Herring Vitamin D and B12 — A Dual Micronutrient Vehicle
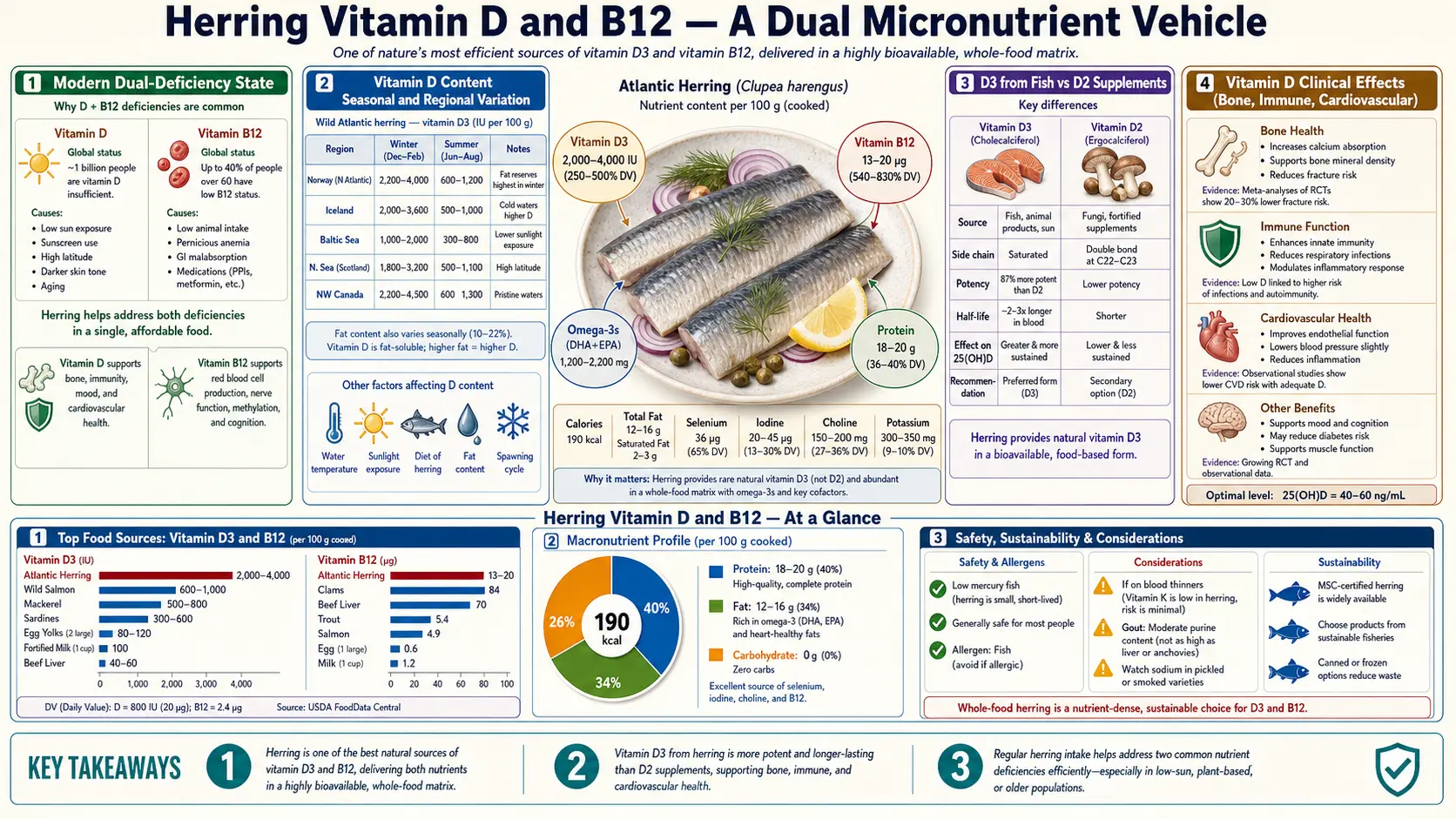
Vitamin D and Vitamin B12 are two of the most prevalent micronutrient deficiencies in industrialized populations — an estimated 40% of US adults have serum 25(OH)D below 20 ng/mL, and 6–20% of adults over 60 have functional B12 insufficiency. Herring is one of a very small number of natural foods that delivers pharmacologically meaningful doses of both in a single serving: a 100 g portion of Atlantic herring contains 600–1,600 IU of Vitamin D3 (depending on season and harvest waters) and 13.7 mcg of Vitamin B12 (570% of the adult RDA). Two servings per week supplies the equivalent of a daily Vitamin D supplement and corrects subclinical B12 deficiency in most adults — making herring a uniquely efficient dietary intervention for the dual-deficiency state that drives much of the metabolic, neurological, and immune dysfunction seen in modern populations.
