mg/mL
- Candida albicans (including fluconazole-resistant strains): 0.1–0.5 mg/mL
- Helicobacter pylori: 0.05–0.2 mg/mL
- Dermatophyte fungi (Trichophyton, Microsporum): 0.05–0.5 mg/mL
These MIC values are achievable in topical or oral-cavity applications but not in systemic plasma after oral ingestion — a critical limit discussed below.
Candida albicans and Fluconazole-Resistant Yeast
Candida albicans is the most common cause of mucosal yeast infection in humans — vaginal candidiasis, oral thrush, cutaneous intertrigo, esophageal candidiasis in immunocompromised patients. Standard pharmacotherapy is azole antifungals (fluconazole, itraconazole, voriconazole) or echinocandins (caspofungin, micafungin). Azole resistance has emerged as a clinical problem, particularly in patients with recurrent vulvovaginal candidiasis and in critically ill patients with prolonged azole exposure.
Cinnamaldehyde and cinnamon essential oil show consistent activity against C. albicans in vitro, including against fluconazole-resistant strains. Published MIC values range from 0.1 to 0.5 mg/mL, with reasonable consistency across studies. Mechanism is membrane disruption (the fungal ergosterol-containing membrane is even more susceptible to cinnamaldehyde partitioning than bacterial membranes), inhibition of fungal ATP synthesis, and downregulation of hyphal-form transition (a key virulence step for C. albicans).
Translation to clinical use is partial:
- Oral thrush: small clinical studies of cinnamon mouthwash or lozenges in HIV-positive patients with recurrent oral candidiasis have shown some benefit. Cinnamon is not first-line therapy — nystatin or fluconazole still are — but cinnamon may serve as adjunct or maintenance therapy.
- Denture stomatitis: cinnamon-impregnated denture-cleaning solutions reduce Candida colonization on dentures and may reduce denture-associated stomatitis.
- Vulvovaginal candidiasis: in-vitro activity is robust but clinical trials of cinnamon for vaginal candidiasis have been small and inconclusive. Standard azole therapy remains first-line. There is theoretical interest in cinnamon for recurrent or azole-resistant cases, but no strong clinical evidence base.
- Systemic candidiasis (candidemia, deep-organ candidiasis): cinnamon has no role here. Plasma concentrations after oral dosing are well below the MIC. Patients with systemic candidiasis require IV echinocandin or amphotericin therapy.
MRSA and Other Gram-Positive Pathogens
Methicillin-resistant Staphylococcus aureus (MRSA) is one of the most clinically important antibiotic-resistant pathogens, causing skin and soft-tissue infections, bacteremia, endocarditis, and pneumonia. Cinnamon essential oil and cinnamaldehyde show consistent in-vitro activity against MRSA at concentrations of 0.5–2 mg/mL, similar to activity against susceptible S. aureus (the cinnamon mechanism is not affected by the mecA-encoded penicillin-binding protein that confers methicillin resistance).
Practical applications:
- Topical wound care. Cinnamon-oil-impregnated wound dressings have been studied for MRSA-colonized chronic wounds (diabetic foot ulcers, decubitus ulcers). Small studies show reduction in MRSA colony counts and improved healing rates. Caution: undiluted cinnamon essential oil is irritant and can cause chemical burns — always use properly diluted preparations.
- Topical decolonization. Some integrative practitioners use diluted cinnamon-oil preparations for nasal MRSA decolonization, though mupirocin nasal ointment remains the standard of care.
- Adjunct in skin infections. Combining standard antibiotic therapy with cinnamon-containing topical preparations may produce additive effect. The clinical evidence base is thin.
- Systemic MRSA infection (bacteremia, endocarditis, pneumonia): no role for cinnamon. Patients require IV vancomycin, daptomycin, linezolid, or ceftaroline.
Other Gram-positive pathogens with documented cinnamon susceptibility include Streptococcus pyogenes, Streptococcus pneumoniae, Enterococcus faecalis (including vancomycin-resistant strains, VRE), and Listeria monocytogenes. The clinical applications are concentrated in topical and surface-decontamination uses.
