Renal Cell Carcinoma
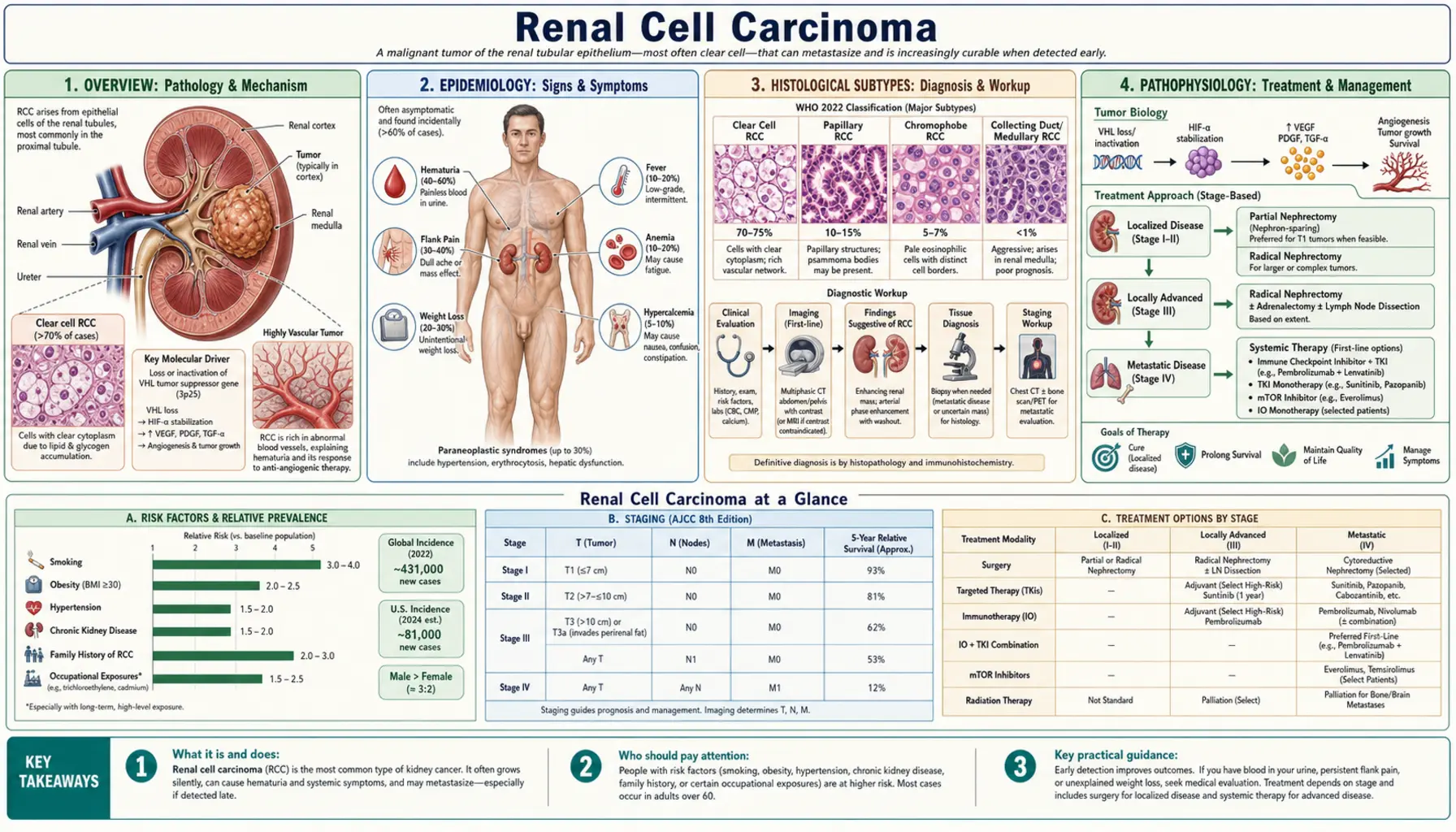
Table of Contents
- Overview
- Epidemiology
- Histological Subtypes
- Pathophysiology
- Paraneoplastic Syndromes
- Diagnosis and Staging
- Surgical Treatment
- Systemic Treatment
- Ablative and Stereotactic Therapies
- Complications
- Recent Research
- References
- Research Papers
- Connections
- Featured Videos
1. Overview
Renal Cell Carcinoma (RCC) is the most common malignancy arising from the kidney parenchyma in adults, accounting for approximately 90% of all kidney cancers and an estimated 80,000 new cases per year in the United States. It arises from the epithelial cells lining the renal tubules, and its biological behavior ranges from indolent incidental tumors to aggressive, rapidly metastatic disease.
