Herring Omega-3 Density — EPA and DHA per Serving
Atlantic herring delivers approximately 1.7–2.0 g of combined EPA + DHA per 100 g serving, placing it consistently in the top three fish for marine omega-3 density alongside mackerel (2.5–2.7 g) and sardines (1.4–1.5 g). A single 4 oz serving (113 g) of herring supplies more EPA + DHA than 30 standard 1,000 mg fish oil softgel capsules — making it one of the most efficient dietary delivery vehicles for the omega-3 fatty acids that drive cardioprotective, anti-inflammatory, and neurocognitive effects documented across 40 years of clinical trial evidence.
Table of Contents
- Nutrient Density: Herring vs Other Fish and Supplements
- EPA vs DHA: Distinct Molecules, Distinct Roles
- Bypassing the ALA-to-EPA Bottleneck
- Cardiovascular Evidence: GISSI, REDUCE-IT, VITAL
- Inflammation Resolution and Specialized Pro-Resolving Mediators
- Neurocognitive Effects of DHA
- Dose Translation: Servings per Week
- Whole-Food Fish vs Fish Oil Supplements
- Oxidation, Storage, and Lipid Quality
- Key Research Papers
- Connections
- Featured Videos
Nutrient Density: Herring vs Other Fish and Supplements
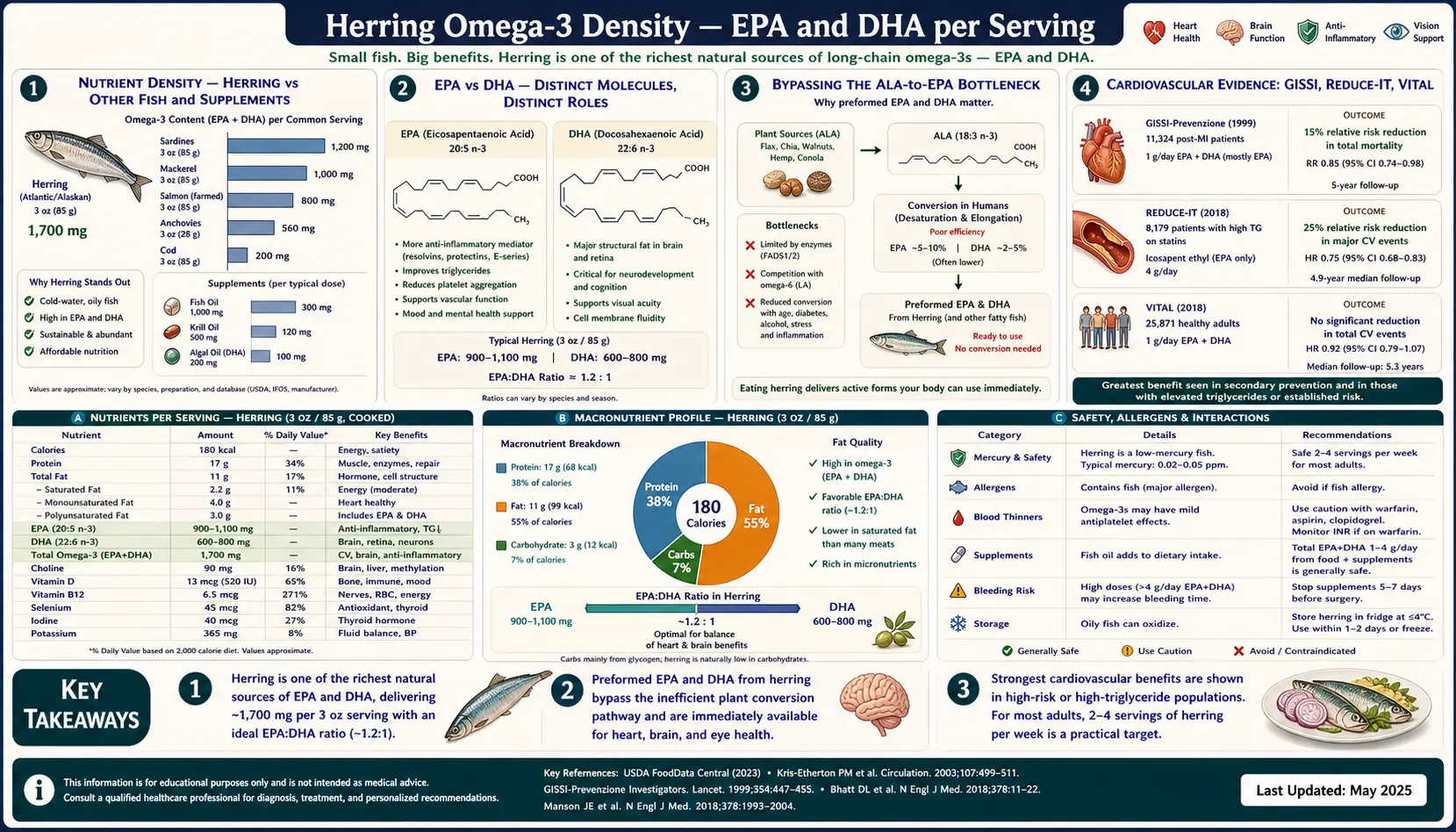
Marine omega-3 density per 100 g cooked serving, drawn from USDA FoodData Central and matched literature:
- Atlantic mackerel — ~2,670 mg EPA + DHA per 100 g
- Atlantic herring — ~1,729 mg EPA + DHA per 100 g (Pacific: ~1,810 mg)
- Sardines (canned in oil) — ~1,480 mg EPA + DHA per 100 g
- Wild Atlantic salmon — ~1,840 mg EPA + DHA per 100 g; farmed Atlantic: ~2,260 mg
- Anchovies (canned in oil) — ~2,055 mg EPA + DHA per 100 g
- Rainbow trout — ~840 mg EPA + DHA per 100 g
- Albacore tuna (canned) — ~860 mg EPA + DHA per 100 g
- Cod (Atlantic) — ~158 mg EPA + DHA per 100 g
- Tilapia — ~115 mg EPA + DHA per 100 g
For comparison, a typical 1,000 mg fish oil capsule contains 180 mg EPA + 120 mg DHA = 300 mg combined omega-3. A 100 g serving of herring thus delivers the equivalent omega-3 of roughly six 1,000 mg fish oil capsules — without the rancidity, encapsulation cost, or pill burden. A 4 oz (113 g) restaurant-style serving roughly doubles that to 1,950 mg, exceeding the American Heart Association recommendation of 1,000 mg/day for patients with established coronary heart disease in a single serving.
EPA vs DHA: Distinct Molecules, Distinct Roles
EPA (eicosapentaenoic acid, 20:5n-3) and DHA (docosahexaenoic acid, 22:6n-3) are often referenced jointly as "marine omega-3," but they are structurally and functionally distinct:
- EPA — 20-carbon backbone, 5 double bonds. Serves as substrate for the 3-series prostaglandins and 5-series leukotrienes, which are markedly less inflammatory than the AA-derived 2-series prostaglandins and 4-series leukotrienes. EPA is also the precursor to the E-series resolvins. EPA appears to drive most of the cardiovascular and triglyceride-lowering effects of marine omega-3.
