Bladder Cancer
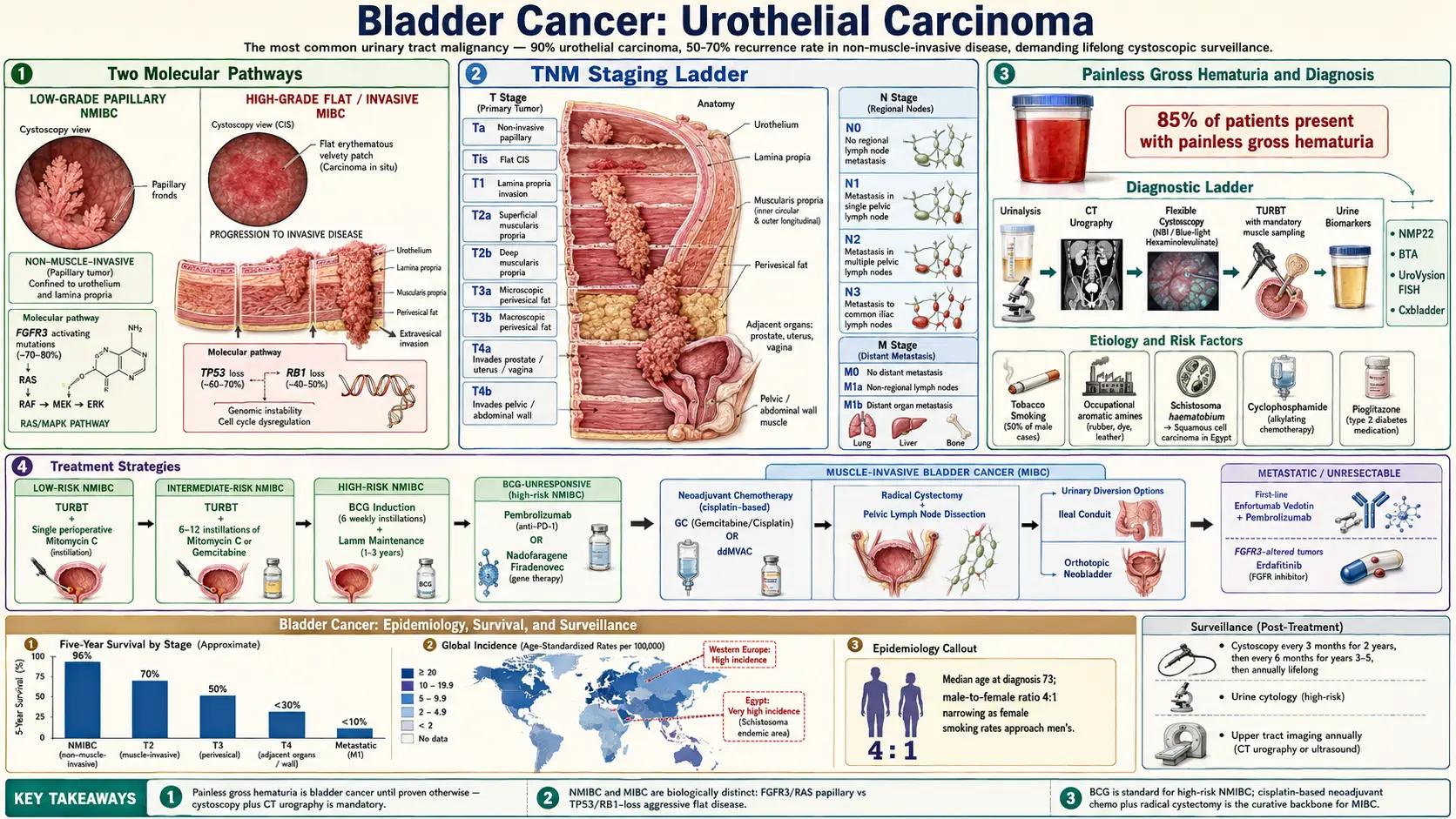
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation and TNM Staging
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research
- References
- Connections
- Featured Videos
1. Overview
Bladder cancer is the sixth most common cancer in the United States and the most common malignancy of the urinary tract. The vast majority — approximately 90% — are urothelial carcinomas (formerly called transitional cell carcinoma, TCC), arising from the urothelial lining that lines the bladder, ureters, and renal pelvis. The remaining histologic subtypes include squamous cell carcinoma (SCC), which accounts for 3–5% of cases in Western countries (associated with chronic catheterization, recurrent infections, and schistosomiasis in endemic regions), and adenocarcinoma (less than 2%), arising from urachal remnants or metaplastic urothelium.
