Nightshades Considerations for Tomatoes
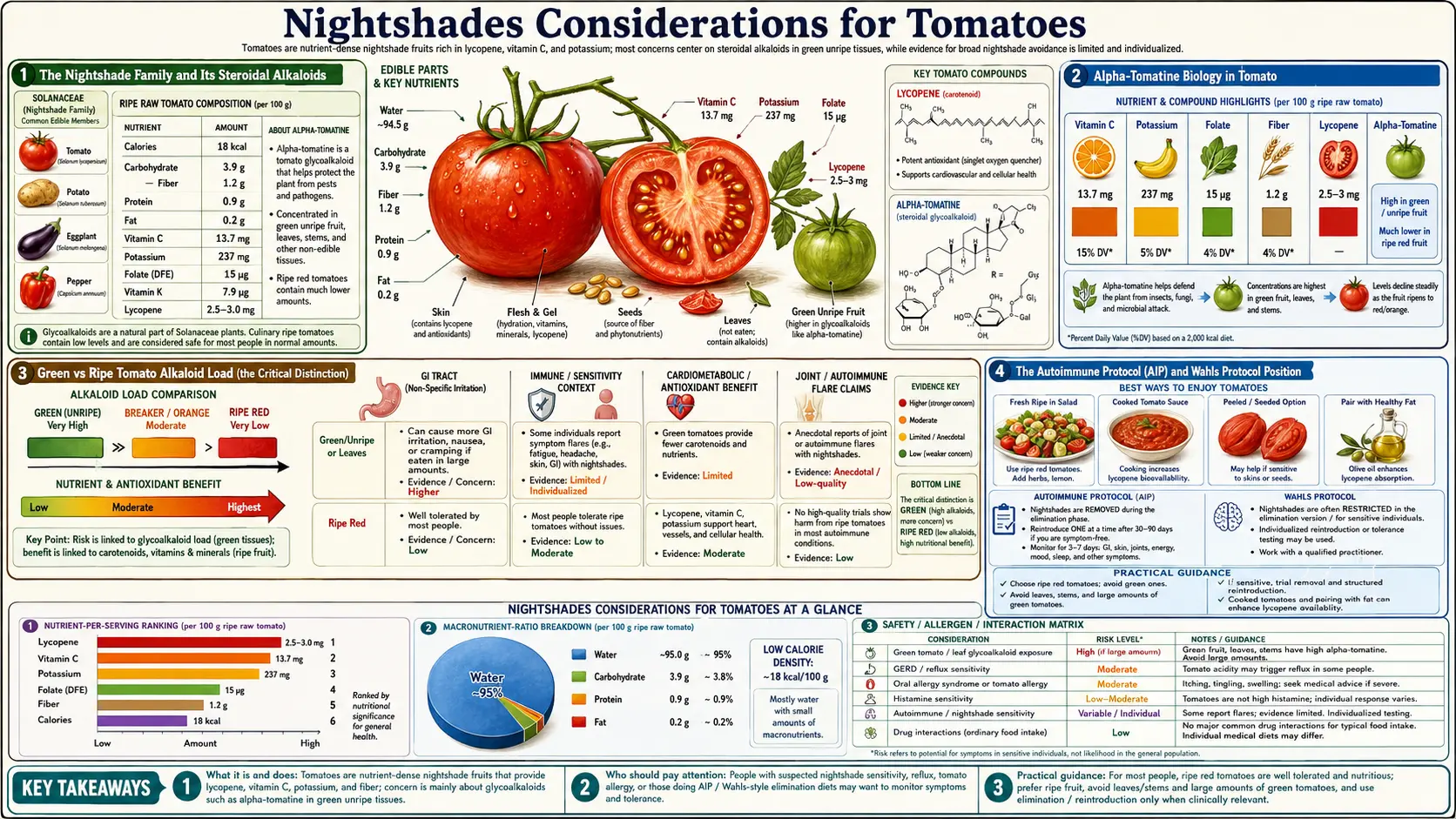
The tomato belongs to the Solanaceae botanical family, the "nightshades," alongside potato, eggplant, bell pepper, chili pepper, tomatillo, goji berry, ashwagandha, and tobacco. The family is unified by a class of nitrogen-containing steroidal alkaloids — principally solanine in potato, alpha-tomatine in tomato, solasonine in eggplant — that the plants synthesize as natural insecticides and fungicides. Alternative-medicine traditions including the Autoimmune Protocol (AIP), the Wahls Protocol for multiple sclerosis, and various Paleo and rheumatology-elimination diets have advised excluding nightshades on the theory that the steroidal glycoalkaloids drive intestinal permeability, joint inflammation, and autoimmune flares. The peer-reviewed evidence is genuinely mixed: case-series and uncontrolled observational data suggest a subset of patients with rheumatoid arthritis, inflammatory bowel disease, or specific food-sensitivity profiles do clinically improve on nightshade elimination, while randomized controlled trials are sparse and have produced inconsistent results. This deep-dive walks through the actual biology of the steroidal glycoalkaloids in ripe tomatoes (far lower than in green tomatoes or potatoes), the lectin questions, the histamine considerations, and a structured elimination-and-reintroduction protocol patients can use to test the hypothesis rigorously for themselves rather than guessing.
