Beef for CLA and Omega-3 Ratio
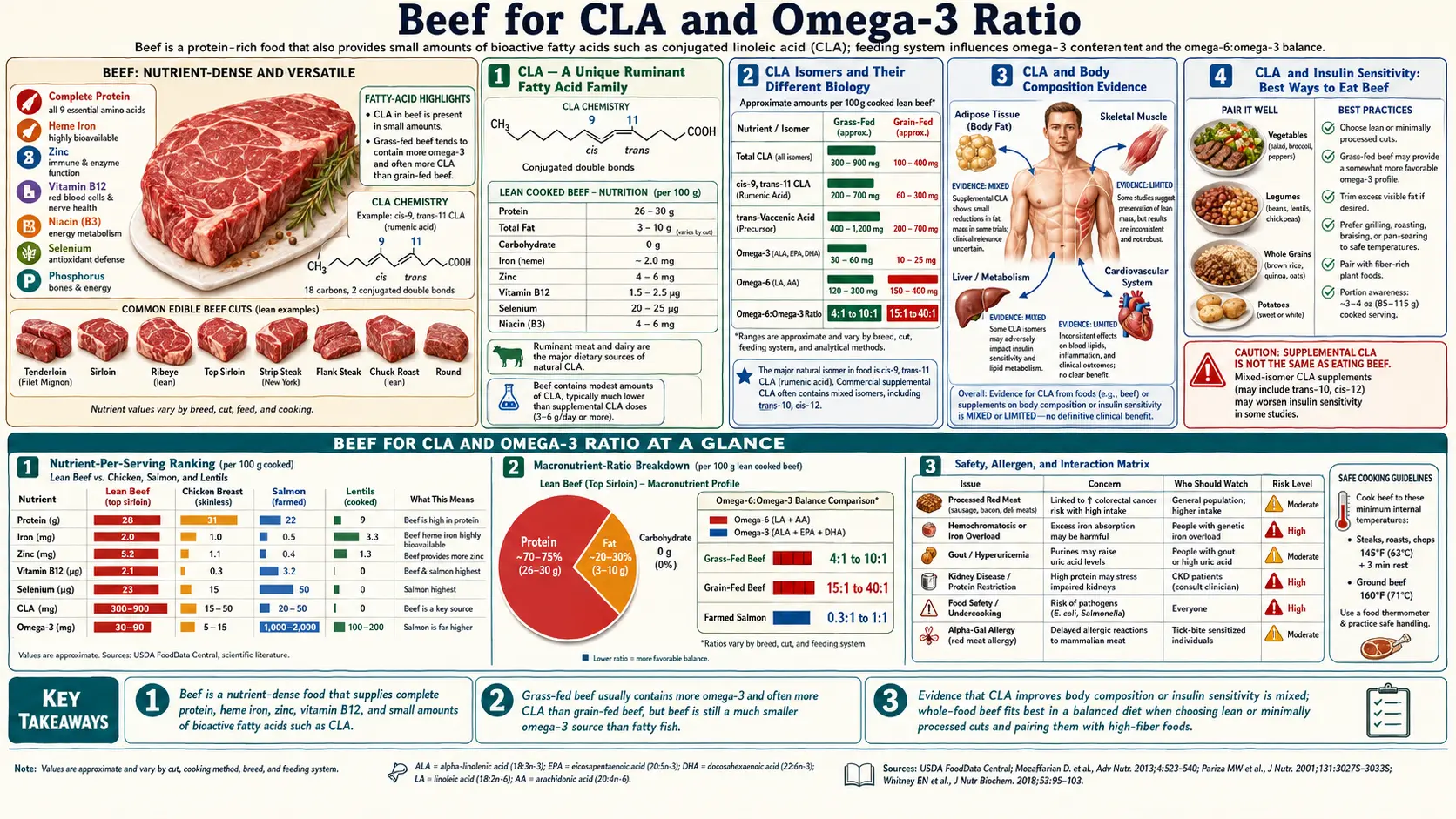
Conjugated linoleic acid (CLA) and the omega-6 to omega-3 fatty acid ratio are the two most-discussed and most-marketed nutritional features of the beef fat fraction. Both deserve a careful look that separates the strong biochemistry from the much weaker clinical evidence. CLA is a family of naturally occurring positional and geometric isomers of linoleic acid, produced exclusively by ruminant bacteria from feed linoleic acid. The dominant naturally occurring isomer (cis-9, trans-11 CLA, called rumenic acid) is structurally and biologically different from the trans fatty acids of partially hydrogenated industrial fats and should not be conflated with them. The omega-6 to omega-3 ratio of beef ranges from approximately 2:1 in grass-finished beef to 8:1 in grain-finished beef — both substantially better than the 15:1 ratio of the typical industrial Western diet, and within or close to the 1:1 to 4:1 range associated with lower inflammation in cross-cultural epidemiology. This page works through the biochemistry of both, the clinical trial evidence on body composition, insulin sensitivity, and cardiovascular markers, and the practical question of how much these fatty acid features should influence beef choice and overall diet design.
