Premenstrual Dysphoric Disorder (PMDD)
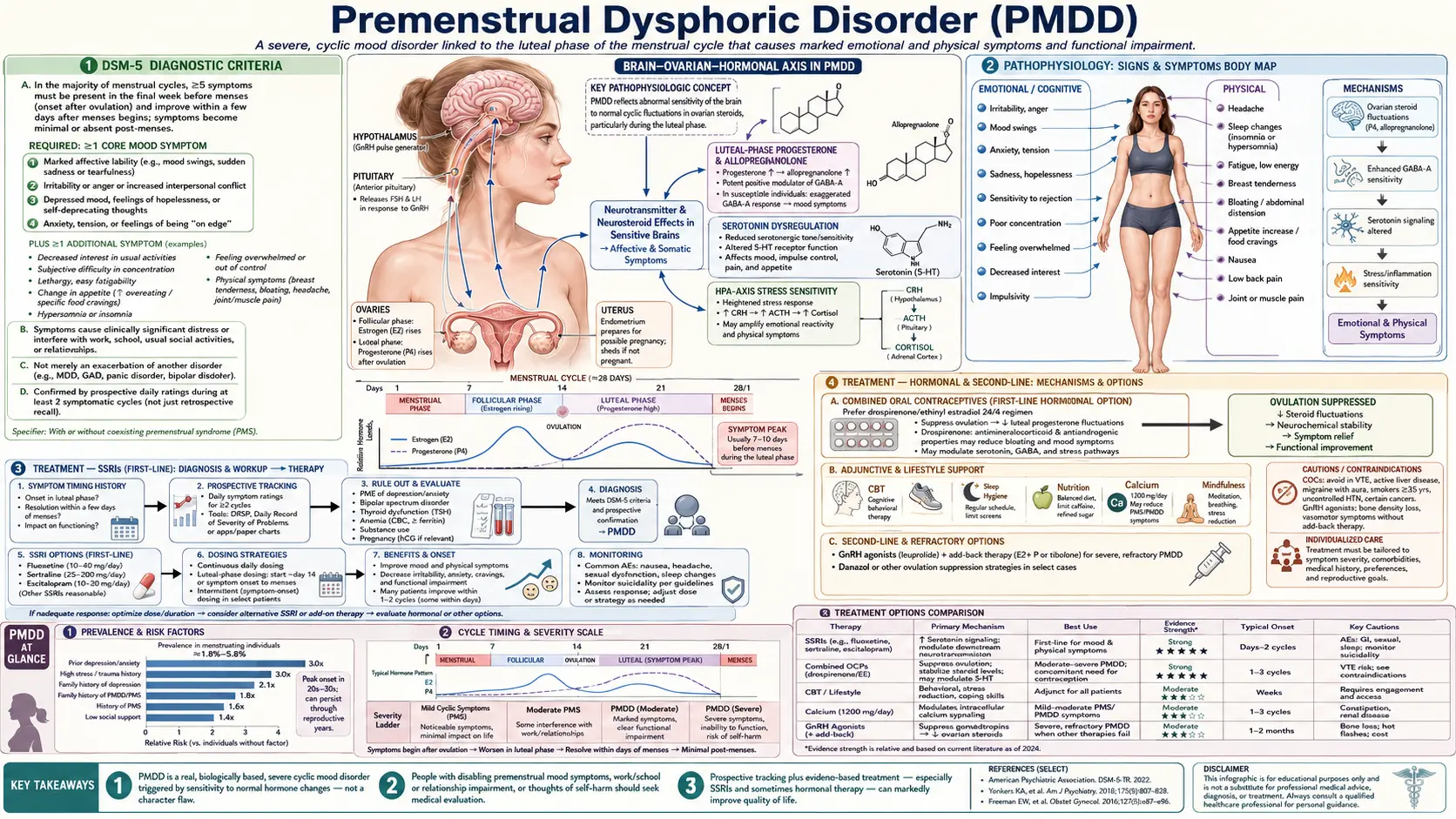
Premenstrual Dysphoric Disorder (PMDD) is a severe, cyclic mood disorder rooted in a biological sensitivity of the brain to normal hormonal fluctuations — not a character flaw or exaggerated emotionality. It affects 3–8% of menstruating women and was formally recognized as a distinct DSM-5 diagnosis in 2013. The hallmark is predictable timing: symptoms emerge in the luteal phase (after ovulation, roughly days 14–28 of a 28-day cycle) and remit within days of menstrual onset, leaving a symptom-free follicular phase. This distinguishes PMDD from ordinary premenstrual syndrome (PMS), which affects 70–90% of women with milder, less impairing symptoms.
