Testicular Cancer
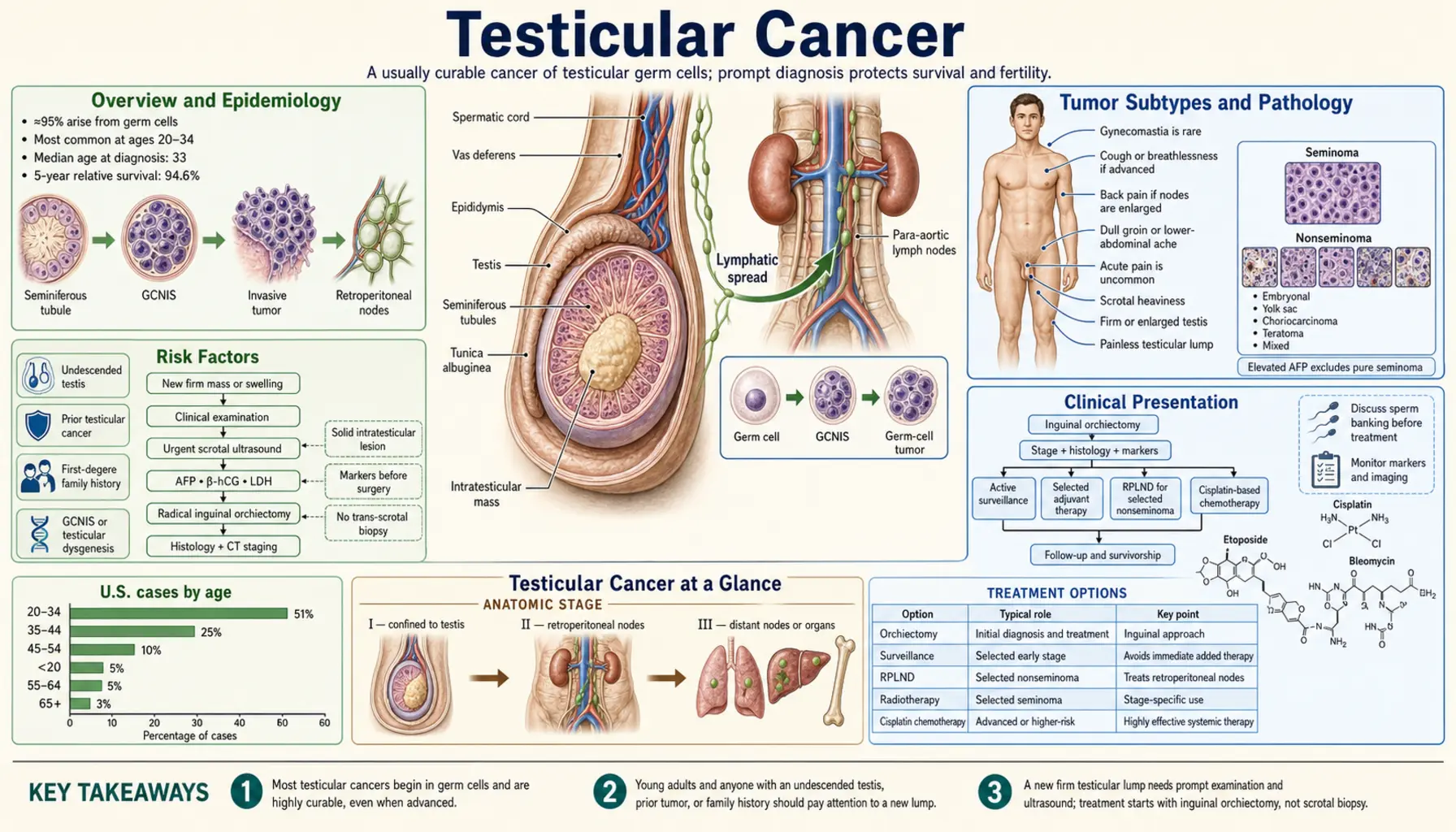
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Classification
- Tumor Markers
- Diagnosis and Staging
- Treatment by Stage
- Retroperitoneal Lymph Node Dissection
- Complications
- Fertility and Quality of Life
- Recent Research
- References
- Research Papers
- Connections
- Featured Videos
1. Overview
Testicular cancer is the most common solid malignancy in men aged 15 to 35, accounting for approximately 1–2% of all male cancers but representing the leading cause of cancer-related death in young men before cisplatin-based chemotherapy became standard care. More than 95% of testicular tumors arise from germ cells (germ cell tumors, GCTs), making GCT the dominant clinical and pathological entity. Two main GCT subtypes exist: seminoma (approximately 60% of GCTs) and non-seminomatous germ cell tumor (NSGCT) (approximately 40%), each with distinct biology, marker profiles, and treatment strategies.