The most clinically important distinction is between non-muscle-invasive bladder cancer (NMIBC) — confined to the mucosa (Ta, T1) or carcinoma in situ (CIS, Tis) — and muscle-invasive bladder cancer (MIBC), which has penetrated the detrusor muscle (T2 and beyond). Approximately 75% of newly diagnosed bladder cancers are NMIBC. Although NMIBC is generally not life-threatening at diagnosis, it carries high recurrence rates (50–70%) and a 10–30% risk of progression to MIBC over time. The hallmark presenting symptom of bladder cancer at any stage is painless gross hematuria, which should prompt urgent urological evaluation.
2. Epidemiology
In the United States, approximately 83,190 new bladder cancer cases and 16,840 deaths were estimated for 2024, according to the American Cancer Society. Bladder cancer has a striking male predominance, with a male-to-female ratio of approximately 3–4:1; men have a lifetime risk of approximately 1 in 27 compared with 1 in 89 for women. Despite the higher incidence in men, women are often diagnosed at later stages, contributing to relatively worse sex-adjusted outcomes.
The incidence rises sharply with age: more than 90% of cases occur in patients older than 55, with a median age at diagnosis of approximately 73 years. White Americans have a higher incidence than Black Americans, though Black patients present with more advanced disease and have worse stage-adjusted survival — disparities attributed to differences in access to care, tumor biology, and diagnostic delay. Globally, bladder cancer incidence is highest in Egypt (where SCC driven by Schistosoma haematobium infestation is endemic), Southern and Western Europe, and North America.
Cigarette smoking is the single most important modifiable risk factor, attributable to approximately 50% of cases in men and 35% in women. The relative risk for current smokers is 2.5–4 times that of never-smokers, with a dose-dependent relationship to pack-year exposure. Risk decreases progressively after smoking cessation, reaching background levels by approximately 15 years of abstinence.
3. Pathophysiology
Bladder carcinogenesis follows two major molecular pathways that correspond to distinct clinical and histologic trajectories:
Luminal/Papillary Pathway (Low-Grade Ta)
The majority of urothelial carcinomas arise via the papillary pathway, initiated by activating mutations in the FGFR3 (fibroblast growth factor receptor 3) gene or the HRAS oncogene, leading to constitutive RAS-MAPK signaling, cellular proliferation, and exophytic papillary tumor growth. These tumors are typically low-grade, non-invasive (Ta), have intact lamina propria, and harbor relatively few additional somatic mutations. Loss of chromosome 9 (del9q) is the earliest and most common cytogenetic event in this pathway. Despite high recurrence rates — mediated partly by intraluminal tumor cell implantation during TURBT — progression to MIBC is uncommon (less than 5% for pure low-grade Ta disease).
CIS/Invasive Pathway (High-Grade T1/MIBC)
High-grade disease, including CIS and invasive tumors, follows a fundamentally different pathway characterized by early TP53 mutation and loss of the RB1 (retinoblastoma) tumor suppressor, leading to genomic instability, aneuploidy, and accumulation of multiple somatic alterations. CIS is a flat, high-grade intraepithelial lesion with severely dysplastic cells and absent normal urothelial differentiation. It is a precursor to T1 and MIBC and carries a 50–80% risk of progression to muscle-invasive disease if untreated. MIBC is further characterized by E-cadherin loss, epithelial-mesenchymal transition (EMT), activation of PI3K/AKT/mTOR pathways, and frequent alterations in ARID1A, KDM6A, and chromatin-remodeling genes identified through The Cancer Genome Atlas (TCGA) bladder cancer dataset.