Table of Contents
- CLA — A Unique Ruminant Fatty Acid Family
- CLA Isomers and Their Different Biology
- CLA and Body Composition Evidence
- CLA and Insulin Sensitivity
- CLA and Cancer Research
- The Omega-6 to Omega-3 Ratio Hypothesis
- Beef and the Dietary Ratio in Context
- What Actually Improves the Ratio
- Saturated Fat in Beef: Modern Cardiology Context
- Practical Implications
- Key Research Papers
- Connections
- Featured Videos
CLA — A Unique Ruminant Fatty Acid Family
Conjugated linoleic acid was discovered as a meat-derived anticancer factor in the 1980s by Michael Pariza at the University of Wisconsin, who was investigating mutagenic compounds in fried beef and unexpectedly identified a protective rather than harmful factor. Subsequent work characterized CLA as a family of positional and geometric isomers of the 18-carbon polyunsaturated fatty acid linoleic acid, where the two double bonds are in a conjugated (1,3-diene) configuration rather than the standard methylene-interrupted (1,4-diene) configuration of linoleic acid itself.
CLA is produced naturally in the rumen of cattle, sheep, goats, and other ruminants by the bacterium Butyrivibrio fibrisolvens, which partially hydrogenates dietary linoleic acid through the conjugated intermediate. The CLA thus produced is absorbed by the ruminant and stored in tissues and milk fat. There is no significant non-ruminant source of CLA in the food supply — ruminant meat and dairy are essentially the only meaningful dietary sources.
The naturally occurring CLA in ruminant fat is dominated by cis-9, trans-11 CLA (rumenic acid), which makes up 80-90% of total CLA in beef and dairy fat. A smaller fraction (5-15%) is trans-10, cis-12 CLA, which has different biological effects. This isomer distinction matters because most of the early supplement studies used a 50:50 mixture of the two isomers (called "mixed CLA"), and many of the metabolic effects attributed to "CLA" actually trace to the trans-10, cis-12 isomer that is a minor fraction of natural ruminant CLA.
The most important conceptual point: rumenic acid (cis-9, trans-11 CLA) is a trans fatty acid by chemical definition (one of its double bonds is in the trans configuration), but it is not associated with the cardiovascular harm of the artificial trans fats produced by industrial partial hydrogenation of vegetable oils. The two come from different sources, have different metabolic fates, and have different epidemiologic associations. The FDA-regulated trans fat label specifically excludes ruminant trans fats from its limits for this reason.
CLA Isomers and Their Different Biology
The two principal CLA isomers have distinct and sometimes opposite metabolic effects:
- cis-9, trans-11 CLA (rumenic acid) — dominant in ruminant fat. Associated in animal studies with anti-inflammatory effects (modest reduction in pro-inflammatory cytokines), modest improvement in insulin sensitivity, and possible cardioprotective effects. Generally considered the "good CLA."