Testicular cancer is one of the most curable solid tumors in oncology. Even in the setting of metastatic disease, 5-year survival exceeds 95% overall, owing to exquisite chemosensitivity to cisplatin-based regimens. Cure rates for localized disease approach 99%, and the majority of patients can expect normal life expectancy after treatment. Awareness of early signs — typically a painless testicular mass or swelling — is essential, as prompt radical orchiectomy provides both diagnosis and definitive local therapy.
2. Epidemiology
Approximately 9,000 new cases of testicular cancer are diagnosed annually in the United States, with roughly 400 deaths per year — a remarkably low mortality-to-incidence ratio reflecting high cure rates. Incidence has been rising steadily in developed countries over the past five decades, with particularly sharp increases in Scandinavian nations and the United States, suggesting environmental or lifestyle contributors not yet fully elucidated.
The peak incidence occurs between ages 20 and 34, with a smaller secondary peak in men over 60 (predominantly spermatocytic seminoma). Testicular cancer is notably more common in white men, with incidence rates approximately 4–5 times higher than in Black men, and intermediate rates in Hispanic and Asian populations. The reasons for this racial disparity remain incompletely understood but may involve differences in gonadal development, hormonal environment, or environmental exposures.
Key established risk factors include:
- Cryptorchidism (undescended testis): Carries a 4- to 8-fold increased risk. Orchiopexy before puberty reduces but does not eliminate the risk elevation. Both the undescended and the contralateral descended testis carry elevated risk, suggesting a shared gonadal dysgenesis mechanism.
- Personal history of testicular GCT: Men with a prior GCT have a 12-fold increased risk of a contralateral tumor.
- Family history: First-degree relatives of affected men have a 4- to 10-fold elevated risk; twin studies suggest a polygenic heritable component.
- Testicular dysgenesis syndrome: Encompasses hypospadias, poor semen quality, and gonadal maldescent — all linked to GCT risk via shared in-utero hormonal disruption.
- Klinefelter syndrome: Associated with mediastinal (extragonadal) GCTs.
3. Pathophysiology
The pathogenesis of testicular GCT centers on germ cell neoplasia in situ (GCNIS), formerly called intratubular germ cell neoplasia (ITGCN) or carcinoma in situ, which is the obligate precursor to invasive GCT (excluding spermatocytic seminoma). GCNIS cells are gonocyte-like cells that fail to differentiate normally during fetal gonadal development, persisting into postnatal life and accumulating additional oncogenic hits during puberty under gonadotropin stimulation.
Isochromosome 12p
The isochromosome of the short arm of chromosome 12 — i(12p) — is the pathognomonic chromosomal abnormality of testicular GCT, present in more than 90% of invasive tumors. Amplification of 12p leads to overexpression of cyclin D2, CCND2, KRAS, and stem-cell-related genes, driving uncontrolled proliferation and inhibiting apoptosis. Detection of i(12p) by FISH is diagnostically useful in ambiguous or extragonadal GCT cases.
Seminoma vs Non-Seminoma Molecular Profiles
Seminoma retains features of primordial germ cells and expresses PLAP (placental alkaline phosphatase), OCT3/4, NANOG, and c-KIT. Critically, pure seminoma does never produce alpha-fetoprotein (AFP) — any AFP elevation in a histologically "pure" seminoma mandates reclassification as a mixed or non-seminomatous tumor. Seminoma is exquisitely sensitive to radiation and cisplatin-based chemotherapy.
Non-seminomatous GCTs (NSGCTs) display a spectrum of differentiation states. The various NSGCT histologies each have distinct molecular and marker profiles, reflecting their embryonic lineage: embryonal carcinoma expresses OCT3/4 and CD30; yolk sac tumor produces AFP; choriocarcinoma secretes beta-hCG at very high levels; teratoma is marker-negative.