Tumor Microenvironment and Immune Evasion
Urothelial carcinomas typically display high somatic tumor mutational burden (TMB), particularly in smoking-associated tumors where tobacco-related mutational signatures predominate. High TMB correlates with neoantigen load and predicts responsiveness to immune checkpoint inhibitor therapy. PD-L1 expression on tumor cells and tumor-infiltrating immune cells provides an important but imperfect biomarker for anti-PD-1/PD-L1 response. The TCGA molecular subtypes of MIBC — luminal papillary, luminal non-specified, luminal unstable, stroma-rich, basal/squamous, and neuroendocrine-like — correspond to distinct clinical behaviors and potential therapeutic vulnerabilities.
4. Etiology and Risk Factors
- Cigarette smoking (primary risk factor): Responsible for approximately 50% of bladder cancers in men and 35% in women. Tobacco smoke contains multiple aromatic amines (2-naphthylamine, 4-aminobiphenyl) and polycyclic aromatic hydrocarbons that are excreted in urine after hepatic N-hydroxylation, exposing the urothelium to carcinogenic metabolites for prolonged periods. Risk is dose-dependent; cessation reduces risk progressively over 10–15 years.
- Occupational aromatic amine exposure: Workers in dye manufacturing, rubber vulcanization, leather tanning, aluminum smelting, truck driving, and hairdressing have elevated bladder cancer risk due to chronic exposure to 2-naphthylamine, benzidine, 4-aminobiphenyl, and 4-chloro-o-toluidine. Occupational exposures account for approximately 20–25% of cases and often have long latency periods (20–40 years).
- Schistosoma haematobium infection: In endemic regions (sub-Saharan Africa, Egypt, Middle East), chronic S. haematobium infestation causes granulomatous bladder inflammation, urothelial dysplasia, and squamous metaplasia, predisposing to SCC rather than urothelial carcinoma. Schistosomiasis-associated SCC accounts for the majority of bladder cancer in Egypt, where it presents at a younger age than Western urothelial carcinoma.
- Chronic catheterization and recurrent UTIs: Long-term indwelling urinary catheters in patients with spinal cord injuries or chronic urinary retention induce persistent bladder irritation, squamous metaplasia, and SCC risk. Recurrent urinary tract infections independently contribute, though the association with urothelial carcinoma is weaker than with SCC.
- Lynch syndrome (hereditary nonpolyposis colorectal cancer, HNPCC): Mismatch repair gene defects (MLH1, MSH2, MSH6, PMS2) confer a 4–16-fold elevated urothelial tract cancer risk (upper tract greater than bladder). Lynch syndrome-associated bladder cancers tend to present at younger ages and have high microsatellite instability (MSI-H), which predicts exceptional responsiveness to pembrolizumab.
- Radiation therapy to the pelvis: Prior pelvic irradiation for prostate, cervical, rectal, or uterine cancer increases bladder cancer risk 2–4-fold, with a latency of 5–10 years. Radiation-induced bladder cancer is often high-grade at presentation.
- Cyclophosphamide chemotherapy: The toxic acrolein metabolite of cyclophosphamide is excreted in urine, causing hemorrhagic cystitis and bladder carcinogenesis; mesna co-administration substantially reduces but does not eliminate this risk.
- Aristolochic acid (herbal nephropathy): Aristolochic acids found in Aristolochia plant species (used in traditional Chinese herbal remedies) cause a distinct aristolochic acid mutational signature (COSMIC SBS22) and are strongly associated with upper tract urothelial carcinoma, with bladder cancer risk also elevated.
5. Clinical Presentation and TNM Staging
Painless gross hematuria is the hallmark presentation of bladder cancer, occurring in approximately 80–85% of patients. The hematuria is typically intermittent and may resolve spontaneously, which can falsely reassure patients and delay diagnosis. Microscopic hematuria (more than 3 red blood cells per high-power field on two of three properly collected specimens) carries a lower but meaningful risk of underlying malignancy and warrants urological evaluation in appropriate clinical contexts. Irritative voiding symptoms — frequency, urgency, and dysuria without infection — are characteristic of CIS and high-grade disease, occurring in 20–30% of patients.
TNM Staging
- Ta: Non-invasive papillary carcinoma confined to the urothelium, above the basement membrane. The most common NMIBC presentation. Low-grade Ta has less than 5% progression risk; high-grade Ta carries a 15–30% progression risk.
- T1: Tumor invades the subepithelial connective tissue (lamina propria) but not the muscularis propria. T1 disease — particularly high-grade T1 — carries substantial progression risk (20–40%) and is the most clinically challenging NMIBC subgroup. Substaging into T1a (invasion into the inner half of the lamina propria, above the muscularis mucosae) and T1b (invasion into the outer lamina propria, below the muscularis mucosae) is prognostically significant but technically demanding.