Table of Contents
- The Modern Dual-Deficiency State
- Vitamin D Content: Seasonal and Regional Variation
- D3 (Cholecalciferol) from Fish vs D2 (Ergocalciferol) from Supplements
- Vitamin D Clinical Effects (Bone, Immune, Cardiovascular)
- B12 Content and Bioavailability
- The Four B12 Forms: Cyano, Methyl, Adeno, Hydroxo
- Methylmalonic Acid as the Functional B12 Marker
- B12 Depletion by Metformin and PPIs
- Population Targets and Practical Dosing
- Key Research Papers
- Connections
- Featured Videos
The Modern Dual-Deficiency State
Vitamin D and B12 are nutritionally unrelated but epidemiologically converge in modern populations because both rely on access patterns that have eroded over the last century. Vitamin D was historically synthesized in skin from UVB exposure to 7-dehydrocholesterol — indoor lifestyles, sunscreen use, latitude, and skin pigmentation have collectively reduced cutaneous synthesis to a fraction of pre-industrial levels. B12 is synthesized only by bacteria and archaea, and the human diet has historically obtained it primarily through animal foods (meat, eggs, dairy, fish) — vegetarian and vegan diets, age-related atrophic gastritis (which impairs intrinsic factor secretion), and long-term acid suppression have collectively reduced B12 absorption and intake.
The result is a substantial overlap deficiency: NHANES data show that 41% of US adults have 25(OH)D <20 ng/mL (frank deficiency by Endocrine Society thresholds), and that subclinical B12 deficiency (elevated methylmalonic acid or low holotranscobalamin) is present in 6% of adults under 60, rising to 20% in adults over 60 and 40% in long-term metformin users. Functional dual deficiency — both nutrients suboptimal in the same individual — is increasingly common in older adults and explains a meaningful share of the fatigue, cognitive complaints, peripheral neuropathy, and bone fragility seen in primary care.
Herring intervenes on both axes simultaneously through the food matrix, without supplementation, and without the conversion uncertainties associated with sun exposure or vegan dietary patterns.
Vitamin D Content: Seasonal and Regional Variation
Fish Vitamin D content varies substantially with species, fat content, harvest season, and harvest location. For Atlantic herring (Lu et al. 2007 J Agric Food Chem):
- Fresh Atlantic herring, raw — ~680–1,628 IU per 100 g
- Pickled herring — ~680 IU per 100 g
- Kippered herring (cold-smoked) — ~525–900 IU per 100 g
- Fresh Pacific herring — lower fat content, generally 300–600 IU per 100 g
For perspective, the same serving size of comparator fish:
- Wild Atlantic salmon: ~360 IU per 100 g
- Farmed Atlantic salmon: ~250 IU per 100 g (substantially lower than wild)
- Canned sardines in oil: ~270 IU per 100 g
- Canned albacore tuna: ~270 IU per 100 g
- Cod liver oil: ~10,000 IU per tablespoon (a category outlier)
- Beef liver: ~50 IU per 100 g
- Egg yolk: ~40 IU per yolk
Herring is therefore second only to cod liver oil and to certain wild-caught herring batches in delivered Vitamin D per gram of food — and substantially exceeds salmon, sardines, tuna, and all non-fish food sources. Seasonal variation is real: late-summer Atlantic herring harvested in waters with peak plankton blooms (the herring's UVB-exposed prey base) contains markedly more Vitamin D than winter-harvested fish.