The central mechanism involves allopregnanolone, a progesterone metabolite that normally acts as a calming modulator of GABA-A receptors. In PMDD, the brain responds paradoxically — what should be calming triggers anxiety and irritability. Genetics play a role: research by Benca and colleagues (2017, Molecular Psychiatry) demonstrated that the ESC/E(Z) epigenetic complex shows differential gene expression in lymphocytes from PMDD patients compared to healthy controls, suggesting a genomic sensitivity to ovarian steroids that operates across tissues. PMDD is a medically recognized biological condition with effective treatments.
- DSM-5 Diagnostic Criteria
- Pathophysiology
- Treatment — SSRIs (First-Line)
- Treatment — Hormonal and Second-Line
- Non-Pharmacological Treatments
- Diagnosis and Prospective Charting
- Disability and Quality of Life
- Suicidality and Crisis Planning
- Key Research Papers
- Connections
Interactive Visualization Serotonin, Mood & SSRIs — build it, fire it, block reuptake Assemble serotonin from tryptophan, fire it across the synapse, then take an SSRI and watch the cleft flood — or starve the tryptophan and watch the signal fade. Launch →
DSM-5 Diagnostic Criteria
The DSM-5 requires that a patient experience five or more symptoms in most menstrual cycles during the final week before menses onset, with those symptoms improving within a few days after menses begins, and becoming minimal or absent in the week following menstruation. This cyclicity — documented prospectively, not recalled retrospectively — is the cornerstone of the diagnosis.
At least one of the following core mood symptoms must be present: (1) marked affective lability such as sudden tearfulness, sadness, or increased sensitivity to rejection; (2) marked irritability, anger, or increased interpersonal conflicts; (3) marked depressed mood, feelings of hopelessness, or self-deprecating thoughts; or (4) marked anxiety, tension, or feelings of being keyed up or on edge.
Additional symptoms that contribute toward the five-symptom threshold include: decreased interest in usual activities such as work, hobbies, and socializing; difficulty concentrating; marked lethargy, easy fatigability, or lack of energy; marked change in appetite, overeating, or specific food cravings; hypersomnia or insomnia; a subjective sense of being overwhelmed or out of control; and physical symptoms such as breast tenderness or swelling, joint or muscle pain, bloating, or a sensation of weight gain.
The symptoms must cause clinically significant distress or interfere with work, school, social activities, or relationships, and must not be attributable to the physiological effects of a substance or another medical condition. The pattern must be confirmed by prospective daily ratings for at least two symptomatic cycles using a validated instrument such as the Daily Record of Severity of Problems (DRSP). Digital tracking apps including Clue and Kindara have been validated for this purpose and can streamline the documentation process.
A critical differential is premenstrual exacerbation (PME) of an underlying condition — depression, anxiety disorder, migraine, or irritable bowel syndrome can all worsen in the luteal phase without representing true PMDD. In PME, symptoms are present throughout the cycle and amplify premenstrually; in PMDD, the follicular phase is genuinely symptom-free. Retrospective recall systematically underestimates symptom intensity and misses this distinction, which is why prospective charting is mandatory.
Pathophysiology
PMDD is fundamentally a disorder of central nervous system sensitivity to normal ovarian steroid cycling — not an abnormality in hormone levels themselves. This distinction is supported by three key lines of evidence. First, administering a GnRH (gonadotropin-releasing hormone) agonist to suppress ovarian cycling eliminates PMDD symptoms in the majority of patients. Second, when progesterone is added back to these women, it re-triggers PMDD symptoms — but not in women without PMDD. Third, adding back estrogen alone does not trigger symptoms, implicating progesterone and its metabolites rather than estrogen as the proximate trigger.