Clear cell RCC (ccRCC) is the predominant histological subtype, comprising 75–80% of all cases. A defining molecular event in ccRCC is inactivation of the VHL (von Hippel-Lindau) tumor suppressor gene on chromosome 3p25, which drives a cascade of hypoxia-inducible factor (HIF) accumulation, angiogenesis, and metabolic reprogramming. Improved cross-sectional imaging has led to a dramatic rise in incidental detection of small, localized tumors, profoundly shifting the stage distribution toward earlier, potentially curable disease.
2. Epidemiology
RCC demonstrates a striking male predominance, with a male-to-female ratio of approximately 2:1. Peak incidence occurs in the sixth and seventh decades of life, though hereditary forms (VHL disease, hereditary papillary RCC, Birt-Hogg-Dubé syndrome) present earlier. Incidence rates in the United States have risen steadily over the past four decades, driven in part by widespread use of abdominal CT and ultrasound imaging detecting asymptomatic tumors.
Racial and ethnic disparities are notable: Black Americans have higher incidence rates than white Americans, potentially related to higher prevalence of hypertension, obesity, and kidney disease. Stage-specific five-year survival varies dramatically: approximately 93% for stage I (localized, ≤7 cm), 75% for stage II, 55% for stage III (regional lymph node involvement or major venous extension), and 13% for stage IV (distant metastases). Obesity, cigarette smoking, hypertension, and end-stage renal disease are the most consistently identified modifiable risk factors.
3. Histological Subtypes
The 2022 WHO Classification of Urinary and Male Genital Tumors recognizes multiple histologically and molecularly distinct RCC subtypes:
Clear Cell RCC (ccRCC)
The most common subtype (75–80%), characterized by cells with abundant clear or eosinophilic cytoplasm, a delicate vascular network, and prominent lipid/glycogen content. Biallelic inactivation of the VHL gene (chromosome 3p25) is present in over 90% of sporadic ccRCC, whether through mutation, loss of heterozygosity, or promoter methylation. Secondary somatic mutations in epigenetic regulators (PBRM1, BAP1, SETD2, KDM5C) further shape prognosis and treatment sensitivity.
Papillary RCC
The second most common subtype (10–15%), sub-classified into type 1 (low grade, associated with MET proto-oncogene gain-of-function mutations, often multifocal) and type 2 (higher grade, associated with FH gene mutations causing hereditary leiomyomatosis and RCC syndrome, and a generally more aggressive clinical course). Type 2 papillary RCC carries a significantly worse prognosis than type 1.
Chromophobe RCC
Comprising approximately 5% of RCC, chromophobe tumors arise from the cortical collecting duct intercalated cells. They typically follow an indolent course with excellent prognosis in localized disease. Mutations in the FLCN gene cause the hereditary Birt-Hogg-Dubé syndrome, which predisposes to chromophobe RCC (and oncocytomas). TP53 mutations are the most frequent somatic alterations in sporadic chromophobe RCC.
Collecting Duct Carcinoma
A rare and highly aggressive subtype (<1%) arising from the principal cells of the medullary collecting duct. It presents at advanced stage and responds poorly to standard systemic therapies, with a median survival under 12 months. Gemcitabine-based chemotherapy regimens are used empirically.
Translocation RCC (MiT Family)
Characterized by chromosomal translocations involving the TFE3 gene (Xp11 translocation) or, less commonly, TFEB (t(6;11)). Disproportionately affects children and young adults and may masquerade histologically as clear cell or papillary RCC. TFE3 IHC staining or FISH confirms the diagnosis.
Renal Oncocytoma
A benign renal tumor composed of large oncocytic cells with granular eosinophilic cytoplasm packed with mitochondria. Distinguishing oncocytoma from chromophobe RCC on imaging alone is unreliable; both may appear identical on CT or MRI. Biopsy can be informative but occasionally inconclusive. Oncocytomas are managed with active surveillance in appropriate candidates.