D3 (Cholecalciferol) from Fish vs D2 (Ergocalciferol) from Supplements
Vitamin D exists in two principal forms in the human diet:
- Vitamin D3 (cholecalciferol) — synthesized in the skin of vertebrates from 7-dehydrocholesterol on UVB exposure. The only form found in fish, animal liver, and egg yolk.
- Vitamin D2 (ergocalciferol) — synthesized in fungi and some plants from ergosterol on UV exposure. The form found in mushrooms exposed to UV light and in some pharmaceutical and supplement preparations.
The Tripkovic 2012 meta-analysis (Am J Clin Nutr) compared D2 and D3 supplementation across 7 randomized trials and concluded that D3 raises serum 25(OH)D approximately 1.7× more effectively than equivalent doses of D2 — a difference attributed to higher receptor affinity and longer half-life of the D3 metabolites. The clinical implication is that 1,000 IU of Vitamin D3 from herring is biologically equivalent to roughly 1,700 IU of D2 from a fortified supplement or UV-treated mushroom.
Herring therefore provides not only a meaningful absolute dose of Vitamin D but the more bioactive of the two forms — a particularly relevant distinction for individuals with VDR (Vitamin D receptor) polymorphisms or CYP2R1 (the principal hepatic 25-hydroxylase) variants that further reduce D2 utilization.
Vitamin D Clinical Effects (Bone, Immune, Cardiovascular)
The clinical effects of adequate Vitamin D status span multiple organ systems:
- Bone — adequate 25(OH)D (≥30 ng/mL by Endocrine Society thresholds) is required for normal intestinal calcium absorption (~30% absorption efficiency vs ~15% in deficiency) and for the suppression of secondary hyperparathyroidism that accelerates cortical bone loss. The Chapuy 1992 NEJM trial showed that 800 IU Vitamin D3 + 1,200 mg calcium reduced hip fractures by 43% in elderly French nursing-home residents.
- Immune — Vitamin D receptors are expressed on most immune cell types; 1,25(OH)2D modulates T-cell differentiation, induces cathelicidin antimicrobial peptide production in macrophages, and is associated with reduced respiratory infection incidence (Martineau 2017 BMJ meta-analysis of 25 RCTs, 11,321 participants).
- Cardiovascular — observational data consistently associate low 25(OH)D with hypertension, MI, and CV mortality. Interventional trials (VITAL, D-Health, ViDA) have been largely null for primary cardiovascular endpoints, suggesting the observational association is partly confounded.
- Diabetes risk — the D2d trial (2019 NEJM) showed no overall reduction in T2DM progression from 4,000 IU/day D3 in prediabetic adults, but a subgroup analysis suggested benefit in participants with baseline 25(OH)D <20 ng/mL.
- Mortality — meta-analyses of supplementation trials suggest a modest (3–6%) reduction in all-cause mortality, driven primarily by reductions in cancer mortality at longer follow-up.
B12 Content and Bioavailability
Vitamin B12 is among the most concentrated micronutrients in animal foods, and herring is in the top tier of food sources:
- Beef liver — 70.6 mcg per 100 g (2,943% RDA)
- Clams — 98.9 mcg per 100 g (4,121% RDA)
- Atlantic herring — 13.7 mcg per 100 g (571% RDA)
- Sardines — 8.9 mcg per 100 g (371% RDA)
- Atlantic salmon — 4.8 mcg per 100 g (200% RDA)
- Tuna — 2.5 mcg per 100 g (104% RDA)
- Beef — 2.5 mcg per 100 g (104% RDA)
- Whole milk — 0.4 mcg per 100 g (17% RDA)
Absorption is the rate-limiting step. B12 in food is bound to protein, released by gastric acid and pepsin, transferred to haptocorrin in the stomach, freed by pancreatic proteases in the duodenum, and finally bound to intrinsic factor for receptor-mediated uptake in the terminal ileum. Absorption efficiency from a single dose is approximately 50% up to ~1.5 mcg, falling sharply at higher single doses due to saturation of the intrinsic factor pathway. The 13.7 mcg in a 100 g herring serving therefore delivers approximately 1.5 mcg of absorbed B12 from intrinsic-factor-dependent uptake, plus an additional ~1% from non-receptor-mediated diffusion.