The central player is allopregnanolone (3α-hydroxy-5α-pregnan-20-one; also called 3α-THP), a neurosteroid synthesized primarily from progesterone in the brain and adrenal glands. Allopregnanolone is a potent positive allosteric modulator of GABA-A receptors, particularly the extrasynaptic δ-subunit-containing receptors that mediate tonic (continuous background) inhibition in neurons. Allopregnanolone concentrations rise significantly during the luteal phase. Under normal circumstances this rise produces anxiolytic, sedating, and calming effects — similar in mechanism to alcohol and benzodiazepines, though through different binding sites.
In women with PMDD, altered expression and sensitivity of GABA-A receptor subunits and abnormalities in the serotonin system cause this ordinarily calming neurosteroid to produce a paradoxical excitatory effect — anxiety, irritability, and dysphoria rather than calm. This paradox is mechanistically similar to what is seen during alcohol withdrawal, where changes in GABA-A receptor composition during chronic alcohol exposure cause anxiety when GABA-A activity is restored. It explains why brexanolone (IV-administered allopregnanolone, approved for postpartum depression) works effectively — the dosing and delivery bypasses the sensitized receptors — while oral progesterone supplements reliably worsen PMDD symptoms.
The serotonin system is also implicated. Women with PMDD show reduced serotonin transporter (5-HTT) function during the luteal phase, lower platelet serotonin levels, and altered 5-HT1A receptor activity. This serotonergic dysregulation explains why SSRIs — which do not acutely elevate serotonin levels but modulate serotonin receptor sensitivity — produce therapeutic effects within days in PMDD, far faster than their weeks-long onset in major depression. The rapid response suggests SSRIs are acutely modulating neuroactive steroid synthesis or receptor sensitivity rather than correcting a classical monoamine deficit.
Genetic research has added another layer. The study by Benca et al. (2017) found that lymphocytes from PMDD patients — cells completely outside the brain — show different patterns of gene expression from the ESC/E(Z) epigenetic regulatory complex compared to healthy controls. This epigenetic sensitivity appears to affect how genes across multiple cell types respond to ovarian steroids, suggesting PMDD reflects a genome-wide sensitivity rather than a purely localized brain vulnerability.
Treatment — SSRIs (First-Line)
Selective serotonin reuptake inhibitors (SSRIs) are the established first-line pharmacological treatment for PMDD, supported by extensive randomized controlled trial evidence and three FDA approvals. Fluoxetine (marketed as Sarafem specifically for PMDD; 20 mg/day) was the first FDA-approved treatment. Sertraline (50–150 mg/day) and paroxetine CR (12.5–25 mg/day) are also FDA-approved. Paroxetine warrants caution with intermittent dosing strategies due to its short half-life and discontinuation symptoms.
The most striking feature of SSRI treatment in PMDD is the speed of response. Unlike major depression where 4–6 weeks is typically required to detect clinical benefit, PMDD patients often report meaningful improvement within the first 1–2 days of SSRI administration and within 1–2 menstrual cycles of starting treatment. This rapid onset — faster than any possible synaptic serotonin level change — strongly suggests that the therapeutic mechanism involves acute modulation of neuroactive steroid synthesis or GABA-A receptor sensitivity rather than classic monoamine reuptake inhibition.
Two main dosing strategies are available with comparable efficacy:
- Continuous dosing — the SSRI is taken every day of the cycle at standard doses. Preferred when follicular-phase symptoms are present, when the patient has difficulty tracking her cycle, or when cycle irregularity makes luteal-phase timing unreliable.
- Luteal-phase dosing — the SSRI is started approximately on day 14 of the cycle (after confirmed ovulation, ideally with OPK or cycle-tracking confirmation) and discontinued with menses onset or 1–2 days after. This strategy is equally effective to continuous dosing in multiple studies and meta-analyses (Freeman et al. 2004). It reduces total medication exposure, side-effect burden, and cost. Standard doses: sertraline 50 mg/day or fluoxetine 20 mg/day during the luteal phase.