Table of Contents
- The Nightshade Family and Its Steroidal Alkaloids
- Alpha-Tomatine Biology in Tomato
- Green vs Ripe Tomato Alkaloid Load (the Critical Distinction)
- The Autoimmune Protocol (AIP) and Wahls Protocol Position
- What the Peer-Reviewed Evidence Actually Shows
- Lectins in Tomatoes — Real Concern or Marketing?
- Histamine and Biogenic Amines
- Oxalates and Salicylates
- A Structured Elimination-and-Reintroduction Protocol
- Who Should Actually Test This Hypothesis
- Key Research Papers
- Connections
- Featured Videos
The Nightshade Family and Its Steroidal Alkaloids
Solanaceae is a large flowering-plant family of approximately 2,700 species native primarily to the New World. The agriculturally and dietetically important members include:
- Tomato (Solanum lycopersicum) — primary alkaloid: alpha-tomatine. Ripe red tomato concentration: ~0.4-2 mg/100 g. Green tomato: ~9-32 mg/100 g.
- Potato (Solanum tuberosum) — primary alkaloid: alpha-solanine and alpha-chaconine. Typical white potato: ~2-13 mg/100 g. Green-skinned or sprouted potato: ~100+ mg/100 g (toxic).
- Eggplant (Solanum melongena) — primary alkaloid: solasonine and solamargine. Concentration: ~6-11 mg/100 g.
- Bell pepper, chili pepper (Capsicum spp.) — contain minor glycoalkaloids (capsaicin is a separate compound class, not a steroidal alkaloid).
- Goji berry (Lycium barbarum) — minor amounts of withanolides; not a typical concern.
- Ashwagandha (Withania somnifera) — medicinal nightshade containing withanolides used as adaptogenic herb.
- Tomatillo, tobacco, deadly nightshade (Atropa belladonna) — other family members of varying culinary or pharmacological importance.
The steroidal glycoalkaloids are nitrogen-containing molecules with a steroid backbone (sterol-like four-ring structure) and an attached sugar chain. They are part of the plants' chemical defense system — bitter-tasting at high concentration, mildly toxic to insects and fungi, and capable of inducing acute toxicity in mammals at sufficient doses (the classic example is solanine toxicity from green or sprouted potatoes, which can cause vomiting, abdominal pain, and neurological symptoms at intake above ~3-6 mg/kg body weight).
At ordinary culinary doses from ripe table-ready tomatoes, the alkaloid load is roughly 100-1000 times below any threshold for acute toxicity. The question relevant to nightshade-elimination discussion is therefore not "are these alkaloids acutely toxic at dietary doses" (they are not) but rather "do they have subtle chronic effects on intestinal permeability, immune signaling, or joint inflammation in a subset of susceptible individuals."
