Takayasu Arteritis
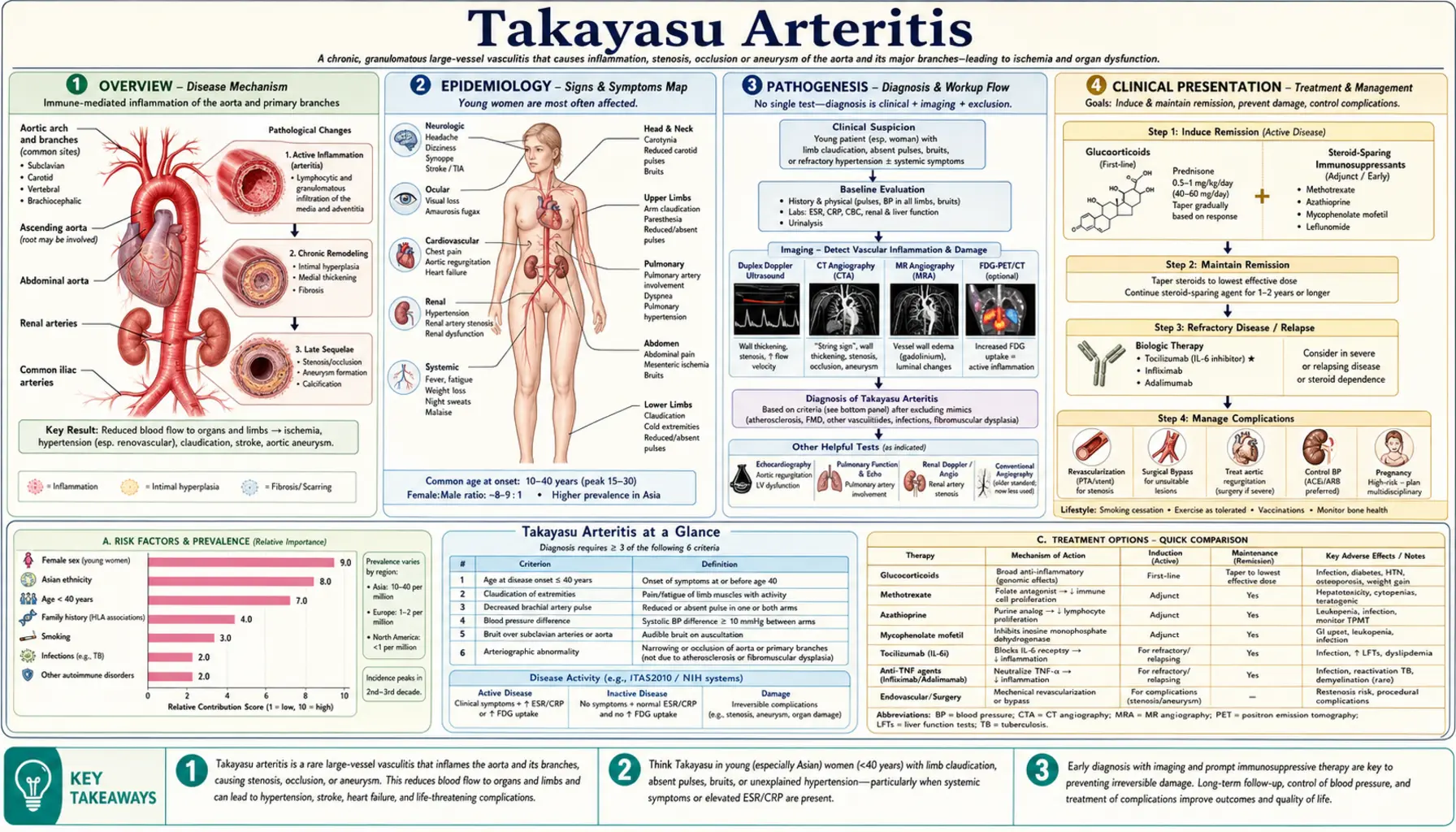
Table of Contents
- Overview
- Epidemiology
- Pathogenesis
- Clinical Presentation
- Classification
- Diagnosis
- Monitoring Disease Activity
- Treatment
- Living with Takayasu Arteritis
- Prognosis
- Research Papers
- Connections
- Featured Videos
1. Overview
Takayasu Arteritis (TA) is a rare, chronic, granulomatous vasculitis that targets the aorta — the body's largest artery — and its major branches, including the subclavian, carotid, vertebral, renal, and mesenteric arteries, as well as the pulmonary arteries. Inflammation progressively thickens, narrows, or blocks these critical vessels, cutting off blood supply to the arms, brain, kidneys, gut, and other organs. Alternatively, chronic inflammation can weaken vessel walls and cause them to balloon outward, forming aneurysms.