- trans-10, cis-12 CLA — minor fraction in natural beef but the more biologically active isomer in body-composition research. Reduces adipocyte triglyceride storage and increases lipolysis in animal and in-vitro studies. However, in human trials it has also been associated with adverse effects on insulin sensitivity, increased inflammation, and fatty liver in some studies.
Most clinical CLA supplements sold in the US are mixed isomers in roughly 50:50 ratio, derived from industrial isomerization of safflower or sunflower oil linoleic acid. These supplements do not replicate the natural isomer balance of ruminant CLA, and most of the published clinical CLA research has used these mixed-isomer products at doses (typically 3-4 g/day) far higher than achievable through diet.
The implication is that the clinical effects of CLA supplements should not be assumed to apply to dietary CLA from beef, both because of the different isomer ratio and because of the different total dose. Dietary CLA from beef is predominantly rumenic acid, in cumulative milligram quantities per serving. Supplemental CLA is predominantly the trans-10, cis-12 isomer (or 50:50), in gram quantities per day.
CLA and Body Composition Evidence
The most popular consumer-facing CLA claim is body fat reduction. The Whigham et al. 2007 meta-analysis in the American Journal of Clinical Nutrition pooled 18 randomized trials of CLA supplementation totaling 1,054 subjects. Key findings:
- Average dose 3.4 g/day for an average of 6-12 months
- Average fat mass reduction of approximately 0.09 kg per week, equivalent to roughly 4.7 kg per year if maintained
- Effect sizes were small and clinically modest
- Effect was greatest in overweight and obese subjects
- Lean body mass was preserved or slightly increased
The Dilzer and Park 2012 review in Critical Reviews in Food Science and Nutrition and the 2019 den Hartigh review in Nutrients largely confirmed the pattern: modest fat mass reduction from CLA supplementation, small effect sizes, more pronounced in animal models than in humans. The effect is real but not dramatic.
The dose required for these effects (3-6 g/day) is approximately 100-300 times higher than the CLA intake from typical dietary consumption of ruminant fat. There is no plausible scenario in which dietary CLA from beef contributes meaningfully to body composition through this acute mechanism. Whatever chronic cumulative effects of dietary CLA exist would be much smaller than supplement-driven effects.
CLA and Insulin Sensitivity
The metabolic effects of CLA on insulin sensitivity have been a research priority because of the strong animal-model signal showing improvement. Human trials have been more mixed:
- Mixed-isomer CLA supplements (the typical commercial product) have shown worsening of insulin sensitivity in some human trials, attributed to the trans-10, cis-12 isomer's pro-inflammatory effect on liver and adipose tissue
- Pure cis-9, trans-11 CLA (rumenic acid) has shown neutral or modestly favorable insulin sensitivity effects, though large trials are scarce
- Population observational studies of dietary CLA intake (rather than supplemental CLA) tend to show favorable associations with insulin sensitivity, possibly reflecting the favorable isomer ratio of dietary CLA
The mixed evidence is one reason that CLA supplements are not currently recommended for diabetes management or insulin sensitivity improvement, despite the body composition signal. Dietary CLA from beef appears to be either neutral or modestly favorable for insulin sensitivity, but the effect is small enough that beef should not be sold to consumers as an insulin-sensitivity intervention.
CLA and Cancer Research
The original Pariza discovery of CLA was as an anti-mutagenic factor in fried beef. Subsequent animal-model research has consistently shown anti-tumor effects of CLA, particularly for breast cancer, colon cancer, and skin cancer, at supplemental doses. The mechanisms include:
- Inhibition of cell proliferation through PPAR-gamma activation
- Induction of apoptosis in transformed cells
- Reduction of angiogenesis
- Modulation of inflammatory cytokines
- Effects on cellular fatty acid composition that may reduce membrane susceptibility to peroxidation-driven damage
Human cancer outcome data are much less robust. A few observational studies have suggested favorable associations between dietary CLA intake (estimated from dairy fat consumption) and breast cancer risk in postmenopausal women, but the signal is inconsistent and confounded by other features of dairy and meat consumption.