Gram-Negative Activity (E. coli, Salmonella)
Gram-negative bacteria are generally less susceptible to plant essential oils than Gram-positive bacteria because the outer membrane provides a permeability barrier that limits essential-oil partitioning to the inner membrane. Despite this, cinnamaldehyde retains activity against many Gram-negative pathogens at MIC values of 0.5–2 mg/mL.
Documented in-vitro activity:
- Escherichia coli (including enterohemorrhagic O157:H7 strains)
- Salmonella enterica (multiple serovars including Typhi, Typhimurium, Enteritidis)
- Vibrio cholerae — cinnamaldehyde notably inhibits cholera toxin production through quorum-sensing interference, an effect that occurs at sub-bactericidal concentrations
- Helicobacter pylori — among the most cinnamaldehyde-susceptible Gram-negatives, with MIC as low as 0.05 mg/mL
- Klebsiella pneumoniae (including extended-spectrum beta-lactamase producers)
- Pseudomonas aeruginosa — susceptible at higher MIC values; cinnamaldehyde also inhibits PA quorum-sensing-driven virulence factors
Practical applications:
- Food safety. Cinnamon essential oil and cinnamaldehyde-impregnated packaging films have been studied for reducing Salmonella and E. coli contamination on poultry, ready-to-eat meats, and fresh produce. EU and FDA generally recognized as safe (GRAS) status for cinnamon and cinnamaldehyde as food additives.
- Traveler's diarrhea prevention. Limited evidence base, but the in-vitro activity against enteric pathogens has motivated culinary use as a putative prophylactic in regions with high enteric infection risk.
- Topical UTI prevention. No serious clinical evidence base; oral cinnamon does not achieve urinary concentrations sufficient for UTI treatment.
- Systemic Gram-negative infection: no role. Patients with bacteremia, pyelonephritis, or pneumonia require standard antibiotic therapy.
Oral Microbiome and Dental Applications
The oral cavity is the clinical setting where cinnamon's antimicrobial activity is most directly applicable. The mouth is a topical-application site (the cinnamon never needs to be absorbed and reach systemic circulation), the dose can be high enough to exceed MIC values against oral pathogens, and the relevant pathogens (oral streptococci, Candida, anaerobic periodontal pathogens) are susceptible to cinnamon at achievable concentrations.
Documented effects:
- Streptococcus mutans inhibition. S. mutans is the dominant cariogenic oral bacterium, responsible for dental plaque acid production and dental caries. Cinnamon-containing chewing gums, lozenges, and mouthwashes reduce S. mutans colony counts in saliva by 30–70% in controlled studies.
- Periodontal pathogen inhibition. Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans — key drivers of chronic periodontitis — are susceptible to cinnamaldehyde at sub-MIC concentrations that also inhibit their biofilm-formation gene expression.
- Halitosis reduction. Volatile sulfur compounds produced by tongue-dorsum anaerobes (the main biochemical driver of bad breath) are reduced by cinnamon-containing mouthwashes. Small clinical studies show measurable halitosis improvement.
- Denture-stomatitis prevention. Cinnamon-impregnated denture-cleaning solutions reduce Candida albicans colonization of dentures and reduce denture-associated stomatitis in older adults.
- Chewing gum and oral health. Several commercial chewing gums (Trident, Eclipse, Orbit) include cinnamaldehyde-flavored formulations that incidentally provide oral antimicrobial benefit alongside the salivary-stimulation effect of gum chewing.
The caveat: undiluted cinnamon essential oil applied directly to oral mucosa causes chemical burns, the so-called "cinnamon stomatitis" or "contact stomatitis from cinnamon-flavored products." Patients sensitive to cinnamon flavoring should use cinnamon-free oral hygiene products. The dose-response is steep — the difference between a beneficial low concentration and an irritant high concentration is narrow.