This is well above the 2.4 mcg/day adult RDA and explains why two weekly servings of herring (or any equivalent fish) is sufficient B12 even for individuals with mildly reduced gastric acid output.
The Four B12 Forms: Cyano, Methyl, Adeno, Hydroxo
B12 exists in four principal chemical forms, distinguished by the upper axial ligand on the cobalt center:
- Cyanocobalamin — the synthetic form used in most supplements and food fortification. Stable, inexpensive, but requires intracellular conversion (and small cyanide release) to active coenzymes.
- Methylcobalamin — the coenzyme form used by methionine synthase in the methylation cycle. Required for conversion of homocysteine to methionine and indirectly for S-adenosylmethionine (SAMe) synthesis.
- Adenosylcobalamin — the mitochondrial coenzyme form used by methylmalonyl-CoA mutase. Required for propionate metabolism (branched-chain amino acids, odd-chain fatty acids, cholesterol side chain).
- Hydroxocobalamin — the form synthesized by gut bacteria and present in food. Long half-life; used as an injectable form for B12 deficiency treatment in Europe.
Food-source B12 (from herring and other animal foods) is predominantly hydroxocobalamin and the two coenzyme forms (methyl and adeno). This is a meaningful difference from cyanocobalamin supplements for individuals with MTRR (methionine synthase reductase) polymorphisms that impair the intracellular conversion of cyanocobalamin to methylcobalamin, and for individuals with rare cobalamin metabolism disorders (CblC, CblG) where the upstream conversion is impaired.
Methylmalonic Acid as the Functional B12 Marker
Serum B12 (cobalamin) is a poor marker of functional B12 status. Approximately 70% of circulating B12 is bound to haptocorrin (not biologically available); only the 20–30% bound to transcobalamin (holoTC) is delivered to peripheral tissues. Total serum B12 within the "normal" range (200–900 pg/mL) does not exclude functional deficiency.
The gold-standard functional markers are:
- Methylmalonic acid (MMA) — elevated when adenosylcobalamin is inadequate to support methylmalonyl-CoA mutase function. Specific for B12 deficiency (not confounded by folate). Reference range typically <0.4 µmol/L.
- Homocysteine — elevated in both B12 deficiency (methionine synthase impairment) and folate deficiency. Less specific than MMA, but useful in combination.
- Holotranscobalamin (holoTC, active B12) — the fraction of serum B12 actually deliverable to tissues. More sensitive than total B12, particularly in early deficiency.
The clinical implication is that practitioners should not rule out B12 deficiency on the basis of "normal" total B12. In a patient with peripheral neuropathy, fatigue, glossitis, or cognitive complaints, MMA or holoTC is the appropriate confirmatory test — particularly in adults over 60, long-term metformin users, PPI users, vegans, and patients with history of gastric surgery or atrophic gastritis.
B12 Depletion by Metformin and PPIs
Two of the most commonly prescribed long-term medications in modern primary care meaningfully reduce B12 absorption:
- Metformin — the Diabetes Prevention Program Outcomes Study (DPPOS) showed that long-term metformin use is associated with a 19% reduction in serum B12 over 13 years, with 7–9% of metformin users developing frank B12 deficiency. Mechanism: metformin disrupts calcium-dependent ileal absorption of the IF-B12 complex. Mitigation: oral calcium 1,200 mg/day partially reverses; B12 supplementation or dietary B12 from sources like herring directly addresses.