Overall SSRI response rates in PMDD are approximately 65–75%, substantially higher than in major depression. Non-response to one SSRI does not predict non-response to another — switching within the class is reasonable before moving to second-line treatments. Common side effects during the luteal phase include nausea (often transient), insomnia, sexual dysfunction, and headache. These are generally milder with intermittent luteal-phase dosing.
Treatment — Hormonal and Second-Line
GnRH agonists (leuprolide acetate, nafarelin, buserelin) produce a medical "chemical ovariectomy" by downregulating pituitary GnRH receptors, suppressing LH and FSH, and eliminating ovarian cycling entirely. Because PMDD depends on luteal-phase hormonal cycling, GnRH agonists are 75–100% effective for PMDD symptoms. However, prolonged use produces menopausal side effects — hot flashes, vaginal dryness, insomnia, and critically, bone mineral density loss that becomes significant beyond 6 months of continuous use. Add-back therapy (low-dose estrogen plus a low-dose progestin) can extend GnRH agonist use while partially mitigating bone loss and vasomotor symptoms, though it reintroduces some hormonal fluctuation. GnRH agonists are most appropriate for severe treatment-resistant PMDD, or as a diagnostic and therapeutic bridge for women considering oophorectomy.
Oral contraceptives vary substantially in their effect on PMDD. The drospirenone-containing combined oral contraceptive YAZ (3 mg drospirenone + 20 mcg ethinyl estradiol, extended 24/4 regimen) is FDA-approved for PMDD. Drospirenone is a progestin with anti-androgenic and antimineralocorticoid (anti-aldosterone) properties that distinguish it from older progestins. The PRISM trial (Pearlstein et al. 2005) demonstrated significant reductions in PMDD symptom scores versus placebo. Continuous or extended cycling (minimizing hormone-free intervals) is preferred in PMDD to avoid withdrawal-related symptom recurrence. By contrast, levonorgestrel-containing pills and some other progestin formulations can worsen mood symptoms in susceptible women and should be used cautiously or avoided in PMDD patients.
Spironolactone (50–100 mg/day during the luteal phase) is an aldosterone antagonist with anti-androgenic activity. It reduces bloating, breast tenderness, and water retention — the physical symptom cluster of PMDD — and provides modest mood benefit. It requires monitoring of serum potassium (risk of hyperkalemia, particularly with NSAIDs, ACE inhibitors, or ARBs), blood pressure, and renal function. It is most useful for patients whose predominant complaint is physical symptom burden rather than severe mood dysregulation.
Alprazolam (a short-acting benzodiazepine) in low doses during the luteal phase has been studied in treatment-resistant PMDD with predominant anxiety. Evidence is modest; dependency risk is significant. It is reserved for carefully selected refractory cases managed by specialists familiar with benzodiazepine prescribing.
Calcium carbonate at 1200 mg/day (elemental calcium) has consistent, if modest, RCT evidence for reducing both mood and physical symptoms of PMDD. A large NCRR-funded RCT (Thys-Jacobs et al. 1998) reported significant reductions in negative affect, water retention, food cravings, and pain compared to placebo over two menstrual cycles. The mechanism may involve calcium's role in regulating calcitriol and serotonin synthesis, or correction of subclinical calcium deficiency common in menstruating women. It is inexpensive, safe, and worth adding as an adjunct to primary treatment.
Vitamin B6 (pyridoxine, 50–100 mg/day) has been studied as adjunctive therapy. Evidence is mixed; doses above 100 mg/day risk peripheral neuropathy with prolonged use. Magnesium supplementation has modest evidence for physical symptom reduction. Neither replaces first-line treatment but may reduce overall symptom burden when combined with SSRI therapy.