- Tis (CIS): Flat, high-grade intraepithelial carcinoma. Clinically silent on cystoscopy (flat, red velvety patches) but detectable by cytology and random bladder biopsies. Carries 50–80% progression to invasive disease without treatment. Concurrent CIS with T1 disease substantially worsens prognosis.
- T2: Tumor invades the muscularis propria (detrusor muscle). T2a invades the inner half, T2b the outer half. This threshold defines MIBC, which requires more aggressive systemic and surgical management.
- T3: Tumor invades perivesical tissue. T3a is microscopically detected; T3b extends through the bladder wall as a macroscopic mass.
- T4: Tumor invades adjacent structures. T4a involves the prostate stroma, seminal vesicles, uterus, or vagina; T4b invades the pelvic wall or abdominal wall. Prognosis is markedly worse at T4b.
- N staging: N1 — single pelvic lymph node; N2 — multiple pelvic nodes or single obturator/iliac node; N3 — common iliac or para-aortic nodes.
- M staging: M0 = no distant metastasis; M1a = non-regional lymph nodes; M1b = other distant metastases (lung, liver, bone most common).
Initial Workup
Evaluation includes cystoscopy with biopsy/TURBT, upper tract imaging (CT urogram preferred), and urine cytology. Staging CT of the chest, abdomen, and pelvis is obtained for MIBC or high-risk NMIBC. Bone scan is reserved for patients with bone pain or elevated alkaline phosphatase. PET-CT is increasingly used for nodal and distant staging in MIBC candidates for curative therapy.
6. Diagnosis
Cystoscopy: Gold Standard
Cystoscopy is the definitive diagnostic procedure for bladder cancer. White-light cystoscopy identifies papillary or flat lesions of the bladder mucosa with high sensitivity for visible tumors. Blue-light cystoscopy (BLC) using the photosensitizer hexaminolevulinate (HAL, Cysview) exploits preferential accumulation of protoporphyrin IX in malignant urothelium, producing red fluorescence under violet light. BLC is superior to white-light cystoscopy for detecting flat CIS lesions (sensitivity increased by 20–30%) and is recommended for patients with high-grade disease, positive cytology without a visible lesion, or suspected CIS.
Transurethral Resection of Bladder Tumor (TURBT)
TURBT is both a diagnostic and therapeutic procedure — the initial management for all NMIBC. Adequate TURBT requires complete macroscopic resection with inclusion of detrusor muscle in the specimen for accurate T-staging. A re-TURBT at 4–6 weeks is recommended for all high-grade T1 tumors, large tumors, incomplete initial resection, or absence of muscle in the initial specimen. Re-TURBT upstages approximately 20–30% of T1 lesions and provides critical prognostic information. A single immediate post-operative intravesical instillation of mitomycin C or gemcitabine within 6 hours of TURBT reduces short-term recurrence risk by approximately 39% in low-risk NMIBC (SWOG S0337 data).
Urine Cytology
Voided urine cytology is a non-invasive adjunct with high specificity (greater than 95%) for high-grade urothelial carcinoma and CIS but poor sensitivity for low-grade tumors (approximately 20–40%). The Paris System for Reporting Urinary Cytology (TPS) standardizes cytology reporting into five categories (negative, atypical, suspicious, high-grade malignancy, low-grade malignancy). Positive cytology in the absence of a visible bladder lesion mandates upper tract evaluation and random bladder biopsies.
Urine Biomarkers
- NMP22 (Nuclear Matrix Protein 22): A point-of-care immunoassay detecting NMP22 released from apoptotic bladder cancer cells; FDA-approved as an adjunct to cytology. Sensitivity for high-grade tumors is approximately 65–70%, with superior performance over cytology for low-grade lesions, but high false-positive rates in patients with urinary tract infections, calculi, or catheters limit specificity.
- UroVysion FISH (fluorescence in situ hybridization): Detects chromosomal abnormalities (gains of chromosomes 3, 7, 17 and loss of 9p21/CDKN2A) characteristic of urothelial carcinoma. Sensitivity exceeds 90% for high-grade tumors; a positive FISH result in the setting of negative cystoscopy ("anticipatory positive") predicts recurrence and warrants intensified surveillance.