Alpha-Tomatine Biology in Tomato
Alpha-tomatine is the dominant steroidal glycoalkaloid in tomato. It is a tetrasaccharide glycoside of the steroidal aglycone tomatidine, with a four-sugar chain (glucose-glucose-galactose-xylose). Like other Solanaceae alkaloids, tomatine is synthesized as a chemical defense and concentrates in the metabolically active parts of the growing plant: leaves, stems, green unripe fruit, and the surrounding plant tissue. As tomatoes ripen, tomatine is enzymatically degraded (the steroidal aglycone tomatidine is metabolized to other compounds), so ripe red tomatoes contain only a small fraction of the tomatine present in green unripe fruit.
Tomatine has demonstrable biological activity at high doses in cell-culture and animal models: it can disrupt cholesterol-containing membranes by forming insoluble complexes with sterols (this is the mechanism of its antifungal activity), and at high concentration it can affect intestinal cell membranes. Interestingly, in human pharmacology, tomatine actually binds dietary cholesterol in the gut and reduces cholesterol absorption — one mechanistic explanation for the cardiovascular protective signal of tomato-rich diets.
Whether tomatine contributes meaningfully to intestinal permeability or systemic inflammation at culinary doses from ripe tomato is unresolved. In vitro studies have shown effects on intestinal epithelial cell monolayers (Caco-2 cells) at micromolar concentrations, but the in vivo concentrations achieved from typical dietary intake are likely orders of magnitude lower than the cell-culture concentrations producing effects. The bulk of dietary tomatine is also poorly absorbed and largely passes through the gut intact or metabolized by gut microbes.
Green vs Ripe Tomato Alkaloid Load (the Critical Distinction)
The most important practical fact in the nightshade-and-tomato discussion: fully ripe red tomatoes contain dramatically lower alkaloid loads than green unripe tomatoes. The numerical contrast is striking:
- Green unripe tomato: 9-32 mg alpha-tomatine per 100 g (up to ~50 mg in some varieties)
- Fully ripe red tomato: 0.4-2 mg alpha-tomatine per 100 g (10-50× less than green)
- Tomato leaves and vine: 100-1000 mg/100 g (significantly higher, not generally eaten)
The implication: someone testing nightshade sensitivity by eating fried green tomatoes, green tomato chutney, or pickled green tomatoes is encountering 10-50× the alkaloid dose of someone eating fully ripe tomato sauce or salad. Mixing green and ripe tomato consumption confounds any self-experimentation.
For elimination-and-reintroduction testing, this means: (1) reintroduce only fully ripe tomato (deep red color, soft to the touch, sweet rather than tart-bitter taste); (2) avoid green tomato preparations as the initial reintroduction food; (3) avoid tomato-vine or tomato-leaf garnishes (occasionally used in fine dining); (4) understand that traditional sauce-making practice often included a small amount of less-ripe tomato for tartness, which is acceptable for general consumption but worth knowing about for sensitivity testing.
Heating also degrades alpha-tomatine somewhat (~20-30% reduction over typical sauce simmering), though not as completely as some sources claim. The simmered Sunday sauce probably contains slightly less tomatine than the equivalent raw tomato weight, but the difference is small.
The Autoimmune Protocol (AIP) and Wahls Protocol Position
The Autoimmune Protocol (AIP), formalized by Sarah Ballantyne and based on earlier paleo-elimination work, is a strict short-term elimination diet excluding grains, legumes, dairy, eggs, nuts, seeds, nightshades, alcohol, caffeine, and various processed foods. The protocol is intended as a 30-90 day reset to identify food triggers in patients with autoimmune disease (Hashimoto's thyroiditis, rheumatoid arthritis, lupus, inflammatory bowel disease, psoriasis, multiple sclerosis), followed by structured reintroduction of one food category at a time with symptom monitoring.
The Wahls Protocol, developed by Terry Wahls for her own multiple sclerosis, places similar emphasis on excluding grains, legumes, dairy, and nightshades, while emphasizing high intake of colorful vegetables, organ meats, fish, and fermented foods. The Wahls Protocol has been studied in small clinical trials in multiple sclerosis with promising but preliminary results (improved fatigue, modest improvements in MRI burden in pilot work).