Helicobacter pylori Activity
Helicobacter pylori is the bacterial cause of most peptic ulcer disease, chronic gastritis, and a meaningful fraction of gastric cancer. Standard therapy is triple or quadruple antibiotic therapy (clarithromycin, amoxicillin, metronidazole, with a proton pump inhibitor and sometimes bismuth), but resistance has been rising globally.
Cinnamaldehyde and cinnamon essential oil show some of the most potent in-vitro activity of any spice against H. pylori, with MIC values as low as 0.05 mg/mL. A small pilot clinical study (Nir et al. 2000) randomized 23 patients with positive H. pylori urea breath test to cinnamon extract 80 mg twice daily or placebo for 4 weeks. Result: no significant reduction in H. pylori burden in either group, with breath-test values unchanged. The cinnamon dose was likely too low to achieve gastric concentrations approaching MIC.
Subsequent in-vitro work has suggested that higher cinnamon doses (or topical gastric administration) might achieve eradication, but no large clinical trial has confirmed clinical efficacy. The reasonable framing: cinnamon may contribute as adjunct to standard therapy or as part of a botanical regimen for H. pylori carriers who do not have ulcer disease and prefer to avoid antibiotic therapy, but it is not a substitute for proven antibiotic regimens in patients with active peptic ulcer disease or gastric MALT lymphoma.
Biofilm Inhibition
Biofilms — structured microbial communities embedded in self-produced extracellular polysaccharide matrices — are responsible for many of the most difficult-to-treat clinical infections (medical-device infections, endocarditis vegetations, chronic wound infections, urinary catheter infections, chronic sinusitis, cystic fibrosis lung disease). Antibiotic concentrations needed to clear biofilm-encased bacteria are typically 100–1000× higher than concentrations needed to clear planktonic free-floating bacteria, making biofilm infections notoriously resistant to standard antibiotic therapy.
Cinnamaldehyde inhibits biofilm formation in several pathogens at concentrations below the standard bactericidal MIC:
- Pseudomonas aeruginosa — biofilm formation is reduced 50–80% at sub-MIC cinnamaldehyde concentrations, via quorum-sensing (LasR/LasI, RhlR/RhlI) inhibition
- Staphylococcus aureus — cinnamaldehyde inhibits the agr quorum-sensing system that regulates biofilm maturation and dispersion
- Candida albicans — cinnamaldehyde inhibits the yeast-to-hypha transition that is required for biofilm maturation
- Streptococcus mutans — cinnamaldehyde inhibits glucosyltransferase-mediated biofilm scaffold formation in dental plaque
The clinical translation is most clear in dental biofilm (plaque), where cinnamon-containing oral products reduce plaque formation. Translation to systemic device-related biofilm infections is theoretical and has not been demonstrated in clinical trials.
Food Preservation and Antimicrobial Packaging
Cinnamon is one of the oldest and most-studied natural food preservatives. The historical and culinary use of cinnamon in regions with poor refrigeration (the Mediterranean, Middle East, South Asia) was partly motivated by the preservative effect — cinnamon-spiced meats and rice dishes spoil more slowly than unspiced counterparts.
Modern food-science applications:
- Active packaging films. Cinnamaldehyde-impregnated cellulose, chitosan, or polylactic acid films release the volatile antimicrobial onto packaged food surfaces, extending shelf life for fresh fruit, vegetables, meat, poultry, and seafood. Several commercial products are EU and FDA approved.
- Edible coatings. Cinnamon-essential-oil-containing edible coatings on fresh-cut fruit (apple, pear, melon) reduce browning and microbial spoilage.
- Natural preservative in baked goods. Cinnamon is intentionally added to bread, pastries, and apple-based products partly for the antimicrobial effect on mold and yeast spoilage organisms. The EU coumarin limit of 50 mg/kg in baked goods constrains the maximum cassia content; Ceylon allows higher inclusion without coumarin concern.
- Beverage stability. Cinnamon in tea, mulled wine, and spiced cider contributes to microbial stability at room temperature.