- Cxbladder, ADXBLADDER, and Bladder EpiCheck: Emerging molecular and epigenetic urine tests under evaluation as surveillance adjuncts; the EAU guidelines now incorporate some for surveillance risk stratification.
7. Treatment
NMIBC: Intravesical BCG Therapy
Intravesical bacillus Calmette-Guerin (BCG) immunotherapy, introduced by Morales et al. in 1976, remains the most effective adjuvant intravesical treatment for high-risk NMIBC. BCG is a live attenuated mycobacterium that, when instilled into the bladder after TURBT, induces a Th1-predominant local immune response characterized by IL-2, IL-12, TNF-alpha, and interferon-gamma secretion, destroying residual tumor cells and providing durable protection against recurrence and progression. Standard induction consists of weekly intravesical instillations for 6 weeks, followed by maintenance BCG at 3, 6, 12, 18, 24, 30, and 36 months (SWOG S8507 protocol). Three years of maintenance BCG is superior to 1 year for preventing progression in high-risk disease. Adverse effects include cystitis (most common), fever, and rarely disseminated BCG infection (BCGosis) requiring antitubercular therapy.
BCG is indicated for all CIS, high-grade T1 disease, and high-grade Ta disease. For high-grade T1 tumors with concurrent CIS, lymphovascular invasion, variant histology (micropapillary, plasmacytoid, sarcomatoid), or BCG failure, early radical cystectomy is recommended rather than repeated BCG courses, as the risk of metastatic progression outweighs bladder-preservation benefit.
BCG-Unresponsive NMIBC: Pembrolizumab KEYNOTE-057
For patients with BCG-unresponsive high-grade NMIBC (CIS with or without papillary tumors) who are ineligible for or refuse radical cystectomy, pembrolizumab (anti-PD-1) was evaluated in the single-arm KEYNOTE-057 cohort A trial. Complete response rate was 41% at 3 months, with 46% of complete responders maintaining response at 12 months. FDA approved pembrolizumab in January 2020 for this BCG-unresponsive CIS indication. Nadofaragene firadenovec (intravesical adenoviral-mediated interferon-alpha gene therapy, FDA-approved 2022) and nogapendekin alfa inbakicept (IL-15 superagonist) are additional options in this space.
MIBC: Neoadjuvant Chemotherapy and Radical Cystectomy
The standard of care for fit patients with MIBC (T2–T4a, N0–N1, M0) is cisplatin-based neoadjuvant chemotherapy (NAC) followed by radical cystectomy. The landmark SWOG 8710 trial demonstrated a median survival benefit of 14 months (77 months vs. 46 months) and an absolute 5-year overall survival benefit of 8% (57% vs. 43%) for NAC with MVAC (methotrexate, vinblastine, doxorubicin, cisplatin) plus cystectomy versus cystectomy alone. Gemcitabine-cisplatin (GC) has equivalent efficacy with superior tolerability and is preferred in contemporary practice. Pathologic complete response (pT0 at cystectomy) after NAC, achieved in 25–35% of patients, is a strong surrogate for improved survival. Dose-dense MVAC (ddMVAC) achieves higher pCR rates and is increasingly used. Patients with eGFR less than 50–60 mL/min/1.73m2 are cisplatin-ineligible; carboplatin-based regimens are inferior and should be reserved for the metastatic setting.
Radical cystectomy includes en-bloc removal of the bladder, perivesical fat, and regional lymph nodes; in men, the prostate, seminal vesicles, and proximal urethra; in women, the uterus, fallopian tubes, ovaries, anterior vaginal wall, and urethra (when involved). Extended pelvic lymph node dissection (eLND) improves staging accuracy and may provide survival benefit. Urinary diversion options include ileal conduit (most commonly performed), orthotopic neobladder (requiring intact urethral sphincter and patient motivation for self-catheterization), or Indiana pouch continent diversion.