- Proton pump inhibitors (PPIs) — suppress gastric acid required to liberate B12 from dietary protein. Long-term PPI use (>2 years) is associated with a 65% increased risk of B12 deficiency (Lam 2013 JAMA, case-control of 25,956 cases).
- H2 blockers — smaller effect than PPIs but same mechanism. Long-term H2 use is associated with a 25% increased risk of B12 deficiency.
- Nitrous oxide — irreversibly oxidizes the cobalt center of B12, inactivating methionine synthase. Single-exposure for general anesthesia is generally tolerated; recreational use or prolonged anesthetic exposure can precipitate acute B12 deficiency neuropathy.
For patients on long-term metformin or PPI therapy, the simplest intervention is two weekly servings of B12-dense fish like herring (or sardines, salmon, mackerel), supplemented with periodic MMA monitoring if symptoms develop.
Population Targets and Practical Dosing
For a 65-kg adult, the dosing arithmetic is straightforward:
- Vitamin D target — serum 25(OH)D 30–50 ng/mL (Endocrine Society) requires approximately 1,500–2,000 IU/day in adults with limited sun exposure. Two weekly 100 g servings of herring supply approximately 1,360–3,250 IU/week (195–465 IU/day equivalent) — meaningful but typically insufficient on its own. Combination with sun exposure and/or a 1,000–2,000 IU daily D3 supplement is usually required.
- B12 target — RDA 2.4 mcg/day; functional adequacy typically requires 4–6 mcg/day of intake. Two weekly 100 g servings of herring supply approximately 4 mcg/day equivalent — sufficient for most adults without absorption impairment.
- Pregnancy and lactation — Vitamin D RDA 600 IU/day, B12 RDA 2.6 mcg/day. Two weekly servings of herring contribute meaningfully to both, while delivering the EPA + DHA required for fetal neural development.
- Vegan transition — the single highest-yield dietary intervention for vegans transitioning back to omnivore is fatty fish like herring — it simultaneously corrects B12, Vitamin D, omega-3, and iodine deficiencies that the long-term vegan pattern accumulates.
- Older adults — the population at highest risk of dual deficiency. Two weekly servings of herring address both nutrients in the food matrix and avoid the polypharmacy burden of separate D3 and B12 supplements.
Key Research Papers
- Lu Z et al., evaluation of vitamin D3 content in fish (J Agric Food Chem 2007) — Search PubMed
- Holick MF, vitamin D deficiency review (NEJM 2007) — PubMed 17634462
- Tripkovic L et al., D2 vs D3 supplementation meta-analysis (Am J Clin Nutr 2012) — PubMed 22552031
- Chapuy MC et al., vitamin D3 and calcium to prevent hip fractures in elderly women (NEJM 1992) — PubMed 1331788
- Martineau AR et al., vitamin D supplementation to prevent acute respiratory tract infections meta-analysis (BMJ 2017) — PubMed 28202713
- Manson JE et al., VITAL vitamin D and cardiovascular disease and cancer prevention (NEJM 2019) — PubMed 30415629
- Stabler SP, vitamin B12 deficiency clinical practice review (NEJM 2013) — PubMed 23301732
- Aroda VR et al., long-term metformin use and vitamin B12 deficiency in DPPOS (J Clin Endocrinol Metab 2016) — PubMed 26900641
- Lam JR et al., proton pump inhibitors and H2 blockers and risk of B12 deficiency (JAMA 2013) — PubMed 24327038
- Allen LH, vitamin B12 bioavailability and intake (Am J Clin Nutr 2009) — Search PubMed
- Carmel R, biomarkers of cobalamin status (Am J Clin Nutr 2011) — Search PubMed
- Pittas AG et al., D2d vitamin D supplementation and prevention of type 2 diabetes (NEJM 2019) — PubMed 31173679
Connections
- Benefits Hub
- Herring (Main Page)
- Omega-3 Density
- Pickled vs Fresh
- Sustainability and Lower Mercury
- Vitamin D3
- Vitamin B12
- Vitamin D Lab Test (25-OH)
- Methylmalonic Acid
- Homocysteine
- Sardines
- Salmon