The Belury 2002 Annual Review of Nutrition and Bhattacharya 2006 Journal of Nutritional Biochemistry reviews remain authoritative summaries of the CLA biological effects. The clinical translation has been less successful than the animal-model literature suggested, which is a recurring pattern in cancer chemoprevention research.
The Omega-6 to Omega-3 Ratio Hypothesis
The omega-6 to omega-3 fatty acid ratio hypothesis was articulated most influentially by Artemis Simopoulos in a series of papers from the late 1990s through the 2000s, including the 2002 Biomedicine & Pharmacotherapy paper that is one of the most-cited papers in nutrition science. The hypothesis is that:
- Hunter-gatherer and traditional human diets had an omega-6 to omega-3 ratio of approximately 1:1 to 4:1, with omega-3 from wild fish and game and omega-6 from wild plant foods
- The modern industrial Western diet has a ratio of approximately 15:1 to 20:1, driven by the explosive growth of soybean, corn, and other seed oil consumption from the 1960s onward, and by the omega-6-heavy grain feeding of livestock
- Omega-6 fatty acids are metabolized via cyclooxygenase and lipoxygenase pathways to pro-inflammatory eicosanoids; omega-3 fatty acids compete for the same enzymes and produce less inflammatory or actively anti-inflammatory eicosanoids
- The shift in the dietary ratio has shifted the eicosanoid balance toward inflammation, contributing to the modern epidemic of inflammatory and metabolic diseases
The hypothesis has been influential but also contested. The proponents' argument is supported by cross-cultural epidemiology (low-ratio populations like traditional Japanese, Mediterranean, and Inuit had lower cardiovascular disease rates) and by mechanistic biochemistry (the eicosanoid pathway is real and well-characterized). The critics argue that the eicosanoid pathway effects are partial, that linoleic acid (the dominant omega-6) has its own beneficial effects on cholesterol and cardiovascular health, and that absolute omega-3 intake is more important than the ratio.
The 2011 Mozaffarian and Wu review in JACC and the Calder 2017 Biochemical Society Transactions paper give contemporary perspectives. The current consensus is that increasing omega-3 intake (particularly EPA and DHA from fatty fish) is well-supported, while aggressive omega-6 reduction is more controversial. The ratio matters somewhat, but absolute omega-3 sufficiency probably matters more.
Beef and the Dietary Ratio in Context
The omega-6 to omega-3 ratio of beef varies substantially by production system:
- Grass-finished beef — ratio approximately 1.5:1 to 2:1 (favorable)
- Grain-finished beef — ratio approximately 7:1 to 10:1 (less favorable but still better than the diet average)
- Modern industrial Western diet average — 15:1 to 20:1
- Mediterranean diet (well-followed) — approximately 4:1 to 6:1
- Hunter-gatherer dietary reconstruction — approximately 1:1 to 4:1
The point is that beef of either production type has a more favorable omega-6 to omega-3 ratio than the dietary average. Substituting beef for industrial seed oil-heavy foods (most processed foods, fast food, baked goods, fried foods) improves the ratio, regardless of grass-finished vs grain-finished. Choosing grass-finished further improves it.
The total absolute omega-3 contribution from beef is modest in either case — a 3-oz serving of grass-finished beef provides perhaps 80 mg of long-chain omega-3, vs 1,500-2,000 mg in a 3-oz serving of fatty fish. Beef should not be viewed as an omega-3 source in the way that fish is. But beef should also not be viewed as a meaningful contributor to omega-6 excess in the way that industrial seed oils are. See our Omega-3 page for the full story.
What Actually Improves the Ratio
For an adult with a goal of meaningfully shifting the dietary omega-6 to omega-3 ratio toward the lower end of the spectrum, the most effective interventions in approximate order of impact are:
- Reduce industrial seed oil consumption — soybean, corn, sunflower, safflower, cottonseed, grapeseed oils are the dominant source of omega-6 excess in the modern diet. These oils are used heavily in processed foods, restaurant cooking, salad dressings, mayonnaise, and many baked goods. Cooking at home with olive oil, butter, ghee, or animal fats instead is the single most impactful change.