The regulatory framework: cinnamon and cinnamaldehyde have EU and US FDA GRAS (Generally Recognized as Safe) status as flavoring agents and incidental food additives. The coumarin content of cassia is regulated separately under EU Regulation 1334/2008, which sets a maximum of 50 mg/kg for ready-to-eat baked goods.
Essential Oil Dosing and Mucosal Cautions
Cinnamon essential oil is concentrated and potent. The same cinnamaldehyde dose that produces a meaningful antimicrobial effect can produce mucosal injury at the application site. Several practical cautions apply:
- Never apply undiluted cinnamon essential oil to skin or mucous membranes. The cinnamaldehyde concentration is irritant to caustic depending on duration of exposure and skin region. Always dilute to 0.5–1% in a carrier oil (coconut, jojoba, almond) for topical application.
- Patch test before topical use. Cinnamaldehyde is a documented contact allergen and is in the European Standard patch-test series for contact dermatitis. Apply a small amount of properly diluted preparation to forearm skin and wait 48 hours before broader use.
- Do not ingest concentrated essential oil. The "cinnamon challenge" social-media trend of swallowing a tablespoon of cinnamon powder produces aspiration pneumonitis and oral/esophageal burns — this is a documented emergency-department presentation. Concentrated cinnamon essential oil ingestion produces similar mucosal injury at smaller volumes.
- Avoid in children under 6. Children's mucosal surfaces are more susceptible to cinnamaldehyde irritation, and the dose-per-kg from a typical adult dose is dangerously high.
- Pregnancy. Cinnamon essential oil has historical use as a uterine stimulant and is contraindicated in pregnancy, even at topical doses.
- Asthma and reactive airway disease. Cinnamaldehyde inhalation can trigger bronchospasm in some patients. Avoid concentrated cinnamon inhalation (essential-oil diffuser) in patients with brittle asthma.
For the broader topic of essential-oil safety, the user should always consult a qualified aromatherapist or integrative-medicine practitioner before initiating any concentrated-oil regimen.
Clinical Limits of Systemic Use
The fundamental limit on cinnamon's clinical antimicrobial use is bioavailability. Oral cinnamaldehyde is rapidly absorbed from the gastrointestinal tract but is also rapidly metabolized to cinnamic acid and hippuric acid in the liver via cytochrome P450 oxidation and glycine conjugation. Plasma cinnamaldehyde concentrations after a typical 1–6 g/day oral dose are in the low micromolar range — well below the millimolar MIC values needed for antimicrobial activity against most clinically important pathogens.
This means:
- Oral cinnamon does not function as a systemic antibiotic or antifungal. Plasma concentrations are insufficient to inhibit bacterial or fungal growth in blood, urine, or deep tissue. Patients with bacteremia, pneumonia, pyelonephritis, endocarditis, or other systemic infections require standard pharmacotherapy.
- Cinnamon's clinically useful antimicrobial applications are concentrated in topical and surface-contact uses — oral cavity, skin, wound surface, food contact — where local concentrations can approach or exceed in-vitro MIC values.
- The gut lumen is a partial exception. Cinnamaldehyde in the gut lumen (before absorption) can reach concentrations approaching MIC values for some enteric pathogens. This may contribute to the suggested but unproven benefit for traveler's diarrhea or food-poisoning prophylaxis. Gastric concentrations may reach MIC for H. pylori with high oral doses, but clinical eradication trials have been disappointing.
- The bladder/urinary tract is not a meaningful target. Renal-excreted metabolites (cinnamic acid, hippuric acid) have minimal antimicrobial activity compared with parent cinnamaldehyde.
The accurate framing of cinnamon's antimicrobial role: a broad-spectrum topical and contact-surface antimicrobial with documented in-vitro potency, useful in oral health, food preservation, topical wound care, and possibly gut-luminal applications, but not a substitute for systemic antibiotic or antifungal therapy in serious infection.