Blood-Testis Barrier Breakdown
The blood-testis barrier, formed by Sertoli cell tight junctions, normally sequesters developing germ cells from immune surveillance. Disruption of this barrier by GCT allows tumor-associated antigens and serum markers (AFP, beta-hCG) to enter the bloodstream, providing the basis for the highly informative clinical serum tumor marker panel in testicular cancer management.
4. Classification
The World Health Organization (WHO) classification of testicular tumors divides primary testicular neoplasms into germ cell and non-germ cell tumors:
Germ Cell Tumors (GCT) — derived from GCNIS
- Seminoma (classical): Accounts for approximately 60% of GCTs. Uniform sheets of large cells with clear glycogen-rich cytoplasm and prominent nucleoli, separated by fibrous septa infiltrated by lymphocytes. Spreads predominantly via lymphatics to para-aortic lymph nodes. Highly radiosensitive and chemosensitive. AFP always negative.
- Spermatocytic seminoma: Distinct entity arising in older men (mean age ~55), not associated with GCNIS or i(12p), extremely rare metastatic potential. Does not require aggressive treatment.
Non-Seminomatous GCT (NSGCT)
- Embryonal carcinoma: Most common NSGCT component. Highly aggressive; anaplastic cells with glandular or papillary architecture. CD30+. LVI (lymphovascular invasion) is a major staging determinant for Stage I disease.
- Yolk sac tumor (endodermal sinus tumor): The dominant component in prepubertal boys; produces AFP. Schiller-Duval bodies are pathognomonic on histology.
- Choriocarcinoma: Rarest and most aggressive NSGCT. Composed of syncytiotrophoblasts and cytotrophoblasts; produces very high beta-hCG. Associated with hematogenous metastases (lungs, liver, brain) and poorest prognosis among GCTs. Even small primary tumors can cause widespread disease.
- Teratoma: Contains elements from two or more germ layers (ectoderm, mesoderm, endoderm). Mature teratoma is benign in children but in post-pubertal males carries malignant potential, does not respond to chemotherapy, and requires surgical resection. Immature teratoma and teratoma with somatic-type malignancy are aggressive variants.
- Mixed GCT: The most common NSGCT presentation; any combination of the above histologies. Managed as NSGCT regardless of the proportion of seminomatous elements.
Non-Germ Cell Tumors (rare, mostly benign)
- Leydig cell tumor: Most common sex cord-stromal tumor; usually benign; may produce testosterone or estrogen causing hormonal symptoms (gynecomastia, precocious puberty).
- Sertoli cell tumor: Rare; generally benign; minority are malignant (large cell calcifying subtype).
- Granulosa cell tumor: Extremely rare; indolent course in most cases.
5. Tumor Markers
Three serum tumor markers are central to the diagnosis, staging, risk stratification, and surveillance of testicular cancer. All three must be measured pre-orchiectomy and serially post-treatment. Failure of markers to decline appropriately after orchiectomy indicates residual or metastatic disease.
Alpha-Fetoprotein (AFP)
AFP is a fetal glycoprotein produced by yolk sac cells and fetal liver hepatocytes. In testicular cancer, AFP elevation indicates the presence of yolk sac tumor or embryonal carcinoma elements. AFP is never elevated in pure seminoma or pure choriocarcinoma — any AFP elevation in a histologically pure seminoma mandates reclassification as NSGCT and management as such. Normal adult AFP is less than 10 ng/mL. Serum half-life: 5–7 days. Persistently elevated or rising AFP post-orchiectomy confirms residual or metastatic disease.
Beta Human Chorionic Gonadotropin (β-hCG)
Beta-hCG is produced by syncytiotrophoblastic cells, present at highest levels in choriocarcinoma and also elevated in seminoma (up to 30% of cases, reflecting giant cell syncytiotrophoblastic differentiation). Mild elevation (<1,000 IU/L) can occur in pure seminoma and does not alter its management; markedly elevated beta-hCG (>5,000 IU/L) in a "seminoma" raises suspicion for occult NSGCT elements or choriocarcinoma. Serum half-life: 24–36 hours. Post-treatment monitoring of beta-hCG decline is critical — failure to normalize within 5–6 days post-orchiectomy predicts persistent disease.
Lactate Dehydrogenase (LDH)
LDH is a non-specific cellular enzyme elevated in many cancers but is included in the IGCCCG staging system as a prognostic marker. LDH reflects tumor bulk and cellular turnover. It is particularly useful when AFP and beta-hCG are uninformative (e.g., pure seminoma at advanced stage). LDH is incorporated into the IGCCCG risk classification (see Staging section) — specifically, LDH greater than 10× the upper limit of normal defines poor-prognosis NSGCT.