Non-Pharmacological Treatments
Cognitive behavioral therapy (CBT) has randomized controlled trial evidence in PMDD. CBT targeting PMDD addresses catastrophizing around symptom recurrence, emotion regulation skills, interpersonal communication strategies for the luteal phase, and behavioral activation to counteract social withdrawal. A key CBT principle in PMDD is anticipatory coping — patients learn to recognize the luteal phase early, prepare coping strategies in advance, and reduce impulsive decisions (quitting jobs, ending relationships) that are temporally associated with peak symptoms but often regretted in the follicular phase. CBT is particularly useful for patients who prefer not to use medications, those with mild-moderate symptom severity, or as an adjunct to pharmacotherapy for residual psychosocial impairment.
Aerobic exercise demonstrates consistent benefit across observational studies and several controlled trials. Regular aerobic exercise at least 4 times per week appears to reduce overall PMDD severity, including both mood and physical symptom components. Proposed mechanisms include endorphin release, serotonin system modulation, and reduction of the inflammatory signaling that correlates with luteal-phase symptom peaks. Exercise timing across the cycle does not appear to substantially alter the benefit — consistent routine matters more than strategic cycling-phase timing.
Dietary modifications are commonly recommended on the basis of mechanistic plausibility and patient-reported benefit, though RCT evidence is limited. Reduced caffeine intake (caffeine is anxiogenic and worsens irritability and insomnia, symptoms that are already amplified in the PMDD luteal phase) and reduced alcohol consumption (alcohol disrupts sleep architecture, worsens dysphoria via rebound effects, and interacts with allopregnanolone-GABA pathways) are prudent recommendations for symptomatic luteal-phase management. Reducing refined sugar and sodium may help with physical symptom burden — bloating, fluid retention, and energy crashes — though the evidence base is largely observational.
Sleep hygiene optimization is important because sleep deprivation dramatically worsens mood dysregulation, irritability, and the capacity to manage interpersonal conflict — all PMDD symptoms. Consistent sleep and wake times, minimizing blue-light exposure before bed, and avoiding caffeine after noon are standard recommendations that carry particular value in the symptomatic luteal phase.
Bright light therapy has preliminary evidence for benefit in PMDD, particularly for patients who notice seasonal worsening of their luteal-phase symptoms — a recognized overlap between PMDD and seasonal affective disorder (SAD). Standard bright-light devices (10,000 lux, 20–30 minutes in the morning) carry an excellent safety profile. Acupuncture has been investigated in several small randomized trials with mixed but generally positive results; evidence is insufficient to recommend it as a primary treatment but it can be offered as a complementary option for patients who prefer integrative approaches.
Diagnosis and Prospective Charting
The diagnosis of PMDD cannot be established on the basis of history alone. Prospective daily symptom charting across at least two consecutive symptomatic cycles is required. This requirement exists because retrospective recall of premenstrual symptoms is systematically inaccurate — women tend to recall symptoms as worse than daily ratings confirm, and recall bias can produce apparent PMDD in women who actually have premenstrual exacerbation of another condition. Multiple studies have found that 30–50% of women who report PMDD by history do not meet criteria on prospective charting.
The Daily Record of Severity of Problems (DRSP) is the most widely used and validated instrument for prospective PMDD charting. It rates 21 items daily on a scale of 1–6, spanning mood symptoms, behavioral changes, and physical complaints. The pattern that confirms PMDD is a clear premenstrual rise beginning after ovulation, peak in the luteal phase, and fall to near-baseline within 2–4 days of menstrual onset, followed by a symptom-free follicular phase.
Digital tracking applications have made prospective charting far more feasible in clinical practice. Apps such as Clue, Kindara, and MigraineX allow daily symptom logging with graphical displays that can be exported or reviewed at follow-up appointments. When recommending daily charting, clinicians should explain the purpose — not to dismiss the patient's experience but to confirm the pattern that determines the most effective treatment strategy. Many patients find that charting itself is therapeutic because it objectifies what felt like unpredictable chaos.