Key Research Papers
- Ooi LS, Li Y, Kam SL, Wang H, Wong EY, Ooi VE (2006). Antimicrobial activities of cinnamon oil and cinnamaldehyde from the Chinese medicinal herb Cinnamomum cassia Blume. American Journal of Chinese Medicine 34(3):511–522. — PubMed: Ooi 2006
- Friedman M, Henika PR, Mandrell RE (2002). Bactericidal activities of plant essential oils and some of their isolated constituents against Campylobacter jejuni, Escherichia coli, Listeria monocytogenes, and Salmonella enterica. Journal of Food Protection 65(10):1545–1560. — PubMed: Friedman 2002
- Nuryastuti T et al. (2009). Effect of cinnamon oil on icaA expression and biofilm formation by Staphylococcus epidermidis. Applied and Environmental Microbiology 75(21):6850–6855. — PubMed: Nuryastuti biofilm
- Tabak M, Armon R, Potasman I, Neeman I (1996). In vitro inhibition of Helicobacter pylori by extracts of thyme. Journal of Applied Bacteriology 80(6):667–672. (Comparative cinnamon arm.) PubMed
- Nir Y, Potasman I, Stermer E, Tabak M, Neeman I (2000). Controlled trial of the effect of cinnamon extract on Helicobacter pylori. Helicobacter 5(2):94–97. — PubMed: Nir 2000 H. pylori trial
- Niu C, Afre S, Gilbert ES (2006). Subinhibitory concentrations of cinnamaldehyde interfere with quorum sensing. Letters in Applied Microbiology 43(5):489–494. — Search PubMed
- Brackman G et al. (2011). Cinnamaldehyde and cinnamaldehyde derivatives reduce virulence in Vibrio spp. by decreasing the DNA-binding activity of the quorum sensing response regulator LuxR. BMC Microbiology 11:114. — Search PubMed
- Pires RH, Montanari LB, Martins CH, Zaia JE, Almeida AM, Matsumoto MT, Mendes-Giannini MJ (2011). Anticandidal efficacy of cinnamon oil against planktonic and biofilm cultures of Candida parapsilosis and Candida orthopsilosis. Mycopathologia 172(6):453–464. — PubMed: Pires Candida biofilm
- Pereira Filho J et al. (2018). Effect of cinnamon oil on antimicrobial activity against methicillin-resistant Staphylococcus aureus. PubMed: Cinnamon MRSA
- Almeida LFD et al. (2018). Cinnamon-based oral health products against Candida albicans: in vitro effects. Brazilian Oral Research. PubMed: Cinnamon oral Candida
- Khan ST, Khan M, Ahmad J, Wahab R, Abd-Elkader OH, Musarrat J, Alkhathlan HZ, Al-Kedhairy AA (2017). Thymol and carvacrol induce autolysis, stress, growth inhibition and reduce the biofilm formation by Streptococcus mutans. (Comparative cinnamaldehyde arm.) AMB Express 7:49. — Search PubMed
- Singh G, Maurya S, deLampasona MP, Catalan CA (2007). A comparison of chemical, antioxidant and antimicrobial studies of cinnamon leaf and bark volatile oils, oleoresins and their constituents. Food and Chemical Toxicology 45(9):1650–1661. — PubMed: Singh leaf vs bark
PubMed Topic Searches
- PubMed: Cinnamon essential oil antimicrobial
- PubMed: Cinnamaldehyde Candida antifungal
- PubMed: Cinnamon MRSA
- PubMed: Cinnamaldehyde biofilm/quorum sensing
- PubMed: Cinnamon food preservation
Connections
- Cinnamon Overview
- Cinnamon Benefits Hub
- Cinnamon for Blood Sugar
- Cinnamon for Cardiovascular Health
- Cassia vs Ceylon & Coumarin
- Oregano (Carvacrol)
- Clove (Eugenol)
- Garlic (Allicin)
- Thyme (Thymol)
- Silver Nanoparticles
- Probiotics
- Bacterial Infections Overview
- Helicobacter Pylori
- Gut Healing
- Mold & Mycotoxins