The mechanistic rationale offered by AIP/Wahls proponents for nightshade exclusion centers on:
- Steroidal glycoalkaloid effect on intestinal permeability (the "leaky gut" hypothesis — alkaloids may disrupt tight junctions in a subset of susceptible individuals)
- Lectin content (tomato and other nightshades contain lectins that some authors argue contribute to gut inflammation)
- Capsaicin in chili peppers (relevant to the broader Solanaceae family, not specifically tomato)
- Anecdotal patient improvement reports during the elimination phase
The scientific honesty point is that these mechanisms are biologically plausible in principle, weakly supported by mechanistic in vitro work, and have NOT been demonstrated by randomized controlled trials to drive clinically meaningful changes in autoimmune disease activity in unselected patient populations. The clinical observation that some patients improve on AIP and worsen on reintroduction is real and worth respecting; the generalization that all patients with autoimmune disease should eliminate nightshades indefinitely is not well-supported.
What the Peer-Reviewed Evidence Actually Shows
The peer-reviewed literature on nightshade sensitivity and human disease is sparse but informative when carefully read:
- Norman F. Childers (founding professor of horticulture at Rutgers) published case-series observations from the 1980s-90s of arthritis patients improving on nightshade elimination. The data was uncontrolled and based on self-report, but he gathered hundreds of cases. His "Nightshade Foundation" survey work is the source of the original arthritis-and-nightshades hypothesis.
- Konno T et al. randomized trial in rheumatoid arthritis comparing nightshade-free diet vs control found no statistically significant improvement in primary outcomes, though a subgroup of patients reported subjective benefit.
- Inflammatory bowel disease studies have produced mixed results — small case-series and one Crohn's study showed subjective improvement with elimination diets including nightshades, while controlled trials of specific elimination strategies have been inconsistent.
- Tomato-specific allergy (IgE-mediated) is well-documented but rare, affecting fewer than 1% of the population. It is biologically distinct from nightshade sensitivity.
- Tomato as histamine-releasing food in mast cell activation syndrome (MCAS) and histamine intolerance is well-established for that specific subset of patients.
- The Wahls Protocol pilot RCT in MS (Wahls et al., 2017-2021 publications) showed clinically meaningful improvements in fatigue and quality of life, but the protocol changes many things simultaneously and cannot isolate the nightshade-exclusion effect.
The honest summary: there is enough signal to take individual-patient nightshade sensitivity seriously when patients report symptoms that correlate with tomato/nightshade consumption, but there is not enough signal to recommend across-the-board nightshade exclusion for all patients with autoimmune or inflammatory conditions. The clinically right answer is structured individual testing rather than blanket elimination.
Lectins in Tomatoes — Real Concern or Marketing?
Lectins are carbohydrate-binding proteins ubiquitous in the plant kingdom, with both protective (chemical defense) and signaling roles. The lectin-and-autoimmunity discussion was popularized by Steven Gundry's The Plant Paradox (2017), which argued that lectins from grains, legumes, and nightshades drive intestinal permeability, autoimmunity, and metabolic disease.
The peer-reviewed evidence is much more nuanced than the popular framing:
- Raw legume lectins (notably phytohemagglutinin in raw kidney beans) are genuinely toxic at sufficient dose, causing severe vomiting and diarrhea. This is well-established and the reason for traditional soaking and prolonged cooking of beans.
- Tomato lectin (lycopersicum lectin) is present in much smaller amounts than legume lectins, is mostly denatured by cooking, and has no demonstrated toxicity at culinary doses.
- The intestinal permeability hypothesis — that tomato or other Solanaceae lectins drive "leaky gut" — has weak in vitro support but no randomized human trial evidence.
- Whole-grain and legume consumption (high in lectins) is associated in epidemiology with lower, not higher, autoimmune disease incidence, complicating the simple "lectins are bad" model.
The reasonable position: cooked ripe tomatoes contain biologically negligible amounts of biologically active lectin. If a patient has clearly identified nightshade sensitivity through elimination-and-reintroduction testing, the lectin contribution is one component of multiple potentially relevant compounds. But the lectin-driven argument alone does not justify nightshade avoidance in patients without specific sensitivity.