Bladder-Sparing Trimodality Therapy (TMT)
For patients with solitary T2–T3 tumors, complete TURBT achievable, no hydronephrosis, and normal bladder function who desire to preserve the bladder, trimodality therapy (TMT) — maximal TURBT, concurrent chemoradiation (cisplatin or 5-FU/mitomycin C as radiosensitizer), and cystoscopic surveillance — provides 5-year overall survival of 50–65% in carefully selected patients, comparable to cystectomy series. The Radiation Therapy Oncology Group (RTOG) 89-03, 95-06, and 97-06 protocols established TMT as a legitimate curative alternative. Predictors of favorable TMT outcome include complete initial TURBT, cT2 disease, absence of hydronephrosis, and absence of CIS.
Metastatic Urothelial Carcinoma: Pembrolizumab + Enfortumab Vedotin
The first-line standard of care for metastatic urothelial carcinoma has been transformed by the EV-302 / KEYNOTE-869 trial, which randomized 886 patients to enfortumab vedotin (EV, anti-Nectin-4 antibody-drug conjugate) plus pembrolizumab versus platinum-based chemotherapy. EV+pembro achieved a median overall survival of 31.5 months versus 16.1 months for chemotherapy (HR 0.47), with a confirmed overall response rate of 67.7% versus 44.4%. This combination received FDA approval in December 2023 regardless of PD-L1 status, replacing platinum-based chemotherapy as the preferred first-line option for eligible patients.
For cisplatin-ineligible patients who receive first-line platinum-based therapy, avelumab maintenance (anti-PD-L1) — following disease control with platinum-based chemotherapy — demonstrated significantly improved overall survival over best supportive care in the JAVELIN Bladder 100 trial (21.4 months vs. 14.3 months, HR 0.69), establishing a new maintenance standard.
FGFR3-Targeted Therapy: Erdafitinib
Approximately 15–20% of metastatic urothelial carcinomas harbor activating FGFR3 or FGFR2 mutations or fusions. Erdafitinib, a pan-FGFR kinase inhibitor, received FDA approval in 2019 for FGFR-altered metastatic urothelial carcinoma progressing after platinum-based chemotherapy, based on an overall response rate of 32.2% and median duration of response of 5.4 months in the THOR trial's phase 2 cohort. FGFR3 mutational testing is now recommended for all metastatic urothelial carcinoma patients.
8. Complications
- Hydronephrosis: Ureteral obstruction by bladder tumor at the ureteral orifice or by perivesical extension causes hydroureteronephrosis, which is a poor prognostic indicator. Bladder cancer with hydroureteronephrosis on imaging carries T3b or higher staging in most cases and increases the risk of renal insufficiency that may render patients cisplatin-ineligible for NAC. Ureteral stenting or nephrostomy may be required before surgery.
- Tumor recurrence and progression: NMIBC recurrence affects 50–70% of patients within 5 years of initial TURBT; 10–30% progress to MIBC. Risk stratification using EORTC or CUETO risk tables guides surveillance cystoscopy frequency and adjuvant therapy intensity. Progression to MIBC markedly worsens prognosis and necessitates a shift to systemic therapy and radical surgery.
- Gross hematuria and hemorrhagic cystitis: Tumor-related hematuria can cause urinary clot retention, requiring bladder irrigation, clot evacuation, and occasionally arterial embolization or cystoscopic fulguration. Radiation-induced hemorrhagic cystitis is a delayed complication of pelvic radiation, sometimes presenting years after treatment.
- Urinary diversion complications: After radical cystectomy, ileal conduit and neobladder diversions are associated with metabolic acidosis (hyperchloremic), urinary tract infections, stomal stenosis or parastomal hernia (conduit), neobladder-urethral anastomotic stricture, urinary retention requiring self-catheterization (neobladder, in up to 25% of women), and vitamin B12 deficiency from ileal segment resection.
- Sexual dysfunction: Nerve-sparing cystectomy techniques reduce erectile dysfunction risk in men but standard radical cystectomy causes erectile dysfunction in the majority. Women undergoing anterior exenteration lose the anterior vaginal wall and may have significantly altered sexual function; vaginal reconstruction or neovaginal techniques can partially mitigate this.
- BCG complications: Systemic BCG infection (BCGosis) manifests as fever, hypotension, and multi-organ involvement and requires antitubercular therapy with isoniazid, rifampin, and ethambutol. BCG sepsis is rare (approximately 0.4% of patients) but life-threatening. Intravesical BCG should not be instilled within 2 weeks of TURBT or in the presence of traumatic catheterization to reduce the risk of systemic absorption.