Because subclavian artery stenosis can eliminate detectable pulses in both arms, Takayasu Arteritis has long been called "pulseless disease" — a striking physical finding that was historically how the condition was first recognized. The name honors Mikito Takayasu, a Japanese ophthalmologist who in 1908 described unusual wreath-like anastomotic rings of blood vessels surrounding the optic disc in a young woman's retina — changes now understood to represent collateral circulation forming in response to occlusion of the aortic arch vessels supplying the eye and brain. His case report, published in the Acta Societatis Ophthalmologicae Japonicae, launched more than a century of investigation into this fascinating and complex disease.
TA is classified as a large-vessel vasculitis alongside Giant Cell Arteritis (GCA), but the two diseases differ sharply in who they affect: GCA strikes older adults (typically over 50), while Takayasu Arteritis predominantly targets young women in the prime of their reproductive years. This distinction has profound implications — a young woman presenting with arm claudication, absent radial pulse, or unexplained hypertension deserves prompt investigation for TA.
TA is rare in Western countries, affecting roughly 1–2 people per million per year in Europe and North America. However, the disease is substantially more common across East, Southeast, and South Asia, as well as parts of Latin America, where it represents a meaningful cause of renovascular hypertension and stroke in young people. Worldwide, the disease disproportionately affects women, with a female-to-male ratio of approximately 8–9 to 1.
Without treatment, TA steadily destroys blood vessels over years and decades, leading to stroke, heart failure from aortic valve damage, renal failure from kidney artery stenosis, and blindness. With modern immunosuppressive therapy and timely vascular surgery or intervention, most patients live decades with their disease — but the road requires vigilance, patience, and a strong partnership between patient and specialist team.
2. Epidemiology
Takayasu Arteritis predominantly affects young women, with a peak age of onset between 15 and 40 years. The female-to-male ratio is striking at approximately 8–9:1 — far higher than most autoimmune diseases. Why women in this age group are so disproportionately affected is not fully understood, but sex hormones almost certainly play a modulatory role in the immune dysregulation that drives the disease.
Geographic Distribution
TA is a disease with a clear geographic gradient. Incidence and prevalence are highest in:
- Japan: Approximately 150 new cases per year nationally — the country where the disease was first described and remains most studied. Incidence roughly 1–2/million/year.
- India: Incidence estimates of 6–10/million/year make India one of the highest-burden countries globally. TA is an important cause of renovascular hypertension and aortic aneurysm in young Indian women.
- China and Korea: TA is a recognized major cause of large-vessel disease in young adults across both countries.
- Mexico and Latin America: Higher incidence than Europe or North America, with TA frequently presenting in young women with hypertension or stroke.
- North America and Europe: Estimated incidence of 1–2.6/million/year. Less common but not rare; often delayed in diagnosis because clinicians may not consider it in young Western women.
Genetic Risk Factors
The HLA-B52 antigen — and specifically the HLA-B*5201 subtype — is the most consistently replicated genetic risk factor for TA across all studied populations, including Japanese, Korean, Indian, Turkish, and North American cohorts. Carriers of HLA-B52 have approximately three times the risk of developing TA compared to non-carriers. The specific HLA subtype also appears to subtly influence disease phenotype and severity. Outside of HLA, genome-wide association studies have identified additional risk loci involving immune regulation (including IL12B, RPS9/LILRB3, and the MLX gene region), but none approach the effect size of HLA-B52.
The geographic clustering of TA in Asian and Latin American populations mirrors — at least in part — the geographic distribution of HLA-B52, which is more prevalent in these populations. However, environmental and infectious triggers that interact with genetic susceptibility almost certainly also contribute to the global distribution pattern.
Age at Diagnosis
Although peak onset is 15–40 years, TA can first manifest in childhood (pediatric TA) or, rarely, in older adults. Children with TA often present with hypertension and renal artery stenosis. Delay in diagnosis from symptom onset to confirmed TA is typically 1–3 years — a critical window during which ongoing inflammation silently injures vessels before the disease is identified.
3. Pathogenesis
The exact cause of Takayasu Arteritis — what triggers the immune system to attack the aorta and its branches — remains unknown. The best current evidence points to an antigen-driven, T cell-mediated granulomatous inflammation that progresses through all three layers of the arterial wall (pan-arteritis), eventually scarring and remodeling the vessel into either a tight stenosis or a weakened aneurysm.
Cellular Mechanisms
The inflammatory infiltrate in TA consists primarily of:
- CD4+ T lymphocytes (T helper cells): The dominant cell type in the granulomas. These cells secrete interferon-gamma (IFN-γ), interleukin-6 (IL-6), interleukin-17 (IL-17), and tumor necrosis factor-alpha (TNF-α), all of which sustain and amplify vessel wall inflammation.
- CD8+ cytotoxic T lymphocytes: Directly kill vascular smooth muscle cells and endothelial cells, contributing to tissue destruction in the medial layer.
- Macrophages and multinucleated giant cells: Fuse to form the granulomas that are the histological hallmark of the disease — clusters of activated macrophages surrounded by lymphocytes, sometimes with Langerhans-type giant cells.