Marker Half-Life Kinetics and Clinical Interpretation
Post-orchiectomy marker decline must follow the expected half-life curves. Slower-than-expected decline suggests residual tumor burden and should trigger restaging with CT. Marker normalization does not exclude microscopic residual disease, particularly in NSGCT — staging CT and clinical risk factors (LVI, percentage embryonal carcinoma) continue to drive Stage I management decisions.
6. Diagnosis and Staging
Clinical Presentation
The most common presentation is a painless testicular mass or swelling, often noticed incidentally. Acute pain occurs in approximately 10% of cases (due to intratumoral hemorrhage or torsion). Systemic symptoms (back pain, cough, hemoptysis, gynecomastia, weight loss) may herald metastatic disease — retroperitoneal nodal involvement can compress the lumbar nerve roots or ureter.
Scrotal Ultrasound
High-frequency (7.5–15 MHz) scrotal ultrasound is the first-line imaging modality, with sensitivity exceeding 95% for testicular neoplasm detection. GCTs typically appear as hypoechoic intratesticular lesions with internal vascularity on Doppler. Ultrasound distinguishes intratesticular from extratesticular pathology, identifies non-palpable tumors, and evaluates the contralateral testis. A suspicious intratesticular lesion identified by ultrasound mandates radical inguinal orchiectomy, not fine-needle aspiration or transscrotal biopsy.
Radical Inguinal Orchiectomy
Radical inguinal orchiectomy — removal of the entire testis and spermatic cord to the level of the internal inguinal ring — is both the definitive diagnostic procedure and the primary therapeutic intervention. It is mandatory in the workup of any suspected testicular malignancy. Transscrotal biopsy or scrotal orchiectomy must never be performed, as violation of the scrotal skin disrupts lymphatic drainage from the inguinal to the pelvic/iliac lymph nodes, altering the metastatic pattern and potentially requiring scrotal radiotherapy.
Post-Orchiectomy Staging
Following orchiectomy, staging is completed with:
- CT chest/abdomen/pelvis with contrast: Standard for nodal and visceral staging. CT abdomen/pelvis evaluates retroperitoneal lymph nodes; CT chest evaluates pulmonary metastases. MRI brain is indicated in poor-prognosis NSGCT or neurological symptoms.
- Serum tumor markers (AFP, beta-hCG, LDH): Measured pre-orchiectomy and at defined intervals post-operatively. Marker half-life kinetics guide the pace of staging and treatment decisions.
- PET-CT: Not standard for initial staging. Has a specific role in post-chemotherapy residual seminoma masses (>3 cm) — FDG-PET at 6+ weeks post-chemotherapy predicts viable tumor in residual seminoma with sensitivity ~80% and specificity ~90%.
TNM Staging (AJCC 8th Edition)
Testicular cancer uses a unique TNM staging system incorporating serum marker levels (S category) as the fourth staging dimension: S0 (markers normal), S1 (mild elevation), S2 (moderate), S3 (high elevation). Stage grouping: Stage I (tumor confined to testis, markers normal or S1); Stage IIA-C (retroperitoneal nodal involvement); Stage IIIA-C (distant metastases or high markers).
IGCCCG Risk Stratification for Metastatic Disease
The International Germ Cell Cancer Collaborative Group (IGCCCG) classification stratifies metastatic GCT into good, intermediate, and poor prognosis groups based on histology, primary tumor site, metastatic sites, and marker levels. Good prognosis NSGCT (AFP <1,000, beta-hCG <5,000, LDH <1.5×ULN, no non-pulmonary visceral metastases): 5-year survival ~92%. Poor prognosis NSGCT (any non-pulmonary visceral mets, or AFP >10,000, beta-hCG >50,000, LDH >10×ULN): 5-year survival ~48%. All seminoma with good or intermediate prognosis only (no poor-prognosis seminoma by IGCCCG).
7. Treatment by Stage
Stage I Seminoma
With 5-year cancer-specific survival exceeding 99%, Stage I seminoma management focuses on minimizing long-term treatment toxicity while maintaining cure rates. Three evidence-based options exist:
- Surveillance (preferred for most patients): Approximately 15–20% of Stage I seminoma patients will relapse, typically in the retroperitoneum, within 2–3 years. All relapses are curable with chemotherapy or radiation. Active surveillance avoids treating 80–85% of patients unnecessarily. Requires compliance with follow-up imaging (CT abdomen/pelvis at defined intervals for 5 years).