4. Pathophysiology
The molecular pathogenesis of ccRCC centers on the VHL-HIF axis and downstream oncogenic signaling:
VHL–HIF Axis
The VHL protein forms an E3 ubiquitin ligase complex that targets hypoxia-inducible factor-1α (HIF-1α) and HIF-2α for proteasomal degradation under normoxic conditions. Loss of VHL function causes constitutive accumulation of HIF-1α and HIF-2α, which transactivate hundreds of hypoxia-response genes including VEGF, PDGF, EPO, GLUT1, and LDHA. The result is a pseudohypoxic state driving tumor angiogenesis, erythropoiesis, and the Warburg metabolic shift toward aerobic glycolysis.
VEGF and Angiogenesis
Constitutive VEGF overproduction makes ccRCC among the most vascular of all solid tumors, explaining the dramatic efficacy of VEGF-receptor (VEGFR) tyrosine kinase inhibitors (TKIs) in metastatic disease. VEGF-A binds VEGFR-2 on endothelial cells, activating RAS-MAPK and PI3K-AKT-mTOR proliferative and survival pathways.
mTOR Pathway
Activation of the mechanistic target of rapamycin (mTOR) complex occurs through PIK3CA amplification, PTEN loss, and TSC1/TSC2 mutations — the latter responsible for tuberous sclerosis-associated angiomyolipomas. mTOR complex 1 (mTORC1) promotes cap-dependent translation of HIF-1α and other oncoproteins, providing a therapeutic target for rapalogs (everolimus, temsirolimus).
Epigenetic Dysregulation
PBRM1 (SWI/SNF chromatin remodeling complex) is the second most frequently mutated gene in ccRCC after VHL, lost in ~40% of tumors. BAP1 mutations (deubiquitinase) occur in ~10–15% of ccRCC and are associated with higher grade and worse prognosis. SETD2 (H3K36 methyltransferase) mutations impair homologous recombination DNA repair and confer increased mutational burden. The pattern of epigenetic co-mutation stratifies prognosis independent of stage and grade.
Metabolic Reprogramming
ccRCC exhibits striking metabolic abnormalities including suppressed TCA cycle activity, glutamine dependence, accumulation of lipids, and altered amino acid metabolism — reflecting both HIF-driven transcriptional changes and cell-autonomous metabolic adaptations that support rapid proliferation. These vulnerabilities are being exploited in emerging therapeutic approaches.
5. Paraneoplastic Syndromes
RCC is classically associated with a broad spectrum of paraneoplastic manifestations mediated by tumor-secreted hormones, cytokines, and immune-complex deposition. These syndromes may precede the diagnosis of RCC or signal recurrence:
- Erythrocytosis: Excess EPO secretion by tumor cells causes polycythemia in 3–5% of patients. Hematocrit elevation may be the presenting finding prompting kidney imaging.
- Hypercalcemia: Present in 20–30% of patients at diagnosis, attributable to ectopic PTHrP secretion or tumor production of 1,25-dihydroxyvitamin D. Severe hypercalcemia (>14 mg/dL) requires urgent treatment with IV fluids, bisphosphonates, and denosumab. Hypercalcemia resolves with successful tumor resection but recurs with relapse.
- Stauffer Syndrome: Non-metastatic hepatic dysfunction (elevated alkaline phosphatase, transaminases, prolonged prothrombin time, hypoalbuminemia) without hepatic metastases, caused by tumor-secreted IL-6. Resolves after nephrectomy and may recur with relapse — a useful marker of tumor activity.
- Hypertension: Tumor-derived renin or direct compression of the renal artery drives secondary hypertension in a subset of patients. Nephrectomy may normalize blood pressure.
- Fever and Constitutional Symptoms: Intermittent fever, night sweats, weight loss, and anorexia (the classic "B symptoms") reflect IL-6, IL-1, and TNF-α secretion. Present in up to 20% of patients at diagnosis and associated with advanced disease.
- Amyloidosis: Secondary (AA) amyloidosis from chronic tumor-derived serum amyloid A is a rare but recognized paraneoplastic complication, affecting kidneys, liver, and spleen.
- Neuromyopathies: Peripheral neuropathy, polymyositis, and cerebellar degeneration have been described, mediated by cross-reactive anti-tumor antibodies targeting neural antigens.