The laboratory workup for suspected PMDD is relatively brief, aimed at excluding conditions that can masquerade as or coexist with PMDD. Thyroid-stimulating hormone (TSH) should be obtained to exclude hypothyroidism, which causes fatigue, depression, and cognitive changes that are not cycle-dependent but may appear to worsen premenstrually in susceptible women. A complete blood count (CBC) can identify iron-deficiency anemia contributing to fatigue and cognitive difficulties. Follicle-stimulating hormone (FSH) is appropriate in perimenopausal women to assess ovarian reserve, as the hormonal transitions of perimenopause frequently worsen or unmask PMDD-like symptoms.
The critical differential diagnosis to exclude at the diagnostic stage is premenstrual exacerbation (PME) of a primary psychiatric disorder. Depression, generalized anxiety disorder, bipolar disorder, PTSD, and obsessive-compulsive disorder all commonly worsen premenstrually without fulfilling PMDD criteria — because symptoms persist (at lower intensity) throughout the follicular phase. The clinical implication is important: in PME, the primary condition requires treatment, not PMDD-specific interventions. Prospective charting reliably distinguishes the two by demonstrating whether a symptom-free follicular window truly exists.
Disability and Quality of Life
The functional impact of PMDD is frequently underestimated by clinicians, employers, and family members — and often by patients themselves, who may have internalized the cultural message that premenstrual symptoms are normal and should be endured. In reality, severe PMDD causes clinically significant functional impairment for an average of 7–14 days per month — one-quarter to one-half of a woman's adult life spent in a state of significant psychological and physical distress.
Occupational impact is substantial. Women with PMDD report significantly higher rates of work absenteeism and presenteeism (reduced productivity while at work) during the luteal phase compared to controls. A large European study found that PMDD was associated with work impairment comparable to that seen in major depression — a condition universally recognized as disabling. Academic performance shows analogous impairment in students, with test anxiety, concentration difficulties, and social withdrawal clustering in luteal-phase weeks.
Relationship impact is also severe. Marital and partnership conflict peaks during the luteal phase in PMDD patients; partners report unpredictable anger, emotional distance, and rejection sensitivity that strains relationships over time. Critically, partners who understand the biological basis of PMDD — that the person they love is experiencing a predictable, biologically driven state — demonstrate markedly better coping and relationship satisfaction than those who attribute symptoms to personality or willfulness. Partner psychoeducation is an underutilized therapeutic tool.
Co-occurring conditions are common in PMDD and compound functional impairment. Major depression and anxiety disorders are the most prevalent comorbidities. PTSD is significantly overrepresented in PMDD patients, though the causal direction is uncertain — the hyperarousal and emotional reactivity of PTSD may share neurobiological pathways with PMDD sensitivity. Endometriosis occurs at elevated rates in PMDD patients, creating a compound burden of physical pain and mood dysregulation that is often underdiagnosed and undertreated. Chronic pain conditions, migraine (with documented perimenstrual migraine clustering), and irritable bowel syndrome (IBS, which worsens premenstrually in many women) also co-occur with PMDD.
A critical message for patients is that PMDD is not a personality disorder, not a character flaw, and not a choice. Biological conditions that impair functioning deserve treatment. Validation — from clinicians, partners, employers, and the patient herself — is itself therapeutic. Many women with PMDD have spent years being told that their suffering is "just PMS," "all in their head," or a sign of emotional immaturity. Providing an accurate biological framework for PMDD frequently produces substantial relief independent of any pharmacological intervention.
Suicidality and Crisis Planning
A significant and underrecognized subgroup of women with PMDD experiences passive suicidal ideation, active suicidal ideation, or self-harm ideation confined to the luteal phase, resolving spontaneously with menstrual onset. A landmark study by Pilver et al. (2011) in the American Journal of Psychiatry confirmed that PMDD is independently associated with suicidal ideation and suicide attempts, controlling for depression and anxiety. Population-based data suggest that 15–30% of women with PMDD report some degree of luteal-phase suicidal ideation. Hospitalizations for self-harm and suicidal crises cluster during the luteal phase in this population.