- Immunotherapy-related adverse events: Pembrolizumab and other checkpoint inhibitors cause immune-related adverse events (irAEs) including pneumonitis, colitis, hepatitis, endocrinopathies (thyroiditis, adrenal insufficiency, diabetes), and nephritis. Severe (grade 3–4) irAEs require high-dose corticosteroids and treatment discontinuation in approximately 5–10% of patients.
9. Prognosis
Prognosis varies dramatically by stage at diagnosis. For NMIBC, the 5-year overall survival exceeds 95% for low-grade Ta disease treated with TURBT alone or with adjuvant intravesical chemotherapy. High-grade T1 disease with CIS, variant histology, or BCG failure carries a 5-year disease-specific survival of 70–80% with aggressive management including early cystectomy in appropriate candidates; outcomes are substantially worse if progression to MIBC occurs before cystectomy. EORTC risk table scores stratify low-risk (annual recurrence rate 15%, 5-year progression less than 1%) to high-risk (recurrence rate 61%, progression rate 17%) NMIBC.
For MIBC, 5-year overall survival decreases with advancing stage: approximately 60–65% for pT2N0, 40–50% for pT3N0, 20–30% for pT4N0, and less than 20% for node-positive (pN+) disease even after definitive therapy. Pathologic complete response (pT0) after NAC is associated with 5-year overall survival exceeding 80%. For metastatic urothelial carcinoma, the EV+pembrolizumab combination has extended median overall survival to 31.5 months from a historical median of 14–16 months with platinum-based chemotherapy alone, representing the most significant survival improvement in this disease in decades. Long-term survivors (greater than 5 years) with metastatic disease are increasingly observed with modern immunotherapy combinations.
10. Prevention
- Smoking cessation: The single most impactful preventive intervention. Risk reduction begins within 1–2 years of cessation and approaches background risk at approximately 15 years of abstinence. All patients with bladder cancer who smoke should receive intensive cessation counseling, pharmacotherapy (varenicline, nicotine replacement therapy, or bupropion), and referral to behavioral cessation programs.
- Occupational exposure reduction: Engineering controls, personal protective equipment, and regulatory exposure limits for aromatic amines in dye, rubber, leather, and hairdressing industries. Bladder cancer screening by urine cytology is offered to high-risk occupational cohorts in some European countries. Substitution of benzidine-based dyes with less carcinogenic alternatives has reduced occupational bladder cancer in industrialized nations.
- Schistosomiasis prevention and treatment: In endemic regions, mass drug administration with praziquantel reduces schistosomal bladder disease and associated SCC risk. Improved sanitation, molluscicide treatment of water bodies, and avoidance of freshwater exposure in endemic areas reduces transmission.
- Fluid intake: Higher fluid intake (greater than 2 liters per day) may dilute urinary carcinogens and reduce urothelial contact time; epidemiological data are suggestive but not definitive. Adequate hydration is a low-risk recommendation for high-risk individuals.
- Avoidance of aristolochic acid herbal products: Patients should be counseled against herbal preparations containing Aristolochia species, which are found in some traditional Chinese, Balkan, and South American herbal medicines. Regulatory bans in many countries have reduced exposure, but unregistered products remain available.
- Genetic counseling for Lynch syndrome: Individuals from HNPCC families or with personal history of early-onset urothelial carcinoma should undergo mismatch repair gene testing. Lynch syndrome carriers benefit from intensified urothelial surveillance (urine cytology every 1–2 years from age 30–35) given elevated urothelial tract cancer risk.
11. Recent Research
EV-302 / KEYNOTE-869 (Enfortumab Vedotin + Pembrolizumab, 1L Metastatic): The phase 3 EV-302 trial enrolled 886 previously untreated metastatic urothelial carcinoma patients and demonstrated that enfortumab vedotin (EV) plus pembrolizumab nearly doubled overall survival compared to gemcitabine-platinum chemotherapy (median OS 31.5 vs. 16.1 months, HR 0.47, p<0.001). Progression-free survival was also significantly improved (12.5 vs. 6.3 months). The EV+pembro combination received FDA approval in December 2023, establishing the first new first-line standard in over 30 years for this disease. EV targets Nectin-4, a cell adhesion molecule overexpressed on urothelial carcinoma cells, delivering the microtubule-disrupting payload MMAE (monomethyl auristatin E) with high selectivity.