- Eat fatty fish 2-3 times per week — salmon, sardines, mackerel, anchovies, herring are the most reliable sources of long-chain omega-3 (EPA and DHA). A 3-4 oz serving provides ~1,500-2,500 mg of long-chain omega-3. See our Salmon page and our Sardines page.
- Consider fish oil or algae oil supplementation — for those who cannot or do not eat fatty fish regularly. 1-2 g/day combined EPA + DHA is the typical cardiovascular dose.
- Choose grass-finished beef when feasible — better ratio than grain-finished, contribution to overall diet is meaningful, particularly if fish intake is low. See our Grass-Fed vs Grain-Fed deep dive.
- Add ALA-rich plant sources — flax, chia, walnuts contain alpha-linolenic acid, the parent omega-3. Conversion to EPA and DHA in humans is inefficient (~5% for EPA, <1% for DHA) so these are partial replacements for fish but contribute to baseline.
- Pasture-raised eggs and dairy — same logic as grass-finished beef applied to other animal products. Pasture-raised eggs have measurably more omega-3 than conventional eggs.
The relative impact of each: substituting butter and olive oil for industrial seed oils probably shifts the dietary ratio more than any other single change. Adding fatty fish twice a week probably shifts it more than switching from grain-finished to grass-finished beef. The grass-finished beef switch is incremental but meaningful for those who consume beef regularly.
Saturated Fat in Beef: Modern Cardiology Context
The historical concern about beef and cardiovascular disease focused on saturated fat content. The diet-heart hypothesis as advanced by Ancel Keys in the 1950s-1970s held that dietary saturated fat raises LDL cholesterol which raises cardiovascular disease risk. This was the basis for decades of dietary guidance to limit red meat consumption.
The modern cardiology context is more nuanced:
- The relationship between dietary saturated fat and serum LDL cholesterol is real but variable between individuals (some respond strongly, some not at all)
- The relationship between serum LDL cholesterol and cardiovascular disease risk is well-established in apoB-particle terms, though saturated fat's effect on apoB and small-dense LDL is more nuanced than just total LDL-C
- The relationship between dietary saturated fat intake and cardiovascular outcomes in observational and randomized trial data is weaker than the linear model predicts (Siri-Tarino 2010 AJCN meta-analysis found no significant association)
- Different saturated fats have different metabolic effects (stearic acid, dominant in beef, has near-neutral effect on LDL; palmitic acid raises it more)
- The food matrix matters — the same amount of saturated fat in cheese or yogurt has different cardiovascular effects than in processed meat
The Johnston et al. 2019 NutriRECS systematic review and meta-analysis published in Annals of Internal Medicine concluded that the evidence does not support reducing unprocessed red meat consumption for cardiovascular reasons in the general adult population. The companion Zeraatkar et al. 2019 meta-analysis found small and statistically marginal associations between red meat consumption and cardiovascular mortality, of a magnitude unlikely to support general avoidance recommendations.
Processed meat (bacon, deli meats, hot dogs, sausages preserved with nitrates) has stronger and more consistent associations with adverse cardiovascular and cancer outcomes and should be considered separately. Unprocessed beef, including fatty cuts, does not show the same signal.
This does not mean that anyone should eat unlimited beef. It means that the older guidance to severely restrict beef consumption for cardiovascular prevention is not supported by current evidence in adults without specific cardiovascular conditions or familial hypercholesterolemia. For individual cardiovascular risk management, see our Cardiology section.
Practical Implications
- For omega-3 sufficiency, fatty fish is the high-leverage intervention — 2-3 servings per week of salmon, sardines, mackerel, or anchovies will accomplish far more than any beef-related change.
- For omega-6 reduction, industrial seed oil avoidance is the high-leverage intervention — cooking at home with butter, olive oil, ghee, or animal fats and avoiding processed foods with high seed oil content matters more than the beef finishing system.
- Grass-finished beef provides incremental benefit for the fatty acid profile — meaningful if beef is consumed regularly, particularly for individuals who do not eat much fish.