6. Diagnosis and Staging
Imaging
Multiphasic CT abdomen and pelvis with and without contrast is the cornerstone of RCC diagnosis and staging. Enhancement of a renal mass by more than 15–20 Hounsfield units (HU) on contrast-enhanced CT is the standard threshold for malignancy. Four phases are obtained: unenhanced, corticomedullary (arterial), nephrographic (parenchymal), and excretory (delayed). MRI with gadolinium is preferred for characterizing complex cystic masses (Bosniak classification), assessing inferior vena cava (IVC) thrombus extent (level I: below renal vein; II: below hepatic veins; III: above hepatic veins; IV: supradiaphragmatic or cardiac), and in patients with iodinated contrast allergy or renal impairment.
Nephrometry Scoring
The RENAL (Radius, Exophytic/Endophytic, Nearness to collecting system, Anterior/posterior, Location) and PADUA scoring systems quantify tumor complexity and predict surgical difficulty, complication risk, and functional outcomes. Scores guide selection between radical and partial nephrectomy and between open and minimally invasive approaches.
Biopsy
Percutaneous CT-guided or ultrasound-guided biopsy is indicated before systemic therapy for presumed metastatic disease, prior to ablative treatment of small renal masses, and when lymphoma, metastasis from another primary, or abscess cannot be excluded on imaging. Core needle biopsy has a diagnostic yield exceeding 90% with low complication rates (<2% significant bleeding). Biopsy is generally not required before surgical resection of a solid enhancing renal mass in a surgical candidate.
Pathological Grading
The WHO/ISUP (International Society of Urological Pathology) nuclear grading system (grades 1–4, based on nucleolar prominence) has supplanted the Fuhrman grading system and is the current standard. Grade 4 includes sarcomatoid and rhabdoid differentiation, both associated with markedly worse prognosis and emerging immunotherapy sensitivity.
TNM Staging
AJCC 8th edition staging: T1a (≤4 cm, organ-confined), T1b (4–7 cm), T2a (7–10 cm), T2b (>10 cm), T3a (renal vein/segmental branch invasion or perinephric fat invasion), T3b (IVC below diaphragm), T3c (IVC above diaphragm or in pericardium), T4 (beyond Gerota's fascia). N1 = regional lymph node metastasis. M1 = distant metastasis.
IMDC Risk Score
The International Metastatic RCC Database Consortium (IMDC) model stratifies metastatic RCC patients into favorable (0 factors), intermediate (1–2 factors), and poor risk (≥3 factors) groups based on six adverse prognostic variables: KPS <80%, time from diagnosis to systemic therapy <12 months, hemoglobin below normal, corrected calcium above normal, neutrophils above normal, and platelets above normal. IMDC risk guides first-line treatment selection (favorable vs. intermediate/poor) and is embedded in all major clinical trial eligibility criteria.
7. Surgical Treatment
Nephron-Sparing Partial Nephrectomy
Partial nephrectomy (PN) is the preferred treatment for T1 tumors (≤7 cm) and is strongly favored for patients with a solitary kidney, bilateral tumors, hereditary RCC syndromes, baseline chronic kidney disease (CKD), or diabetes. PN achieves equivalent oncological outcomes to radical nephrectomy for T1a tumors (≤4 cm) while preserving nephrons, reducing risk of de novo CKD, cardiovascular events, and all-cause mortality. Warm ischemia time should ideally be kept under 25 minutes; "off-clamp" techniques are increasingly used to eliminate ischemia entirely. Robotic-assisted PN has largely supplanted open PN at high-volume centers due to reduced blood loss, shorter hospital stay, and faster recovery.
Radical Nephrectomy
Radical nephrectomy (RN) — removal of the kidney within Gerota's fascia — is indicated for T2 tumors (>7 cm), hilar tumors where partial resection is technically infeasible, and T3/T4 disease. Adrenalectomy is reserved for radiographic evidence of adrenal involvement; routine adrenalectomy has been abandoned. Regional lymph node dissection does not improve survival in clinically N0 patients but provides staging information. Minimally invasive (laparoscopic or robotic) RN is preferred when feasible; open RN is required for very large tumors, IVC level III-IV thrombus, or major vascular reconstruction.
IVC Thrombectomy
RCC-associated IVC tumor thrombus occurs in 4–10% of patients. Surgical removal requires cardiothoracic collaboration for level III (suprarenal infrahepatic) and level IV (supradiaphragmatic) thrombus, including cardiopulmonary bypass for the highest level IV cases. Despite the surgical complexity, IVC thrombectomy in the absence of distant metastases confers five-year survival rates of 40–65%, making aggressive surgical resection worthwhile in appropriate candidates.