- Adjuvant carboplatin (1 cycle, AUC 7): Reduces relapse risk to approximately 5% with a single chemotherapy infusion. Equivalent long-term outcomes to radiotherapy in randomized trials; preferred over RT due to lower secondary malignancy risk.
- Para-aortic radiotherapy (20 Gy in 10 fractions): Historically standard; now less preferred due to slightly elevated long-term risk of secondary gastrointestinal malignancies and cardiovascular disease. Still an option in selected patients.
Stage I Non-Seminomatous GCT (NSGCT)
Approximately 20–30% of Stage I NSGCT patients harbor occult retroperitoneal micrometastases not detectable on CT. Management options:
- Surveillance: Appropriate for low-risk Stage I NSGCT (no LVI, <50% embryonal carcinoma). Relapse rate approximately 15%; all relapses curable. Requires intensive CT follow-up.
- Primary retroperitoneal lymph node dissection (RPLND): Surgical staging and treatment; 10–30% of patients have pathological nodal disease (pN1). Provides definitive staging and avoids chemotherapy in pN0 patients. Nerve-sparing technique preserves antegrade ejaculation in >90%.
- 1 cycle BEP chemotherapy (bleomycin/etoposide/cisplatin): Reduces relapse rate to ~2% in high-risk Stage I NSGCT (LVI present). Preferred option for high-risk patients who decline RPLND or surveillance.
Stage IIA/B Seminoma
Stage IIA (nodes ≤2 cm): radiotherapy (30 Gy dog-leg field) or 3 cycles EP chemotherapy. Stage IIB (nodes 2–5 cm): radiotherapy (36 Gy) or 3 cycles BEP/4 cycles EP. For patients with multiple or bulky IIB nodes, chemotherapy is preferred.
Stage IIA/B NSGCT
Primary RPLND is a viable option for stage IIA NSGCT with normalized markers. For Stage IIB or marker-positive disease, 3 cycles BEP (good prognosis) or 4 cycles BEP is standard. Post-chemotherapy RPLND is performed for residual retroperitoneal masses exceeding 1 cm.
Metastatic Disease (Stage III)
BEP chemotherapy (bleomycin, etoposide, cisplatin) remains the gold standard systemic treatment for metastatic GCT, as established by the landmark Einhorn regimen (1977) and refined in subsequent trials. Current standard dosing:
- Good prognosis: 3 cycles BEP (bleomycin 30 units IV days 1, 8, 15; etoposide 100 mg/m² days 1–5; cisplatin 20 mg/m² days 1–5; 21-day cycle). Complete response rate ~70–80%; 5-year survival ~92%.
- Intermediate/poor prognosis: 4 cycles BEP or 4 cycles EP (if bleomycin contraindicated). Poor-prognosis patients may be candidates for investigational intensification strategies.
Salvage Therapy
Approximately 20–30% of metastatic patients relapse or are refractory to first-line BEP. Salvage options include:
- Conventional-dose salvage regimens: TIP (paclitaxel/ifosfamide/cisplatin) or VeIP (vinblastine/ifosfamide/cisplatin). Second-line complete response rates 15–40%.
- High-dose chemotherapy (HDCT) + autologous stem cell transplantation (ASCT): Carboplatin/etoposide-based HDCT with ASCT produces durable remissions in 20–40% of patients who relapsed after conventional salvage. Two sequential HDCT cycles (Indiana University or Memorial Sloan Kettering protocols) are used by specialized centers. TI-CE (paclitaxel/ifosfamide → carboplatin/etoposide) is a widely adopted HDCT regimen.
- Late relapses (>2 years post-complete response): Managed with surgical resection when possible, as late-relapse GCT is frequently chemorefractory.
Post-Chemotherapy Residual Masses
Following chemotherapy, residual masses are managed differently by histology:
- NSGCT residual >1 cm: Post-chemotherapy RPLND is mandatory to resect teratoma (chemoresistant) and viable tumor (requires additional chemotherapy). Approximately 10–15% of residual NSGCT masses contain viable tumor, 35–40% teratoma, and 45–50% necrosis/fibrosis.