- CLA supplementation is not recommended on current evidence — the body composition effect is small, the mixed-isomer formulations may worsen insulin sensitivity, and the dose-effect relationship at dietary intake levels is unclear.
- Beef of either production type is not a meaningful driver of omega-6 excess — the ratio in beef is more favorable than the average diet, so substituting beef for industrial-food alternatives improves the ratio.
- Total fat intake from beef is variable by cut — a 6-oz top sirloin has approximately 12 g of total fat; a 6-oz ribeye has approximately 30 g. Choose by appetite and overall daily fat targets.
- Processed meat (bacon, deli meat, hot dogs) is in a different category than unprocessed beef and should be limited regardless of personal cardiovascular risk profile.
- Cardiovascular risk is multifactorial — smoking, physical inactivity, untreated hypertension, obesity, untreated diabetes, untreated hyperlipidemia are larger leverage points than the type of beef consumed.
Key Research Papers
- Whigham LD, Watras AC, Schoeller DA (2007). Efficacy of conjugated linoleic acid for reducing fat mass: a meta-analysis in humans. American Journal of Clinical Nutrition. — PMID 17490954
- Simopoulos AP (2002). The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomedicine & Pharmacotherapy. — PMID 12442909
- Belury MA (2002). Dietary conjugated linoleic acid in health: physiological effects and mechanisms of action. Annual Review of Nutrition. — Search PubMed
- Dilzer A, Park Y (2012). Implication of conjugated linoleic acid (CLA) in human health. Critical Reviews in Food Science and Nutrition. — PMID 22452730
- Bhattacharya A, Banu J, Rahman M, et al. (2006). Biological effects of conjugated linoleic acids in health and disease. Journal of Nutritional Biochemistry. — PMID 16650752
- den Hartigh LJ (2019). Conjugated linoleic acid effects on cancer, obesity, and atherosclerosis: a review of pre-clinical and human trials with current perspectives. Nutrients. — Search PubMed
- Field CJ, Blewett HH, Proctor S, Vine D (2009). Human health benefits of vaccenic acid. Applied Physiology, Nutrition, and Metabolism. — Search PubMed
- Mozaffarian D, Wu JH (2011). Omega-3 fatty acids and cardiovascular disease: effects on risk factors, molecular pathways, and clinical events. Journal of the American College of Cardiology. — PMID 22051327
- Calder PC (2017). Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochemical Society Transactions. — PMID 28900017
- Siri-Tarino PW, Sun Q, Hu FB, Krauss RM (2010). Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. American Journal of Clinical Nutrition. — PMID 20071648
- Johnston BC, Zeraatkar D, Han MA, et al. (2019). Unprocessed red meat and processed meat consumption: dietary guideline recommendations from the NutriRECS Consortium. Annals of Internal Medicine. — PMID 31569235
- Zeraatkar D, Han MA, Guyatt GH, et al. (2019). Red and processed meat consumption and risk for all-cause mortality and cardiometabolic outcomes: a systematic review and meta-analysis. Annals of Internal Medicine. — PMID 31569213
- Bhupathiraju SN, Tucker KL (2011). Coronary heart disease prevention: nutrients, foods, and dietary patterns. Clinica Chimica Acta. — Search PubMed
- Ridker PM, Everett BM, Thuren T, et al. (2017). Antiinflammatory therapy with canakinumab for atherosclerotic disease (CANTOS). NEJM. — PMID 28845751
PubMed Topic Searches
- PubMed: CLA body composition trials
- PubMed: Omega-6 to omega-3 ratio
- PubMed: Rumenic acid CLA
- PubMed: Red meat and cardiovascular disease
- PubMed: Saturated fat and cardiovascular
Connections
- Beef Overview
- Beef Benefits Hub
- Iron and B12
- Creatine and Carnosine
- Grass-Fed vs Grain-Fed
- Omega-3 Fatty Acids
- Salmon
- Sardines
- Herring
- Eggs
- Cardiology
- Type 2 Diabetes
- Insulin Resistance
- Organ Meats
- All Foods