- γδ T cells and natural killer (NK) cells: Implicated in the initial wave of vascular injury, possibly responding to heat shock proteins expressed on stressed vascular cells.
- Dendritic cells: Act as sentinels in the adventitia (outer layer), presenting an as-yet-unidentified antigen to T cells and initiating the adaptive immune cascade.
Cytokine Storm and Structural Consequences
Once T cells are activated, the resulting cytokine milieu drives a self-sustaining inflammatory loop. IL-6 — produced abundantly by macrophages and T cells in the vessel wall — is particularly central; it drives acute-phase protein production (explaining elevated ESR and CRP), promotes T cell differentiation, and directly stimulates vascular smooth muscle cell proliferation. This proliferation, combined with intimal thickening from myofibroblast activation, progressively narrows the arterial lumen.
The structural outcomes depend on which layer is most severely damaged:
- Stenosis and occlusion (75–80% of lesions): Intimal hyperplasia + medial fibrosis + adventitial scarring → concentric luminal narrowing → eventual total occlusion, forcing the body to develop collateral vessels (the "anastomotic wreaths" Takayasu observed in the retina).
- Aneurysm formation (20–25% of lesions): Destruction of the elastic fibers in the medial layer weakens the wall → pressure-driven dilation → saccular or fusiform aneurysm → risk of rupture or thrombosis.
The Role of HLA-B52
HLA-B52 is a class I HLA molecule that presents peptide antigens to CD8+ cytotoxic T cells. Its strong association with TA suggests that cytotoxic T cell-mediated killing of vessel wall cells — triggered by a specific (unknown) antigen presented by HLA-B52 — is a key initiating event. Carriers of HLA-B*5201 may have a subtly different disease pattern, though this is still being characterized across populations.
Unresolved Questions
The central mystery of TA remains: what antigen sets off the immune attack on the aorta? Candidates include heat shock proteins (HSP60, HSP65) expressed on vascular cells under stress, an unknown microbial antigen that cross-reacts with vessel wall proteins (molecular mimicry), or an endogenous vascular antigen presented de novo by HLA-B52. Identifying this antigen would be transformative for both diagnosis and targeted therapy.
4. Clinical Presentation
Takayasu Arteritis classically unfolds in two phases, though in practice the boundary between them is blurry and both phases can overlap. Understanding this two-phase model helps explain why TA is so often diagnosed late: the first phase looks like dozens of other conditions, and the dramatic physical findings of the second phase only emerge after years of smoldering vascular damage.
Phase 1: The Inflammatory (Pre-Pulseless) Phase
Early TA produces nonspecific systemic symptoms that are easily mistaken for viral illness, tuberculosis, or other inflammatory conditions:
- Fever and night sweats: Often low-grade but persistent; can be the presenting complaint for months.
- Fatigue and malaise: Profound and out of proportion to other findings; interferes significantly with daily function.
- Weight loss: Unintentional, often 5–10% of body weight over weeks to months.
- Arthralgias and myalgias: Joint and muscle aches, often migratory; can be misdiagnosed as early rheumatoid arthritis or lupus.
- Carotidynia: Tenderness and pain directly over the carotid arteries in the neck, caused by inflammation of the carotid artery wall. When present, this finding is highly suggestive of TA — almost no other common condition causes direct carotid tenderness in a young woman.
- Elevated inflammatory markers: ESR and CRP are typically elevated during the active inflammatory phase, though they can normalize even when disease is still active (a major diagnostic challenge).
Phase 2: The Occlusive (Pulseless) Phase
As arterial stenoses develop and progress, ischemic symptoms emerge. The specific symptoms depend on which arteries are most severely affected:
Upper Limb Involvement (Subclavian Artery Stenosis)
- Upper limb claudication: Fatigue, aching, or weakness in the arms during use (writing, lifting, reaching overhead). The arm equivalent of leg claudication from peripheral artery disease.
- Absent or diminished arm pulses: The radial and/or brachial pulses cannot be felt — the finding that gave TA its "pulseless disease" name. May be unilateral or bilateral.
- Blood pressure discrepancy between arms >10 mmHg: When subclavian stenosis is unilateral or asymmetric, standard blood pressure measurement in the lower-pressure arm gives a falsely low reading, potentially missing hypertension or masking shock. BP should always be measured in both arms in suspected TA.
- Carotid and subclavian bruits: Turbulent blood flow through narrowed vessels creates audible bruits on auscultation over the neck and supraclavicular fossae.
Cerebrovascular Involvement (Carotid/Vertebral Artery Stenosis)
- Visual disturbances: Transient monocular blindness (amaurosis fugax), double vision (diplopia), or blurred vision from reduced blood flow to the optic nerve and retina. The retinal anastomotic wreaths Takayasu observed in 1908 were the collateral response to this ischemia.
- Stroke and TIA: Carotid or vertebral artery stenosis or occlusion can cause ischemic stroke or transient ischemic attacks in young patients — a presentation that should always prompt investigation for TA in a young woman.