- Seminoma residual >3 cm: FDG-PET at 6+ weeks post-chemotherapy. PET-positive residual requires biopsy or resection; PET-negative residual is observed.
8. Retroperitoneal Lymph Node Dissection (RPLND)
RPLND is a sophisticated urologic oncology procedure targeting the primary landing zone of testicular GCT — the retroperitoneal lymph nodes between the renal vessels superiorly and the common iliac bifurcation inferiorly. The primary nodal template for right-sided tumors includes interaortocaval, paracaval, and right para-aortic nodes; for left-sided tumors, left para-aortic and preaortic nodes.
Nerve-Sparing RPLND
The sympathetic nerve fibers responsible for antegrade ejaculation (emission) arise from the lumbar sympathetic chain (L1–L4) and converge at the hypogastric plexus anterior to the aortic bifurcation. Nerve-sparing RPLND — identifying and preserving these fibers under loupe magnification or surgical loupes — maintains antegrade ejaculation in more than 90% of patients undergoing primary (post-orchiectomy, pre-chemotherapy) RPLND. Post-chemotherapy RPLND carries higher rates of ejaculatory dysfunction (70–80% nerve sparing success) due to desmoplastic reaction around vessels and nerves.
Template Modifications
A modified unilateral template (as opposed to the full bilateral template) may be used in low-risk Stage I NSGCT patients undergoing primary RPLND, further reducing the risk of ejaculatory dysfunction while maintaining staging accuracy. However, bilateral template RPLND is required for post-chemotherapy resection and for patients with bulky retroperitoneal disease.
Minimally Invasive Approaches
Laparoscopic RPLND (L-RPLND) and robotic-assisted RPLND (R-RPLND) have been developed at high-volume centers as alternatives to open RPLND for carefully selected Stage I NSGCT patients. Advantages include shorter hospital stay, less blood loss, and faster recovery. Oncologic equivalence to open RPLND has been demonstrated in retrospective series and early prospective data from specialized centers. Patient selection is critical — post-chemotherapy robotic RPLND remains more technically challenging and is performed only at a small number of expert institutions.
Indications Summary
- Primary RPLND: Clinical Stage I high-risk NSGCT (surveillance-averse patient or LVI present); clinical Stage IIA NSGCT with normalized markers.
- Post-chemotherapy RPLND: Residual retroperitoneal mass >1 cm in NSGCT following BEP chemotherapy.
- Desperation/salvage RPLND: Growing teratoma syndrome or isolated late relapse in the retroperitoneum.
9. Complications
Chemotherapy-Related Toxicities
- Bleomycin pulmonary toxicity: The most feared acute complication of BEP. Occurs in approximately 3–5% of patients receiving standard BEP; risk increases with cumulative dose, age over 40, smoking, renal insufficiency, and supplemental oxygen exposure. Ranges from subclinical radiographic changes to fatal pulmonary fibrosis. Pulmonary function tests and diffusing capacity (DLCO) are monitored before each bleomycin dose. Bleomycin is omitted in EP regimens used for patients with compromised pulmonary reserve.
- Cisplatin nephrotoxicity: Cumulative platinum exposure causes a 20–30% reduction in GFR in many long-term survivors. Cisplatin irreversibly damages proximal tubular cells. Vigorous pre- and post-hydration mitigates but does not eliminate risk. Long-term survivors may develop progressive renal insufficiency decades after treatment.
- Cisplatin peripheral neuropathy: Sensory peripheral neuropathy (tingling, numbness in hands and feet) is dose-dependent and often permanent. Affects up to 50% of treated patients to varying degrees. Audiometric hearing loss (predominantly high-frequency) occurs in 20–40%.
- Carboplatin myelosuppression: Carboplatin (used in Stage I seminoma adjuvant treatment) causes dose-dependent thrombocytopenia and neutropenia. Generally well tolerated at the single AUC-7 dose used in Stage I seminoma.
- Etoposide secondary malignancies: Etoposide-associated secondary acute myeloid leukemia (t-AML) occurs in approximately 0.4% of patients, typically presenting 2–4 years post-treatment.
Surgical Complications
- Retrograde ejaculation post-RPLND: Results from disruption of the sympathetic nerves controlling bladder neck closure during emission. Occurs in 10–30% of nerve-sparing RPLND (higher in bilateral template and post-chemotherapy settings). Retrograde ejaculation causes dry orgasm but does not affect sexual function or libido. Anejaculation (complete absence of emission) is less common with nerve-sparing technique. Sperm retrieval from urine may allow biological fatherhood.