Cytoreductive Nephrectomy in Metastatic Disease
The survival benefit of cytoreductive nephrectomy (CN) in the targeted therapy era has been substantially narrowed by the CARMENA trial, which demonstrated that sunitinib alone was non-inferior to CN followed by sunitinib in intermediate- and poor-risk IMDC patients. CN remains appropriate for favorable-risk patients, those with excellent performance status, minimal metastatic burden, symptoms attributable to the primary tumor, or pending immunotherapy combinations where tumor debulking may enhance response.
8. Systemic Treatment
Historical: High-Dose IL-2
High-dose interleukin-2 (IL-2) was the first active systemic therapy for metastatic RCC approved by the FDA (1992), producing durable complete responses in 5–7% of patients. However, its extreme toxicity profile (capillary leak syndrome, hypotension, arrhythmia, renal and hepatic dysfunction) requires intensive care unit administration and limits use to centers with specialized expertise. IL-2 continues to be used at a few academic centers in highly selected patients.
VEGFR Tyrosine Kinase Inhibitors (TKIs)
The landmark phase III trial by Motzer et al. (2007, PMID: 17215529) established sunitinib — a multi-target VEGFR/PDGFR TKI — as first-line standard of care over interferon-α, with superior progression-free survival (11 vs. 5 months) and overall survival. Subsequent approvals followed for pazopanib, axitinib, and cabozantinib. Cabozantinib, which targets VEGFR-2, MET, and AXL, demonstrated improved PFS and OS over sunitinib in the CABOSUN trial in intermediate/poor-risk patients. TKI class effects include hypertension, hand-foot skin reaction, fatigue, diarrhea, and mucositis.
mTOR Inhibitors
Temsirolimus (IV mTORC1 inhibitor) improved OS versus interferon in poor-prognosis metastatic RCC. Everolimus (oral mTORC1 inhibitor) demonstrated PFS benefit after TKI failure. In the era of immunotherapy combinations, mTOR inhibitors are used primarily as second- or third-line therapy after IO/TKI combinations.
Immune Checkpoint Inhibitors
Nivolumab (anti-PD-1) demonstrated OS benefit over everolimus in pre-treated ccRCC (CheckMate 025, 2015), marking the first OS improvement in second-line RCC. This established PD-1 blockade as a cornerstone of RCC treatment. Pembrolizumab (anti-PD-1) received adjuvant approval based on KEYNOTE-564 data.
Combination Regimens — Current Standard of Care
- Nivolumab + ipilimumab (CheckMate 214, PMID: 29562145): The combination of PD-1 and CTLA-4 blockade significantly improved OS, PFS, and objective response rate versus sunitinib in intermediate- and poor-risk IMDC patients, with durable complete responses in ~10%. First-line standard of care for intermediate/poor-risk metastatic ccRCC.
- Pembrolizumab + axitinib (KEYNOTE-426, PMID: 30779529): Improved OS (hazard ratio 0.68) and PFS across all IMDC risk groups versus sunitinib; FDA-approved for first-line metastatic RCC regardless of risk category.
- Nivolumab + cabozantinib (CheckMate 9ER, PMID: 33657295): Superior PFS (16.6 vs. 8.3 months), OS (HR 0.70), and ORR (55.7% vs. 27.1%) vs. sunitinib; FDA-approved for first-line metastatic RCC. Cabozantinib's MET/AXL inhibition may overcome TKI resistance mechanisms.
- Pembrolizumab + lenvatinib: CLEAR trial demonstrated the longest median PFS (23.9 months) of any combination regimen vs. sunitinib; approved for first-line metastatic RCC.
- Avelumab + axitinib (JAVELIN Renal 101): Improved PFS in PD-L1+ subgroup; FDA-approved option for first-line metastatic RCC.
Treatment selection among these regimens is informed by IMDC risk, histology, contraindications to immunotherapy (autoimmune disease, organ transplant), and center preference. Non-ccRCC subtypes (papillary, chromophobe) respond less reliably to VEGFR TKIs and IO; clinical trial enrollment is strongly encouraged.