- Dizziness, syncope, and drop attacks: From vertebrobasilar insufficiency due to vertebral artery stenosis.
- Headache and cognitive symptoms: Chronic reduction in cerebral perfusion.
Cardiovascular Involvement (Aortic Root / Coronary Arteries)
- Aortic regurgitation: Inflammation of the aortic root dilates the aortic annulus and damages the aortic valve leaflets, causing incompetence in 20–25% of patients. Presents with the classic findings of AR: wide pulse pressure, bounding pulse, and diastolic murmur. Progressive AR can cause heart failure.
- Coronary artery involvement: Rare (5–10%), but causes angina or myocardial infarction in young patients who have no conventional cardiovascular risk factors — a diagnostic red flag for TA.
- Cardiomyopathy: From chronic hypertension (renovascular), aortic regurgitation, or myocarditis associated with TA.
Renal Involvement (Renal Artery Stenosis)
- Renovascular hypertension: The most common presenting feature in many series from India and Latin America. Renal artery stenosis reduces renal perfusion, activating the renin-angiotensin system and causing severe, often treatment-resistant hypertension. In any young woman with difficult-to-control hypertension, TA must be excluded.
- Renal impairment: Chronic renal ischemia can lead to renal atrophy and declining kidney function over time.
Abdominal and Pulmonary Involvement
- Mesenteric ischemia: Abdominal pain after eating (intestinal angina) from stenosis of the superior mesenteric or celiac arteries. Severe cases can cause bowel ischemia.
- Pulmonary artery involvement: Present in approximately 50% of patients on advanced imaging, though often clinically silent. Can cause pulmonary hypertension, dyspnea on exertion, chest pain, and hemoptysis in more severe cases.
5. Classification (Numano System)
The Numano classification system, developed by Japanese cardiologist Fujio Numano, categorizes TA based on which arterial territories are involved. This classification has practical importance because different types carry different patterns of complication and may influence surgical planning.
- Type I: Involves only the aortic arch branches (brachiocephalic, carotid, subclavian arteries). Presents primarily with upper limb and cerebrovascular ischemic symptoms.
- Type IIa: Involves the ascending aorta, aortic arch, and its branches. Adds aortic root disease (risk of aortic regurgitation) to Type I territory.
- Type IIb: Extends to include the descending thoracic aorta in addition to the ascending aorta, arch, and branches.
- Type III: Involves the descending thoracic aorta, abdominal aorta, and renal arteries. This pattern is associated with renovascular hypertension and carries significant risk of renal failure.
- Type IV: Confined to the abdominal aorta and its branches (renal, mesenteric). Often presents as renovascular hypertension or mesenteric ischemia without upper limb findings.
- Type V: A combined pattern equivalent to Types IIb + IV, involving the entire aorta from ascending to abdominal and all its major branches. Type V is the most common pattern overall, accounting for >60% of cases in large series.
Two important modifiers are added as suffixes:
- "P" suffix: Indicates pulmonary artery involvement (e.g., Type V+P). Present in approximately 50% of patients on sensitive imaging.
- Coronary artery involvement: Noted separately, occurring in 5–10% of patients. Causes angina, MI, or sudden death in young adults without conventional risk factors.
Understanding the distribution of disease is critical for surgical planning: a patient with Type I disease who needs carotid or subclavian revascularization has a very different operative approach than a patient with Type III disease requiring renal artery bypass.
6. Diagnosis
Diagnosing TA requires combining clinical findings, laboratory results, and vascular imaging. No single test is definitive. The 2022 ACR/EULAR classification criteria — developed to standardize research enrollment — are increasingly used as a practical clinical guide, replacing the older 1990 ACR criteria.
2022 ACR/EULAR Classification Criteria
Grayson et al. (2022) require age at diagnosis ≤60 years plus at least 3 of the following features:
- Limb claudication (upper or lower limb fatigue/pain with use)
- Decreased or absent brachial artery pulse
- Blood pressure differential >10 mmHg between arms
- Carotid bruit on auscultation
- Angiographic evidence of stenosis, occlusion, or aneurysm of the aorta or its major branches (not attributable to arteriosclerosis or fibromuscular dysplasia)
The older 1990 ACR criteria used age ≤40 as the cutoff — a threshold now recognized as too restrictive, since late-onset TA does occur. The 2022 update raises this to ≤60 years.
Vascular Imaging
Imaging is the cornerstone of diagnosis and follow-up. Options include:
- CT Angiography (CTA): Provides excellent anatomical detail of the aorta and its branches. Active TA shows characteristic mural thickening and mural edema ("double ring" enhancement on contrast CT) in addition to luminal changes. CTA gives the best spatial resolution and is the most widely used modality for initial mapping of disease extent. Limitation: radiation exposure makes it less ideal for long-term serial monitoring in young women.
- MR Angiography (MRA): No ionizing radiation — preferred for serial monitoring in young patients. MRI with gadolinium can demonstrate mural thickening and edema (evidence of active inflammation) as well as luminal stenosis and aneurysm. Slightly lower spatial resolution than CTA for fine branch vessels.