- DHA — 22-carbon backbone, 6 double bonds. Selectively incorporated into neural and retinal phospholipids; DHA accounts for ~30–40% of the fatty acid composition of brain gray matter phospholipids and ~60% of photoreceptor outer-segment phospholipids. Substrate for D-series resolvins and protectins. DHA drives most of the neurocognitive and visual development effects.
Herring delivers EPA and DHA in roughly equal proportion (typically 700–900 mg each per 100 g), making it a balanced source for both effect categories. By contrast, krill oil is EPA-heavy with much less DHA, and algae-derived supplements are typically DHA-dominant with minimal EPA.
Bypassing the ALA-to-EPA Bottleneck
The plant-source omega-3 alpha-linolenic acid (ALA, 18:3n-3, found in flaxseed, walnuts, and chia) must be elongated and desaturated in vivo to produce EPA and DHA. The pathway requires the delta-6 desaturase enzyme (FADS2), elongase enzymes, and the delta-5 desaturase — with the same enzymatic machinery shared by the competing n-6 pathway converting linoleic acid to arachidonic acid.
Conversion efficiency in adults is poor:
- ALA → EPA conversion: approximately 5% in adult men, 21% in women of reproductive age (estrogen upregulates the pathway)
- ALA → DHA conversion: approximately 0–9% in adult men, 9% in women
- The pathway is further suppressed by high dietary linoleic acid (the typical Western 10:1 to 20:1 n-6:n-3 ratio drives the desaturase enzymes toward arachidonic acid synthesis)
The practical implication is that consuming 10 g of ALA from flaxseed delivers an expected 0.5 g of EPA and 0–1 g of DHA, with high inter-individual variation driven by FADS gene polymorphisms. The same gram of EPA + DHA from herring requires no conversion and is incorporated into cell membranes within hours of consumption. For individuals with the FADS1 rs174537 minor allele (common in populations of European ancestry), conversion efficiency is further reduced, making direct dietary EPA + DHA from fish particularly important.
Cardiovascular Evidence: GISSI, REDUCE-IT, VITAL
The cardiovascular omega-3 trial landscape includes both landmark positive studies and recent null trials that have refined the indication:
- GISSI-Prevenzione (1999) — 11,324 Italian post-MI patients randomized to 1 g/day EPA + DHA, Vitamin E, both, or neither for 3.5 years. The omega-3 arm showed a 20% reduction in all-cause mortality, 30% reduction in cardiovascular death, and 45% reduction in sudden cardiac death. The study established secondary-prevention omega-3 as a class IIa AHA recommendation.