KEYNOTE-052 (Pembrolizumab, 1L Cisplatin-Ineligible): In KEYNOTE-052, pembrolizumab monotherapy achieved an objective response rate of 29% (complete response 7%) in 370 cisplatin-ineligible patients with locally advanced/metastatic urothelial carcinoma, with responses durable at a median of 30 months in complete responders. PD-L1 combined positive score (CPS) greater than or equal to 10 predicted higher response rates. Pembrolizumab is FDA-approved for this platinum-ineligible indication and remains a standard option for patients who cannot receive EV+pembro.
JAVELIN Bladder 100 (Avelumab Maintenance): The JAVELIN Bladder 100 trial randomized 700 patients with metastatic urothelial carcinoma who had not progressed on first-line platinum-based chemotherapy to avelumab (anti-PD-L1) maintenance plus best supportive care versus best supportive care alone. Avelumab maintenance significantly extended median overall survival (21.4 vs. 14.3 months, HR 0.69, p=0.0008) and progression-free survival, establishing avelumab as the standard maintenance approach after platinum-based induction in patients without disease progression.
Perioperative Nivolumab (CheckMate 274, NIAGARA): Adjuvant nivolumab (anti-PD-1) improved disease-free survival after radical cystectomy in high-risk MIBC patients (CheckMate 274; HR 0.70 for DFS in the all-randomized population, with greater benefit in PD-L1-high tumors). The NIAGARA trial is evaluating perioperative durvalumab (neoadjuvant + adjuvant) combined with chemotherapy, with preliminary results suggesting benefit. These data are reshaping the perioperative treatment landscape for resectable MIBC.
FGFR3-Targeted Therapy (Erdafitinib, THOR): The phase 3 THOR trial confirmed erdafitinib superiority over pembrolizumab or chemotherapy (physician's choice) in FGFR-altered metastatic urothelial carcinoma previously treated with immunotherapy. Erdafitinib achieved an overall response rate of 45.6% versus 11.9% for the comparator arm. The trial underscores the importance of routine FGFR3 molecular testing in metastatic urothelial carcinoma to identify patients most likely to benefit from targeted therapy.
12. References
- Search PubMed — Intracavitary bacillus Calmette-Guerin in the treatment of superficial bladder tumors. J Urol. 1976;116(2):180-183.
- Search PubMed — Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer (SWOG 8710). N Engl J Med. 2003;349(9):859-866.
- Search PubMed — First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052). Lancet Oncol. 2017;18(11):1483-1492.
- Search PubMed — Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma (JAVELIN Bladder 100). N Engl J Med. 2020;383(13):1218-1230.
- Search PubMed — Treatment of non-metastatic muscle-invasive bladder cancer: AUA/ASCO/ASTRO/SUO guideline. J Urol. 2017;198(3):552-559.
- Search PubMed — Predicting recurrence and progression in individual patients with stage TaT1 bladder cancer using EORTC risk tables. Eur Urol. 2006;49(3):466-477.
- Search PubMed — A re-staging transurethral resection predicts early progression of superficial bladder cancer. BJU Int. 1999;84(9):1055-1060.
- Search PubMed — Treatment of muscle-invasive and metastatic bladder cancer: update of the EAU guidelines. Actas Urol Esp. 2012;36(8):449-460.
- Search PubMed — Bladder cancer. Lancet. 2009;374(9685):239-249.
- Search PubMed — Enfortumab vedotin in previously treated advanced urothelial carcinoma. N Engl J Med. 2021;384(12):1125-1135.
- Johansson SL, Cohen SM, 1997 — PMID: 32877583 — Epidemiology and etiology of bladder cancer. Semin Surg Oncol. 1997;13(5):291-298.
- Search PubMed — EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder (TaT1 and CIS). Eur Urol. 2017;71(3):447-461.
Connections
- Urology
- Kidney Stones
- Renal Cell Carcinoma
- Testicular Cancer
- Prostate Conditions
- Urinary Tract Infections
- Overactive Bladder
- Interstitial Cystitis
- Chemotherapy
- Immunotherapy
- Tobacco Smoke
- Urinalysis
- Parasites Overview