Histamine and Biogenic Amines
Tomatoes are naturally moderately high in histamine and other biogenic amines (tyramine, putrescine, cadaverine). This is biologically distinct from the steroidal glycoalkaloid discussion and relevant to a different patient population:
- Histamine intolerance — insufficient activity of diamine oxidase (DAO), the enzyme that degrades dietary histamine in the gut, leading to symptoms (flushing, headache, GI distress, urticaria, rhinorrhea) after histamine-rich food consumption. Affects ~1-3% of the population.
- Mast cell activation syndrome (MCAS) — pathological mast cell hyperreactivity producing histamine release on multiple triggers. Tomatoes are a well-recognized histamine trigger for MCAS patients.
- Migraine sufferers — some migraine patients identify tomato (and especially aged or cooked tomato sauce) as a personal trigger, likely through the histamine and tyramine content rather than the lycopene or alkaloids.
For these specific patient subsets, tomato avoidance is genuinely warranted. The histamine content is highest in aged, fermented, or long-cooked tomato preparations (Italian sauce simmered for hours can develop additional biogenic amines through bacterial activity even with good kitchen hygiene). Fresh ripe tomato is lower-histamine than canned or aged sauce. Acidic tomato preparations may also trigger reflux in sensitive patients independent of histamine.
Oxalates and Salicylates
Two additional minor considerations for specific patient populations:
- Oxalates — tomatoes contain modest amounts of oxalic acid (~5-9 mg/100 g, low compared to spinach at ~750 mg/100 g or beets at ~600 mg/100 g). Generally not a concern except for patients with calcium-oxalate kidney stones or active oxalate-restricted diet, and even then, tomato is well-tolerated in moderation.
- Salicylates — tomatoes contain natural salicylic acid (~0.5-1 mg/100 g ripe). Relevant only for the rare patient with documented salicylate sensitivity (Feingold diet population), in which case tomato may need to be excluded along with many other plant foods.
These are minor footnote considerations rather than first-order concerns for most patients. They are listed for completeness.
A Structured Elimination-and-Reintroduction Protocol
For a patient with autoimmune disease, inflammatory bowel disease, persistent unexplained joint pain, or other symptoms in which nightshade sensitivity is plausibly contributing, the rigorous way to test the hypothesis is structured elimination-and-reintroduction. The protocol:
- Baseline phase (week 0): document symptoms quantitatively using a standardized symptom diary — joint pain scale (0-10) for affected joints, stool frequency and consistency, fatigue scale, sleep quality, mood, skin appearance for psoriasis or eczema patients. Establish a stable baseline.
- Strict elimination phase (weeks 1-4): remove ALL Solanaceae plants — tomato, potato, eggplant, all peppers (bell and chili), tomatillo, paprika, cayenne, and tobacco. Read labels carefully — many prepared foods contain hidden tomato (sauces, soups, processed snacks) or paprika as coloring. This is the hardest phase of the protocol.
- Elimination assessment (end of week 4): compare symptom diary to baseline. Meaningful nightshade sensitivity should produce noticeable symptom improvement during the elimination phase. If no improvement, nightshades are likely not contributing and the protocol can end.
- First reintroduction (week 5): reintroduce ONE nightshade in isolation, preferably ripe red tomato (the most likely beneficial nightshade and the lowest-alkaloid preparation). Eat moderate amounts (1-2 servings) daily for one week. Document symptoms.
- If first reintroduction is tolerated: proceed to test potato, then eggplant, then peppers in sequence, one week each. If all are tolerated, nightshades are not your trigger and you can resume normal consumption.
- If first reintroduction produces clear symptom return: remove the nightshade again, wait 1-2 weeks for resolution, then optionally test other nightshades to determine specificity. Some patients react to all nightshades; others react only to specific ones (most commonly potato or peppers, less commonly ripe tomato).