- FDG-PET / PET-CT: Fluorodeoxyglucose (FDG) is taken up by metabolically active inflammatory cells. PET shows increased FDG uptake in the aortic wall and branches in active TA — making it the most sensitive imaging tool for detecting metabolic disease activity. FDG-PET/CT combines functional (inflammation) and anatomical (stenosis/aneurysm) data. Particularly useful when clinical symptoms and lab markers are discordant with suspected disease activity, and for monitoring treatment response. Limitation: high cost; radiation from CT component.
- Digital Subtraction Angiography (DSA): The historical gold standard for defining luminal anatomy. Still used when endovascular intervention is planned and when CTA/MRA findings are equivocal. Limitation: invasive; misses mural inflammation (shows only the lumen); radiation and contrast required.
- Vascular Ultrasound: Non-invasive and radiation-free. The "macaroni sign" — uniform circumferential hypoechoic thickening of the carotid or subclavian artery wall — is a characteristic ultrasound finding in active TA. Useful for serial monitoring of carotid and subclavian arteries, but limited by operator dependence and inability to image the thoracic aorta.
Laboratory Investigations
- ESR and CRP: Elevated in active disease but frustratingly unreliable. Approximately 50% of patients with angiographically active TA have normal ESR and CRP — a normal value does NOT exclude active disease. Conversely, elevated values support activity and can be used to track treatment response.
- Interleukin-6 (IL-6): More sensitive than ESR/CRP for disease activity in some studies; useful in patients on tocilizumab (which suppresses downstream acute-phase proteins).
- Complete blood count: May show anemia of chronic disease, leukocytosis, and thrombocytosis in active disease.
- ANA, ANCA, anti-dsDNA: Typically negative; ordered to exclude overlapping connective tissue disease or ANCA vasculitis in the differential diagnosis.
Differential Diagnosis
Key conditions to exclude include: atherosclerosis (older patients, risk factors), fibromuscular dysplasia (younger women, bead-on-string angiographic pattern, no mural inflammation), Giant Cell Arteritis (age >50, temporal artery involvement, PMR), IgG4-related aortitis, infectious aortitis (syphilis, tuberculosis — especially in TB-endemic regions), and congenital aortic coarctation.
7. Monitoring Disease Activity
One of the most challenging aspects of managing Takayasu Arteritis is that no single reliable biomarker accurately reflects disease activity. A patient can feel fine, have normal ESR and CRP, yet have ongoing arterial inflammation visible on FDG-PET — or conversely, have elevated inflammatory markers from causes unrelated to TA. This diagnostic uncertainty makes steroid tapering particularly fraught: taper too fast and you risk relapse; stay on high-dose steroids indefinitely and you accumulate serious side effects.
NIH Criteria for Active Disease
The National Institutes of Health (NIH) criteria define active disease as the presence of any of the following:
- New or worsening systemic features: fever, arthralgia, weight loss, night sweats
- Elevated ESR or CRP (with or without systemic symptoms)
- New vascular signs or symptoms: new bruit, asymmetric pulses, new claudication, new hypertension
- Angiographic progression: new stenosis, occlusion, dilation, or aneurysm on serial imaging
Clinical Scoring Systems
- Indian Takayasu Activity Score (ITAS): Validated scoring tool for TA specifically, capturing vascular and constitutional domains. ITAS2010 is the most widely used version; scores ≥2 generally indicate active disease.
- Birmingham Vasculitis Activity Score (BVAS): Broader vasculitis activity score not specific to TA but widely used in clinical trials and specialist centers.
FDG-PET for Activity Monitoring
PET-CT has become an increasingly important tool for monitoring TA activity in specialized centers. FDG uptake in the aortic wall and branches — graded against liver background activity — correlates with histological inflammation and predicts relapse better than ESR/CRP alone. However, PET has practical limitations (cost, radiation, availability) that prevent its use as a routine monitoring tool for every clinic visit. It is most valuable when there is a clinical question about activity that cannot be resolved by symptoms and standard blood tests alone.
The Relapse Challenge
Relapse is the rule, not the exception, in TA. Studies consistently show that 50–80% of patients relapse during or after steroid tapering. This high relapse rate is the primary reason that steroid-sparing agents are added early and why many patients remain on low-dose immunosuppression indefinitely. Recognizing early relapse — before new arterial damage has occurred — requires careful coordination of clinical examination, labs, and interval imaging.
8. Treatment
Treatment of Takayasu Arteritis has two goals: controlling active inflammation to prevent new vascular damage, and managing existing stenoses or aneurysms through vascular intervention when necessary. Neither goal can be achieved in isolation — revascularization performed during active inflammation has much higher failure rates, while waiting indefinitely for perfect disease control may allow progressive ischemic organ damage.