- JELIS (2007) — 18,645 Japanese hypercholesterolemic patients randomized to statin + 1.8 g/day EPA vs statin alone. The EPA arm showed a 19% reduction in major coronary events.
- REDUCE-IT (2019) — 8,179 patients with established CVD or diabetes + elevated triglycerides randomized to icosapent ethyl (4 g/day purified EPA) vs mineral oil placebo. The EPA arm showed a 25% reduction in major adverse cardiovascular events at 4.9 years — the largest cardiovascular benefit of any omega-3 trial to date, driven by purified EPA at a pharmacological dose.
- VITAL (2019) — 25,871 US adults randomized to 1 g/day EPA + DHA for primary prevention. The trial was null for the composite cardiovascular endpoint but showed a 28% reduction in MI as a secondary endpoint, and a 17% reduction in CV events in participants consuming <1.5 servings of fish per week at baseline.
- STRENGTH (2020) — 13,078 patients randomized to a mixed EPA + DHA carboxylic acid formulation vs corn oil placebo. The trial was null, raising questions about whether the REDUCE-IT effect was driven by pure EPA specifically (vs mixed EPA + DHA) or by an unfavorable mineral oil placebo effect.
The 2021 American Heart Association Science Advisory continues to recommend two servings per week of oily fish for cardiovascular health, with the strongest evidence in secondary prevention and in patients with elevated triglycerides.
Inflammation Resolution and Specialized Pro-Resolving Mediators
The traditional model of omega-3 anti-inflammatory action emphasized competitive substrate displacement at the cyclooxygenase and lipoxygenase enzymes — EPA-derived 3-series prostaglandins are less inflammatory than AA-derived 2-series prostaglandins. Charles Serhan's laboratory at Harvard reframed the mechanism beginning in the early 2000s with the discovery of specialized pro-resolving mediators (SPMs), a family of lipid signaling molecules synthesized from EPA and DHA that actively terminate inflammation rather than passively reducing it.
SPM families include:
- E-series resolvins (RvE1, RvE2, RvE3) — synthesized from EPA via 5-lipoxygenase, drive macrophage clearance of apoptotic cells
- D-series resolvins (RvD1 through RvD6) — synthesized from DHA, inhibit neutrophil infiltration and promote tissue repair
- Protectins (PD1/NPD1) — synthesized from DHA, neuroprotective in models of ischemic and inflammatory CNS injury
- Maresins — synthesized from DHA by macrophages, drive tissue regeneration and pain resolution
The clinical implication is that adequate dietary EPA + DHA is not just an "anti-inflammatory" intervention — it is a substrate requirement for the active resolution phase that follows acute inflammation. Inadequate SPM synthesis is implicated in the chronic, non-resolving inflammation that characterizes atherosclerosis, periodontal disease, and rheumatoid arthritis.
Neurocognitive Effects of DHA
DHA accounts for 30–40% of phospholipid fatty acids in the gray matter of the cerebral cortex and 60% of phospholipid fatty acids in retinal photoreceptor outer segments. Dietary DHA crosses the blood-brain barrier via the MFSD2A transporter as lysophosphatidylcholine-DHA and is incorporated into neural membrane phospholipids over a timescale of weeks to months.
Functional implications:
- Fetal and infant neurodevelopment — DHA accumulates rapidly in the developing brain during the third trimester and first two years of life. The ALSPAC cohort (Hibbeln 2007 Lancet) found that maternal fish consumption <340 g/week in pregnancy was associated with reduced verbal IQ in offspring at age 8.
- Cognitive aging — the MIDAS trial (Yurko-Mauro 2010) randomized 485 healthy adults aged 55+ with age-associated memory complaints to 900 mg/day DHA vs placebo for 24 weeks, showing improved episodic memory scores in the DHA arm.
- Alzheimer's disease — observational cohort data consistently show reduced AD incidence in individuals with higher omega-3 intake and higher plasma DHA. Interventional trials in established AD have been null, suggesting the benefit may be limited to prevention rather than treatment.
- Mood and depression — meta-analyses suggest a modest antidepressant effect of EPA-predominant formulations at doses of 1–2 g/day, with weaker evidence for DHA-predominant or low-dose preparations.
Dose Translation: Servings per Week
The 2020–2025 US Dietary Guidelines recommend 8 oz (227 g) of seafood per week for the general adult, with at least one of the servings being a low-mercury oily fish. The American Heart Association recommends two 3.5-oz (100 g) servings per week of oily fish for cardiovascular health. Translating those targets to herring:
- For general health — one 100 g serving of herring per week supplies approximately 1.7 g of EPA + DHA, equivalent to a daily dose of 250 mg — matching the EFSA adequate intake recommendation for adults.