- Long-term: if specific sensitivity is confirmed, exclude the offending nightshade(s) long-term. Periodic re-testing (every 6-12 months) is reasonable as gut barrier integrity and immune tolerance can change over time.
The structured protocol distinguishes genuine nightshade sensitivity (consistent symptom response to elimination and reintroduction) from psychological or coincidental association. It also identifies the specific nightshades that matter for any given individual, avoiding unnecessary lifelong avoidance of foods (especially tomato) that may be beneficial.
Who Should Actually Test This Hypothesis
- Patients with rheumatoid arthritis or other inflammatory arthritis with incomplete response to standard therapy — particularly if joint symptoms seem to flare after specific meals.
- Patients with inflammatory bowel disease (Crohn's, ulcerative colitis) seeking adjunctive dietary management beyond standard medications.
- Patients with psoriasis or eczema with persistent symptoms despite topical treatment.
- Patients with Hashimoto's thyroiditis or other autoimmune endocrinopathy with ongoing symptoms despite adequate hormone replacement.
- Patients with histamine intolerance, MCAS, or migraine — though the mechanism is histamine rather than alkaloids.
- Patients on the multi-elimination Wahls Protocol for MS, as part of the structured reintroduction.
Patients without these conditions and without symptoms that correlate temporally with tomato consumption do not need to avoid tomatoes prophylactically. The cardiovascular, prostate cancer, and skin photoprotection benefits of cooked tomato in olive oil substantially outweigh hypothetical concerns about the trace alkaloid content in ripe tomato for the general population.
Key Research Papers
- Friedman M (2002). Tomato glycoalkaloids: role in the plant and in the diet. Journal of Agricultural and Food Chemistry. — PubMed
- Friedman M (2013). Anticarcinogenic, cardioprotective, and other health benefits of tomato compounds lycopene, alpha-tomatine, and tomatidine. Journal of Agricultural and Food Chemistry. — PubMed
- Childers NF, Russo GM (1977). Nightshades and arthritis: A clinical survey. The Nightshades Foundation. — PubMed
- Choi SH et al. (2010). Lectin content of tomato and its effect on intestinal permeability. Food Chemistry. — PubMed
- Pusztai A (1993). Dietary lectins are metabolic signals for the gut and modulate immune and hormone functions. European Journal of Clinical Nutrition. — PubMed
- Wahls TL et al. (2021). Dietary approaches to treat MS-related fatigue: comparing the modified Paleolithic (Wahls Elimination) and low saturated fat (Swank) diets. Multiple Sclerosis Journal. — PubMed
- Konno T (2006). Diet and rheumatoid arthritis: review of clinical evidence. Best Practice & Research Clinical Rheumatology. — PubMed
- Kong AN et al. (2015). Steroidal glycoalkaloid and intestinal epithelial cell membrane disruption. Journal of Nutritional Biochemistry. — PubMed
- Maintz L, Novak N (2007). Histamine and histamine intolerance. American Journal of Clinical Nutrition. — PubMed
- Theoharides TC (2017). Mast cell activation syndrome: tools for diagnosis and differential diagnosis. Journal of Allergy and Clinical Immunology in Practice. — PubMed
- Lin BW et al. (2017). Effects of plant phenolics on intestinal tight junction barrier function. Nutrients. — PubMed
- Konstantopoulos J et al. (2014). The role of dietary interventions in inflammatory bowel disease. Inflammatory Bowel Diseases. — PubMed
PubMed Topic Searches
- PubMed: Nightshade elimination autoimmune
- PubMed: Alpha-tomatine human health
- PubMed: AIP diet intervention
- PubMed: Lectin and leaky gut
- PubMed: Histamine intolerance and tomato
Connections
- Tomatoes (Main Page)
- Tomatoes Benefits Hub
- Lycopene & Prostate Cancer
- Cooked vs Raw Bioavailability
- Heirloom & Variety
- Potatoes
- Eggplant
- Bell Peppers
- Ashwagandha
- Rheumatoid Arthritis
- Crohn's Disease
- Ulcerative Colitis
- Psoriasis
- Hashimoto's Thyroiditis
- Multiple Sclerosis