Corticosteroids — First-Line Induction
High-dose corticosteroids (prednisone 0.5–1 mg/kg/day, commonly starting at 40–60 mg/day) remain the foundation of induction therapy. Corticosteroids effectively suppress the acute inflammatory response, normalizing ESR/CRP and improving systemic symptoms in the majority of patients within weeks. However:
- Only 50–70% of patients achieve initial remission on steroids alone.
- Relapse on taper is extremely common (50–80%), making steroid monotherapy inadequate for most patients long-term.
- Prolonged high-dose steroid use causes substantial harm: osteoporosis, diabetes, weight gain, cataracts, avascular necrosis of bone, and adrenal suppression. Bisphosphonate prophylaxis and calcium/vitamin D supplementation should be prescribed from the outset.
Standard practice is to taper steroids over 6–12 months while adding a steroid-sparing agent, targeting the lowest dose that maintains remission (ideally ≤5–7.5 mg/day).
Conventional Steroid-Sparing Immunosuppressants
- Methotrexate (MTX): The most evidence-supported conventional steroid-sparing agent for TA. Weekly oral or subcutaneous MTX (15–25 mg/week with folic acid supplementation) allows steroid tapering and reduces relapse rate. Landmark data from Hoffman et al. (1994) established its role in refractory disease.
- Azathioprine: Widely used, particularly in resource-limited settings; evidence base somewhat weaker than MTX for TA specifically but broadly effective in large-vessel vasculitis.
- Mycophenolate mofetil (MMF): Increasingly used, particularly in patients intolerant of MTX or azathioprine; growing evidence base in TA.
- Leflunomide: An alternative for MTX-intolerant patients; limited but positive data in refractory TA.
Biologic Therapies
Biologics have transformed the management of refractory TA over the past two decades:
- Tocilizumab (anti-IL-6 receptor): Targets the IL-6 pathway that is central to TA inflammation. The TAKT randomized controlled trial (Nakaoka et al., Ann Rheum Dis 2018) demonstrated a trend toward reduced relapse with tocilizumab versus placebo in a Japanese cohort, and multiple observational studies support its efficacy in refractory TA. Tocilizumab suppresses CRP so completely (to undetectable levels) that CRP can no longer be used to monitor disease activity in patients receiving it — FDG-PET or IL-6 levels must be used instead. Approved for Giant Cell Arteritis by the FDA; used off-label for TA (approved for TA in Japan).
- TNF inhibitors (infliximab, adalimumab, etanercept): Effective in refractory TA; infliximab has the most published evidence. Used when tocilizumab fails or is unavailable. Anti-TNF therapy requires TB screening and careful monitoring for infections.
- Abatacept: A CTLA-4-Ig fusion protein that modulates T cell co-stimulation; early evidence of efficacy in refractory TA from the MYCYC trial data and small series.
- Ustekinumab (anti-IL-12/23): Under investigation; rationale based on IL-17/Th17 pathway involvement in TA pathogenesis.
Vascular Intervention and Surgery
Revascularization is indicated for critical stenoses causing organ-threatening ischemia: limb-threatening claudication, severe renovascular hypertension refractory to medications, cerebrovascular compromise from carotid/vertebral stenosis, critical mesenteric ischemia, or severe aortic regurgitation. Key principles:
- Bypass surgery is preferred over percutaneous angioplasty (PTA): Long-term patency of bypass grafts is significantly better. Autologous vein or PTFE grafts from unaffected segments of aorta are preferred anchor sites. PTA ± stenting has higher restenosis rates (50–70% at 5 years in some series) and is reserved for selected, discrete lesions in accessible locations.
- Operate in remission when possible: Active vascular inflammation dramatically increases graft failure rates, anastomotic complications, and early restenosis. The standard recommendation is to delay elective revascularization until at least 3–6 months of immunosuppressive remission has been achieved. Emergency revascularization (for stroke, acute limb ischemia) may have to proceed regardless of disease activity.
- Aortic valve surgery or aortic root replacement: Required for severe progressive aortic regurgitation with cardiac failure; high surgical risk in this population due to the extent of aortic involvement.
Antithrombotic and Cardiovascular Medications
Low-dose aspirin is often prescribed to reduce thrombotic risk in stenotic or aneurysmal vessels. Aggressive management of cardiovascular risk factors (hypertension, dyslipidemia) is essential, particularly in patients with renovascular disease. ACE inhibitors and ARBs are cornerstone therapies for renovascular hypertension but must be used carefully in patients with bilateral renal artery stenosis.
9. Living with Takayasu Arteritis
Takayasu Arteritis is overwhelmingly a disease of young women — often diagnosed during college, early career, or the years of family building. The psychological, physical, and social dimensions of managing a chronic relapsing disease at this life stage deserve as much attention as the medical management.
The Psychological Toll
Living with TA means living with uncertainty. Will the steroids work this time? Will the next imaging scan show new damage? Can I safely get pregnant? Will I need surgery? Depression and anxiety are significantly more common in patients with TA than in the general population — a reality that is underrecognized and undertreated in rheumatology practice. Connecting with other patients through organizations like the Vasculitis Foundation or TA-specific patient communities can reduce isolation and provide practical guidance that no clinic appointment can offer.