The paradox of PMDD-associated suicidality is that it is simultaneously serious and, in most cases, highly predictable and time-limited. Unlike suicidal ideation in major depression — which may be persistent, escalating, and poorly bounded — PMDD suicidal ideation is typically self-terminating within days of menstrual onset. The patient herself often knows this from prior cycles. This cyclicity can be a source of resilience when properly communicated and incorporated into a safety plan: "I know this is the PMDD, I know it will pass in approximately X days, and I have a plan to keep myself safe until it does."
Clinical management of suicidality in PMDD:
- Assess and document suicidal ideation at every visit, including cycle phase at time of assessment. Ideation rated during the follicular phase substantially underestimates luteal-phase risk.
- Psychoeducation about cyclicity — explain that the ideation is a symptom of the disorder, not a reflection of the patient's true desires or the reality of her situation. Many patients find this framing profoundly relieving.
- Written safety plan for the luteal phase — developed in advance, during the follicular phase when the patient is clearest, covering warning signs, coping strategies, crisis contacts (National Suicide Prevention Lifeline: 988), and means restriction.
- Means restriction — in severe cases, reduce access to lethal means during the luteal phase (e.g., firearm storage with a trusted person, medication lockboxes).
- Pharmacological urgency — in patients with luteal-phase suicidality, SSRI initiation is urgent, not optional. The rapid SSRI response in PMDD — often within days — means treatment can reduce suicidal ideation within the same or following cycle.
- GnRH agonist for severe, refractory cases — eliminating ovarian cycling eliminates the luteal-phase trigger for suicidal ideation; this may be medically appropriate as a bridge to more definitive management in women with severe PMDD and recurrent suicidal crises.
Clinicians should approach PMDD-related suicidality with the same seriousness as any other suicidal ideation while communicating the biology of cyclicity clearly — both to reduce stigma and to provide the patient with an evidence-based framework for understanding her own experience. Statements like "that's just your hormones talking" are dismissive and clinically harmful; "your brain is responding to a hormonal signal in a way we can treat" is accurate, validating, and actionable.
Key Research Papers
- Benca CE et al. (2017). Differential gene expression of the ESC/E(Z) epigenetic complex in premenstrual dysphoric disorder. Molecular Psychiatry. Search PubMed
- Hantsoo L, Epperson CN. (2015). Premenstrual Dysphoric Disorder: Epidemiology and Treatment. Current Psychiatry Reports. PMID 26377947
- Yonkers KA et al. (2008). Premenstrual syndrome. Lancet. Search PubMed
- Pearlstein TB et al. (2005). Treatment of premenstrual dysphoric disorder with a new drospirenone-containing oral contraceptive formulation. Contraception. Search PubMed
- Endicott J et al. (1999). Premenstrual changes and emotional and physical well-being. American Journal of Obstetrics and Gynecology. Search PubMed
- Pilver CE et al. (2011). Premenstrual dysphoric disorder and suicidality. American Journal of Psychiatry. Search PubMed
- Rubinow DR, Schmidt PJ. (2006). Gonadal steroid regulation of mood: the lessons of premenstrual syndrome. Frontiers in Neuroendocrinology. Search PubMed
- Freeman EW et al. (2004). Luteal phase administration of agents for the treatment of premenstrual dysphoric disorder. CNS Drugs. Search PubMed
- Rapkin AJ. (2003). A review of treatment of premenstrual syndrome and premenstrual dysphoric disorder. Psychoneuroendocrinology. Search PubMed
- Halbreich U et al. (2003). The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder. Psychoneuroendocrinology. Search PubMed
- Backstrom T et al. (2003). The role of hormones and hormonal treatments in premenstrual syndrome. CNS Drugs. Search PubMed
- Steiner M et al. (2006). Premenstrual dysphoria and the serotonin system: pathophysiology and treatment. Archives of Women's Mental Health. Search PubMed
Connections
- Psychiatry
- Serotonin, Mood & SSRIs — interactive animation
- PMS and PMDD
- Postpartum Depression
- Depression
- Anxiety
- Seasonal Affective Disorder
- Insomnia
- Eating Disorders
- Borderline Personality Disorder
- Magnesium
- Calcium
- Vitamin B6
- Endometriosis