9. Ablative and Stereotactic Therapies
Thermal Ablation
Radiofrequency ablation (RFA) and cryoablation are guideline-endorsed alternatives to partial nephrectomy for clinical T1a (≤4 cm) tumors in patients with high surgical risk due to age, comorbidities, or limited renal reserve. CT- or MRI-guided percutaneous delivery is most common; laparoscopic approaches are used for posterior and hilar lesions. Five-year local recurrence-free survival rates of 90–95% for RFA and 90%+ for cryoablation are reported in experienced centers. Cryoablation may be preferred for tumors near the collecting system or ureter, as ice-ball formation is more precisely controlled than RF heating. Biopsy is obtained before or at the time of ablation to establish histological diagnosis.
Active Surveillance
For incidentally detected cT1a tumors (<4 cm, particularly <2 cm) in elderly or heavily comorbid patients, active surveillance with serial cross-sectional imaging every 3–6 months is an accepted management strategy. Growth rates are typically slow (0.1–0.5 cm/year for small renal masses), metastatic progression is rare during observation (<2%), and delayed intervention is feasible. The risk of over-treatment of benign lesions (oncocytoma, angiomyolipoma) — comprising up to 20–25% of resected small renal masses — strengthens the argument for surveillance in appropriate patients.
Stereotactic Body Radiotherapy (SBRT/SABR)
Historically considered radioresistant, RCC primary tumors can be effectively ablated with stereotactic radiotherapy delivering high biologically effective doses in 3–5 fractions. SBRT for primary RCC achieves local control rates exceeding 95% in published series and is being evaluated prospectively in patients who are non-surgical candidates. For metastatic RCC, SBRT to oligometastatic sites (≤3–5 lesions) has been associated with delayed systemic therapy initiation and improved outcomes in retrospective studies, supporting a growing role for local ablation within the systemic therapy paradigm.
10. Complications
- Metastatic spread: The lung is the most common site of distant metastasis (50–60%), followed by bone (30–40%), liver (20–30%), brain (5–10%), and adrenal gland. Bone metastases cause pain, pathological fractures, and spinal cord compression; bisphosphonates and denosumab reduce skeletal-related events. Brain metastases are treated with stereotactic radiosurgery or whole-brain radiation.
- Paraneoplastic crises: Severe hypercalcemia (>13 mg/dL) can cause lethargy, coma, acute kidney injury, and cardiac arrhythmias requiring emergency IV hydration, calcitonin, and bisphosphonate or denosumab administration.
- TKI toxicities: Hypertension (60–70%, often requiring pharmacological management), hand-foot skin reaction (HFS, dose-limiting in 10–20%), fatigue, diarrhea, hypothyroidism, hepatotoxicity, and wound healing impairment. Hypertension control is particularly important as TKI-induced hypertension may predict anti-VEGF activity and outcomes.
- Immune-related adverse events (irAEs): Anti-PD-1 and anti-CTLA-4 agents cause immune-mediated toxicities including pneumonitis, colitis, hepatitis, endocrinopathies (thyroid dysfunction, adrenal insufficiency, hypophysitis, type 1 diabetes), nephritis, and dermatitis. The combination of nivolumab + ipilimumab yields higher rates of grade 3–4 irAEs (46%) than either agent alone. Most irAEs are managed with immunosuppression (high-dose corticosteroids); severe cases require permanent therapy discontinuation.
- Post-nephrectomy CKD: Radical nephrectomy reduces functioning nephron mass by approximately 50%, conferring risk of stage 3+ CKD in patients with pre-existing contralateral kidney disease, diabetes, or hypertension. CKD is associated with accelerated cardiovascular disease and reduced quality-adjusted life expectancy, motivating nephron-sparing approaches whenever oncologically safe.
- Venous thromboembolism: Active malignancy substantially increases VTE risk; RCC patients receiving VEGFR TKIs have additional arterial thromboembolic risk (myocardial infarction, cerebrovascular accident, 1–3%).
11. Recent Research
Belzutifan (HIF-2α inhibitor): Belzutifan (PT2977) is the first selective HIF-2α inhibitor approved by the FDA (2021) for VHL disease-associated RCC, hemangioblastomas, and pancreatic neuroendocrine tumors (PMID: 34818478). By blocking HIF-2α-ARNT dimerization, belzutifan suppresses VEGF transcription independent of VHL status. Ongoing phase III trials (LITESPARK-005, LITESPARK-011) are evaluating belzutifan in sporadic ccRCC as second-line monotherapy and in combination with cabozantinib, representing a mechanistically distinct treatment axis beyond VEGFR inhibition and immune checkpoint blockade.