Blood Pressure Monitoring at Home
Standard arm blood pressure cuffs may give falsely low or unmeasurable readings if both subclavian arteries are severely stenosed. Patients with bilateral subclavian involvement may need:
- Leg blood pressure measurement (using an ankle cuff and Doppler probe) as a proxy for central arterial pressure.
- Ambulatory blood pressure monitoring or central aortic pressure measurement in specialized centers.
- Education about which arm (if either) gives a reliable pressure reading, and consistent use of that arm for home monitoring.
Physical Activity and Exercise
During active inflammatory phases, high-intensity upper limb exercise should be avoided — it increases demand on already-compromised subclavian and brachial circulations and can precipitate ischemic symptoms. During remission, gentle to moderate aerobic exercise (walking, swimming with arms held low, cycling) is encouraged for cardiovascular health and to counteract the metabolic effects of long-term steroid therapy. A physiotherapist experienced in vascular or inflammatory conditions can design a safe exercise program tailored to which vessels are involved.
Pregnancy and Fertility
Many women with TA want to become pregnant, and this is achievable — but requires careful preconception planning and high-risk obstetric co-management. Key considerations:
- TA can worsen during pregnancy, particularly in the first trimester and postpartum period. The reason may relate to hormonal and immunological shifts of pregnancy.
- Uncontrolled renovascular hypertension is the most dangerous complication during pregnancy, increasing risk of preeclampsia, placental insufficiency, and fetal growth restriction.
- Medications require review: Methotrexate is absolutely contraindicated in pregnancy (teratogenic). Azathioprine and low-dose steroids are generally considered relatively safe during pregnancy. Tocilizumab and TNF inhibitors are used with caution; data are limited but growing.
- Mode of delivery: Regional anesthesia may be complicated by subclavian stenosis affecting monitoring; general anesthesia carries risks from aortic involvement. Delivery planning should involve the rheumatologist, obstetrician, and anesthetist.
- Many women with well-controlled TA have had healthy pregnancies with appropriate monitoring. The goal is planned pregnancy during remission with multidisciplinary oversight.
Medication Side Effects
Long-term corticosteroid use — often unavoidable in TA — causes predictable complications that require proactive prevention:
- Osteoporosis: All patients on long-term steroids should receive calcium, vitamin D3, and a bisphosphonate (e.g., alendronate) unless contraindicated. Baseline DEXA scan at diagnosis.
- Hyperglycemia and diabetes: Monitor fasting glucose and HbA1c; dietary modification and metformin may be needed.
- Weight gain and Cushingoid features: Emotionally difficult for young women; counsel proactively and refer to dietitian.
- Immunosuppression: Increased risk of infections; screen for TB and hepatitis B/C before starting immunosuppressants; ensure vaccinations are up to date (avoid live vaccines during active immunosuppression).
Driving and Safety Considerations
Patients with severe carotid or vertebral artery stenosis may experience drop attacks or sudden dizziness, which can impair driving safety. Discuss with the specialist whether any driving restrictions are appropriate based on individual vascular anatomy.
Regular Specialist Follow-Up
TA requires ongoing monitoring by a rheumatologist experienced in large-vessel vasculitis, ideally in a dedicated vasculitis clinic. Annual vascular imaging (MRA or ultrasound), regular ophthalmology follow-up, and careful cardiovascular risk management are the pillars of long-term care. Patient-held disease summaries (listing which vessels are involved, the current medication regimen, and emergency contact details for the specialist team) are invaluable when patients need care in settings outside their primary center.
10. Prognosis
Modern immunosuppressive therapy and vascular surgical techniques have substantially improved the prognosis of Takayasu Arteritis over the past four decades. However, TA remains a relapsing, progressive disease for most patients, and long-term outcomes depend heavily on which vessels are involved, how quickly the diagnosis is made, and whether disease activity can be controlled before permanent ischemic damage occurs.
Survival
10-year survival exceeds 90% in most modern series from specialized centers in Japan, Europe, and North America. This represents a dramatic improvement over pre-biologic era estimates. The major causes of death are:
- Stroke from carotid or vertebral artery occlusion
- Myocardial infarction from coronary ostial stenosis or accelerated atherosclerosis driven by chronic inflammation and steroid-induced cardiovascular risk factors
- Heart failure from progressive aortic regurgitation or hypertensive cardiomyopathy
- Complications of renovascular hypertension (renal failure, hypertensive emergency)
- Aortic aneurysm rupture — a less common but catastrophic outcome
Disease Course Patterns
Three distinct disease course patterns have been described:
- Monophasic (approximately 20%): A single episode of active disease, followed by sustained remission without relapse. These patients may eventually be weaned off immunosuppression.
- Polycyclic (approximately 20%): Discrete episodes of active disease separated by genuine remissions, with relative stability between flares.