- For cardiovascular secondary prevention — two 100 g servings of herring per week supplies approximately 500 mg/day of EPA + DHA, in the range of the GISSI-Prevenzione effective dose.
- For triglyceride lowering (3–4 g/day target) — dietary herring alone cannot reach the pharmacological dose; combination of two weekly servings with prescription icosapent ethyl or omega-3 ethyl esters is typically required.
- For pregnancy and lactation — the FDA "best choices" list recommends 8–12 oz/week of low-mercury fish; herring is explicitly listed as a safe choice.
Whole-Food Fish vs Fish Oil Supplements
Whole-food fish has several advantages over fish oil supplements that are not captured in the EPA + DHA gram-equivalent comparison:
- Protein — 100 g of herring delivers ~18 g of complete protein with a high biological value (PDCAAS ~1.0) and the full essential amino acid profile.
- Vitamin D3, B12, selenium, iodine — co-delivered in the food matrix at meaningful doses (see Vitamin D and B12 deep-dive).
- Phospholipid-bound omega-3 — a meaningful fraction of herring omega-3 is in phospholipid form (phosphatidylcholine-EPA, phosphatidylcholine-DHA), which has higher bioavailability than the triglyceride or ethyl ester forms typical of fish oil capsules.
- Satiety and meal substitution — a serving of herring replaces a meal of lower-quality protein or refined carbohydrate, an effect a capsule cannot produce.
- Lower rancidity risk — whole fish, properly stored, has freshness signals (smell, color, texture) that consumers can evaluate. Fish oil capsules can be oxidized and rancid without detection until consumption.
The 2018 Cochrane systematic review of omega-3 supplement trials versus dietary fish suggested that the cardiovascular benefit attaches more clearly to whole-fish consumption than to capsule supplementation, although the comparison is confounded by other dietary co-variates.
Oxidation, Storage, and Lipid Quality
The 5 and 6 double bonds in EPA and DHA make them highly susceptible to peroxidation. Best-practice handling preserves the omega-3 yield of herring:
- Refrigerate fresh herring at 0–2°C and consume within 1–2 days of purchase — lipid oxidation accelerates above 4°C.
- Freeze at −30°C if storing >1 month — standard freezer temperatures (−18°C) preserve omega-3 for 2–3 months; lower temperatures extend usable life to 6–12 months.
- Cook briefly at moderate heat — baking, grilling, or pan-searing at <200°C preserves >90% of EPA + DHA. Deep-frying at >180°C in seed oil causes both oxidation and dilution with n-6 frying oil.
- Vacuum-packed and canned herring — well-preserved omega-3 due to oxygen exclusion. Canned products typically retain 85–95% of the omega-3 of fresh.
- Eat the visible fat — the EPA and DHA are concentrated in the dark muscle and subcutaneous fat layer. Trimming visible fat removes a meaningful fraction of the omega-3 yield.
Key Research Papers
- GISSI-Prevenzione Investigators, dietary supplementation with omega-3 polyunsaturated fatty acids and vitamin E after myocardial infarction (Lancet 1999) — PubMed 10465168
- Bhatt DL et al., REDUCE-IT cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia (NEJM 2019) — PubMed 30415628
- Manson JE et al., VITAL marine n-3 fatty acids and prevention of cardiovascular disease and cancer (NEJM 2019) — PubMed 30415637
- Yokoyama M et al., JELIS effects of EPA on major coronary events in hypercholesterolaemic patients (Lancet 2007) — PubMed 17398308
- Nicholls SJ et al., STRENGTH effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events (JAMA 2020) — PubMed 33190147
- Serhan CN, pro-resolving lipid mediators are leads for resolution physiology (Nature 2014) — PubMed 24899309
- Burdge GC and Calder PC, conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults (Reprod Nutr Dev 2005) — Search PubMed
- Yurko-Mauro K et al., MIDAS beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline (Alzheimers Dement 2010) — PubMed 20434961
- Hibbeln JR et al., ALSPAC maternal seafood consumption in pregnancy and neurodevelopmental outcomes (Lancet 2007) — PubMed 17307104
- Hu FB et al., fish and omega-3 fatty acid intake and risk of coronary heart disease in women (JAMA 2002) — Search PubMed
- Mozaffarian D and Rimm EB, fish intake, contaminants, and human health (JAMA 2006) — PubMed 17047219
- Calder PC, omega-3 polyunsaturated fatty acids and inflammatory processes (Biochim Biophys Acta 2015) — PubMed 25149823
Connections
- Benefits Hub
- Herring (Main Page)
- Vitamin D and B12
- Pickled vs Fresh
- Sustainability and Lower Mercury
- Omega-3 Fatty Acids
- Sardines
- Salmon
- Cardiology
- Neurology
- Anti-Inflammatory
- Omega-3 Index Test