Adjuvant immunotherapy: KEYNOTE-564 (PMID: 36706745) demonstrated that adjuvant pembrolizumab for 1 year significantly improved disease-free survival (hazard ratio 0.63) in patients with high-risk ccRCC after nephrectomy — the first systemic agent to demonstrate DFS benefit in the adjuvant setting for RCC. Subgroup analyses suggest the greatest benefit in M1 NED (no evidence of disease) and T3 node-negative high-grade patients. Long-term OS data remain immature. Adjuvant pembrolizumab is now FDA-approved for intermediate-high or high-risk ccRCC following complete resection.
Liquid biopsy and ctDNA: Circulating tumor DNA (ctDNA) detection in plasma is being investigated as a minimally invasive tool for early recurrence detection after nephrectomy, monitoring therapeutic response, identifying resistance mutations, and resolving diagnostic uncertainty in radiologically indeterminate lesions. Sensitivity remains limited in localized RCC due to low tumor DNA shedding, but is higher in advanced metastatic disease.
Metabolic targeting: TCGA metabolomic profiling of ccRCC (PMID: 26853177) revealed profound suppression of the tricarboxylic acid (TCA) cycle and oxidative phosphorylation, with compensatory glutamine and fatty acid metabolism. Glutaminase inhibitors (CB-839/telaglenastat) in combination with cabozantinib are under clinical investigation. GLUT1 inhibitors targeting the HIF-driven glucose uptake phenotype are in preclinical development.
Tumor microenvironment and resistance: Single-cell RNA sequencing of ccRCC tumors has revealed the composition and functional states of tumor-infiltrating immune cells, identifying exhausted T-cell subsets, immunosuppressive myeloid populations, and regulatory T-cells as mediators of checkpoint inhibitor resistance. Strategies to overcome microenvironment-mediated immunosuppression — including LAG-3, TIGIT, and TIM-3 co-inhibitory pathway blockade — are in clinical trials.
12. References
- Siegel RL, Miller KD, Jemal A., 2023 — PMID: 36633525. Cancer statistics, 2023. CA Cancer J Clin.
- Motzer RJ, Hutson TE, Tomczak P, et al., 2007 — PMID: 17215529. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med.
- Motzer RJ, Tannir NM, McDermott DF, et al., 2018 — PMID: 29562145. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med.
- Rini BI, Plimack ER, Stus V, et al., 2019 — PMID: 30779529. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med.
- Jonasch E, Donskov F, Iliopoulos O, et al., 2021 — PMID: 34818478. Belzutifan for renal cell carcinoma in von Hippel-Lindau disease. N Engl J Med.
- Search PubMed. The epidemiology of renal cell carcinoma. Eur Urol.
- Choueiri TK, Powles T, Burotto M, et al., 2021 — PMID: 33657295. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med.
- Linehan WM, Spellman PT, Ricketts CJ, et al., 2016 — PMID: 26536169. Comprehensive molecular characterization of papillary renal-cell carcinoma. N Engl J Med.
- Ravaud A, Motzer RJ, Pandha HS, et al., 2016 — PMID: 27718781. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N Engl J Med.
- Search PubMed. Pembrolizumab versus placebo as post-nephrectomy adjuvant therapy for clear-cell renal cell carcinoma. N Engl J Med.
- Search PubMed. An integrated metabolic atlas of clear cell renal cell carcinoma. Cancer Cell.
- Search PubMed. Systemic therapy for metastatic renal-cell carcinoma. N Engl J Med.
Research Papers
- Immunotherapy combinations for metastatic RCC — PubMed search
- VHL gene and clear cell RCC — PubMed search
- Belzutifan (HIF-2α inhibitor) for RCC — PubMed search
- Partial vs. radical nephrectomy outcomes — PubMed search
- Nivolumab + ipilimumab in RCC (CheckMate trials) — PubMed search
- SBRT for renal cell carcinoma — PubMed search
- VEGFR TKIs in kidney cancer — PubMed search
- Paraneoplastic syndromes in RCC — PubMed search
Connections
- Urology
- Bladder Cancer
- Testicular Cancer
- Kidney Stones
- Benign Prostatic Hyperplasia
- Diabetes
- Urinary Tract Infections
- Urinalysis
- Interstitial Cystitis
- Urinary Incontinence
- Oncology