- Chronic continuous (approximately 60%): Ongoing low-grade or high-grade disease activity that never fully remits, requiring continuous immunosuppression. This pattern is associated with the greatest cumulative vascular damage and medication burden.
Relapse
Relapse rates are uniformly high across all published series: 50–80% of patients relapse at some point, typically during or after corticosteroid tapering. This relapse rate drives the current practice of adding steroid-sparing agents early and maintaining them long-term. Biologic therapies (particularly tocilizumab and anti-TNF agents) appear to reduce relapse frequency in refractory patients, but do not eliminate it.
Morbidity
Even with survival dramatically improved, long-term morbidity from TA is substantial:
- Many patients develop fixed vascular damage (stenoses, occlusions, aneurysms) that persists even after inflammatory remission is achieved, causing ongoing ischemic symptoms and functional limitation.
- Aortic regurgitation requiring surgical valve replacement occurs in 20–25% over a lifetime of disease.
- Renovascular hypertension often requires both vascular intervention and ongoing antihypertensive therapy.
- Side effects of long-term immunosuppression — particularly osteoporosis, diabetes, and cataracts from corticosteroids — add to the long-term disability burden.
Factors Associated with Better Outcomes
- Early diagnosis before extensive arterial stenosis has developed
- Prompt initiation of combination immunosuppression (steroids + steroid-sparing agent)
- Access to a specialist center with expertise in large-vessel vasculitis
- Monophasic or polycyclic disease course (vs. chronic continuous)
- Disease limited to the aortic arch branches (Type I) vs. whole-aorta involvement (Type V)
11. Research Papers
The following peer-reviewed publications represent key milestones in understanding and treating Takayasu Arteritis.
- Takayasu M. Case with unusual changes of the central vessels in the retina. Acta Societatis Ophthalmologicae Japonicae. 1908;12:554–555. (Historical founding report — no PubMed record. Search: PubMed: Takayasu arteritis history.)
- Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum. 1990;33(8):1129–1134. PMID: 2202311
- Ishikawa K. Diagnostic approach and proposed criteria for the clinical diagnosis of Takayasu's arteriopathy. J Am Coll Cardiol. 1988;12(4):964–972. — Search PubMed
- Kerr GS, et al. Takayasu arteritis. Ann Intern Med. 1994;120(11):919–929. — Search PubMed
- Hoffman GS, et al. Treatment of glucocorticoid-resistant or relapsing Takayasu arteritis with methotrexate. Arthritis Rheum. 1994;37(4):578–582. — Search PubMed
- Numano F. Differences in clinical presentation, frequency, and laboratory findings in Takayasu arteritis. Curr Opin Rheumatol. 2000;12(1):18–23. — Search PubMed
- Nakaoka Y, et al. Efficacy and safety of tocilizumab in patients with refractory Takayasu arteritis: TAKT study. Ann Rheum Dis. 2018;77(3):348–354. — Search PubMed
- Comarmond C, et al. Long term outcomes and prognostic factors of complications in Takayasu's arteritis. Circulation. 2017;136(12):1114–1122. — Search PubMed
- Hellmich B, et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. 2020;79(1):19–30. PMID: 31270110
- Grayson PC, et al. 2022 American College of Rheumatology/EULAR Classification Criteria for Takayasu Arteritis. Arthritis Rheumatol. 2022;74(12):1872–1880. — Search PubMed
- Onen F, et al. Comparison of tocilizumab-based therapy and conventional treatment in Takayasu arteritis. Clin Exp Rheumatol. 2020;38 Suppl 124(2):82–88. — Search PubMed
- Misra R, et al. Indian Rheumatology Association consensus statement on the diagnosis and treatment of aortitis. Indian J Rheumatol. 2013;8:S105–S109. (Indian expert consensus — no indexed PMID. Search: PubMed: Takayasu arteritis India treatment.)
Search PubMed for More Research
- Takayasu arteritis treatment
- Takayasu arteritis tocilizumab
- Large vessel vasculitis classification 2022
- Takayasu arteritis FDG-PET imaging
- Takayasu arteritis pregnancy outcomes
12. Connections
- Vasculitis — overview of all vessel-size categories
- Giant Cell Arteritis — the other major large-vessel vasculitis
- Aortic Aneurysm — a complication of TA vessel wall destruction
- Antiphospholipid Syndrome — differential for arterial thrombosis in young women
- Polymyalgia Rheumatica — frequently accompanies Giant Cell Arteritis
- Behcet's Disease — another systemic vasculitis affecting young adults
- Rheumatoid Arthritis — shares steroid and methotrexate treatment strategies
- Lupus (SLE) — autoimmune overlap and young women population
- Polyarteritis Nodosa — medium-vessel vasculitis differential
- EGPA (Eosinophilic Granulomatosis with Polyangiitis) — granulomatous vasculitis
- IgG4-Related Disease — causes aortitis and must be excluded in TA workup
- Hypertension — renal artery stenosis in TA drives severe, often treatment-resistant renovascular hypertension.
- Rheumatology — all conditions