- Chylous ascites: Disruption of retroperitoneal lymphatic channels post-RPLND can cause lymphatic fluid accumulation; managed with medium-chain triglyceride diet and, rarely, somatostatin analogs or reoperation.
Endocrine Complications
- Hypogonadism: Occurs in 10–20% of testicular cancer survivors due to pre-existing testicular dysfunction, chemotherapy gonadotoxicity, or the removal of a solitary testis. Low testosterone levels contribute to fatigue, sexual dysfunction, metabolic syndrome, and osteoporosis. Annual testosterone monitoring is recommended for all survivors.
- Contralateral GCNIS: Approximately 5% of men with testicular GCT harbor GCNIS in the contralateral testis, detected by open biopsy. Left untreated, contralateral GCNIS progresses to invasive GCT in approximately 50% of patients over 5 years. Low-dose radiotherapy (18–20 Gy) to the remaining testis is curative but causes permanent azoospermia.
Radiation-Related Complications
Para-aortic radiotherapy for seminoma carries a long-term elevated risk of secondary gastrointestinal malignancies (stomach, bowel, pancreas), cardiovascular disease from aortic and coronary irradiation, and, with older field designs, contralateral testicular scatter causing infertility and Leydig cell dysfunction. Modern RT field designs and doses have substantially reduced (though not eliminated) these risks.
10. Fertility and Quality of Life
Sperm Banking
Sperm cryopreservation before any treatment (orchiectomy, chemotherapy, radiotherapy, or RPLND) is a mandatory quality-of-care standard for all men with testicular cancer of reproductive age. Many patients have compromised baseline sperm parameters — a consequence of the underlying testicular dysgenesis rather than prior treatment — making pre-treatment banking all the more urgent. Two to three sperm banking samples should be obtained before orchiectomy when possible, or within the interval before chemotherapy initiation. Sperm remain viable in cryopreservation for decades.
The majority of men who desire paternity after testicular cancer treatment are ultimately able to father children through natural conception (recovery of spermatogenesis post-chemotherapy occurs in most patients within 2–5 years) or assisted reproduction using cryopreserved sperm.
Testosterone Monitoring
Annual serum testosterone, LH, and FSH measurement is recommended for all testicular cancer survivors. Symptomatic hypogonadism warrants testosterone replacement therapy (TRT), which does not increase recurrence risk and significantly improves quality of life, body composition, bone density, and cardiovascular risk profile. The threshold for TRT initiation follows standard hypogonadism guidelines (morning testosterone <300 ng/dL with symptoms).
Psychological Impact
A cancer diagnosis in a young man — often during formative years of education, career, relationships, and family planning — carries profound psychological consequences. Fear of recurrence, body image concerns (particularly following orchiectomy and potential requirement for testicular prosthesis), sexual dysfunction, and relationship strain are common. Rates of anxiety and depression are elevated compared to age-matched controls, particularly in the first 2 years post-diagnosis. Access to psychological support, peer support networks, and survivorship clinics should be offered proactively.
Long-Term Cardiovascular Risk
Testicular cancer survivors who received cisplatin-based chemotherapy face a significantly elevated long-term cardiovascular risk, including increased rates of myocardial infarction, hypertension, hyperlipidemia, metabolic syndrome, and early-onset stroke. Cisplatin-induced endothelial dysfunction and atherosclerosis acceleration begin within months of treatment and persist for decades. Annual cardiovascular risk factor monitoring (blood pressure, lipid panel, fasting glucose, BMI) and aggressive lifestyle intervention are integral components of survivorship care in this population.
Testicular Prosthesis
Saline-filled testicular prostheses are available and can be placed at the time of orchiectomy or as a delayed procedure, providing cosmetic symmetry and psychological benefit. Patients should be counseled pre-operatively about prosthesis options; placement at the time of orchiectomy avoids a second surgical procedure and scar formation that may complicate later insertion.
11. Recent Research
RPLND vs surveillance for Stage IIA NSGCT: Ongoing prospective trials (TIGER, SEMS) are refining management of Stage IIA marker-negative NSGCT, exploring whether primary RPLND can achieve equivalent cure rates to BEP chemotherapy while reducing long-term toxicity burden. Early data support RPLND as a chemotherapy-sparing strategy in this setting at high-volume centers.
Checkpoint inhibitors in refractory GCT: Despite the high mutation burden not being a hallmark of GCT, programmed death-1 (PD-1) inhibitors (pembrolizumab, nivolumab) have been evaluated in platinum-refractory GCT. Response rates are modest (~15%) in unselected patients, and trials have not yet identified a predictive biomarker for response. Combination immunotherapy strategies and novel targets are under investigation in multiple international trials.
miR-371a-3p as a liquid biopsy GCT biomarker: MicroRNA-371a-3p (miR-371a-3p) has emerged as a highly sensitive and specific serum biomarker for active testicular GCT, detecting disease with sensitivity exceeding 90% and specificity above 95% — superior to conventional AFP/beta-hCG/LDH in many settings. miR-371a-3p is particularly valuable for: pure seminoma (which may produce no classic markers), teratoma surveillance (marker-negative by definition), and detection of occult retroperitoneal micrometastases in Stage I NSGCT. Commercial assay availability is expanding, and clinical integration into guidelines is anticipated in the near term.
Robotic RPLND expansion: Multi-institutional prospective data on robotic-assisted RPLND continue to accumulate, with several academic centers reporting oncologic outcomes comparable to open RPLND in primary Stage I NSGCT with significantly reduced morbidity. Standardization of surgical templates and certification criteria for robotic RPLND are active areas of guideline development.
Genetic risk stratification: Large-scale genome-wide association studies (GWAS) have identified more than 50 susceptibility loci for testicular GCT, with strongest associations at KITLG, SPRY4, BAK1, and DMRT1/DMRT3. These findings are advancing understanding of the heritable component of testicular cancer risk and may inform future screening strategies for high-risk families.
12. References
- Search PubMed — EAU guidelines on testicular cancer: 2011 update. Eur Urol.
- Einhorn LH et al., 1977 — PMID: 68987 — Cis-diamminedichloroplatinum, vinblastine, and bleomycin combination chemotherapy in disseminated testicular cancer. Ann Intern Med.
- de Wit R et al., 2001 — PMID: 11230476 — Equivalence of three or four cycles of bleomycin, etoposide, and cisplatin chemotherapy and of a 3- or 5-day schedule in good-prognosis germ cell cancer. J Clin Oncol.
- Search PubMed — Management of seminomatous testicular cancer: a binational prospective population-based study from the Swedish Norwegian Testicular Cancer Study Group. J Clin Oncol.
- Search PubMed — Prognostic factors for relapse in stage I seminoma managed by surveillance: a pooled analysis. J Clin Oncol.
- Stephenson AJ et al., 2005 — PMID: 15897577 — Retroperitoneal lymph node dissection for nonseminomatous germ cell testicular cancer: impact of patient selection factors on outcome. J Clin Oncol.
- International Germ Cell Cancer Collaborative Group, 1997 — PMID: 9060544 — International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol.
- Search PubMed — European consensus on diagnosis and treatment of germ cell cancer: a report of the European Germ Cell Cancer Consensus Group. Ann Oncol.
- PubMed: testicular cancer ultrasound diagnosis — Scrotal ultrasound imaging for testicular neoplasm diagnosis.
- Search PubMed — Testicular cancer: a new generation of biomarkers for non-invasive staging of intratubular germ cell neoplasia. Int J Androl.
- Travis LB et al., 2005 — PMID: 15713963 — Second cancers among 40,576 testicular cancer patients: focus on long-term survivors. J Natl Cancer Inst.
- Search PubMed — Testicular seminoma and non-seminoma: ESMO clinical practice guidelines. Ann Oncol.
Research Papers
- Testicular germ cell tumors — PubMed search
- BEP chemotherapy for testicular cancer — PubMed search
- Retroperitoneal lymph node dissection — PubMed search
- Stage I seminoma surveillance — PubMed search
- Cisplatin long-term toxicity in testicular cancer survivors — PubMed search
- miR-371a-3p biomarker in GCT — PubMed search
- Checkpoint inhibitors in refractory GCT — PubMed search
- Cryptorchidism and testicular cancer risk — PubMed search
Connections
- Urology
- Bladder Cancer
- Prostate Cancer
- Renal Cell Carcinoma
- Oncology
- Tumor Markers
- Benign Prostatic Hyperplasia
- Erectile Dysfunction
- Zinc