Bulimia Nervosa
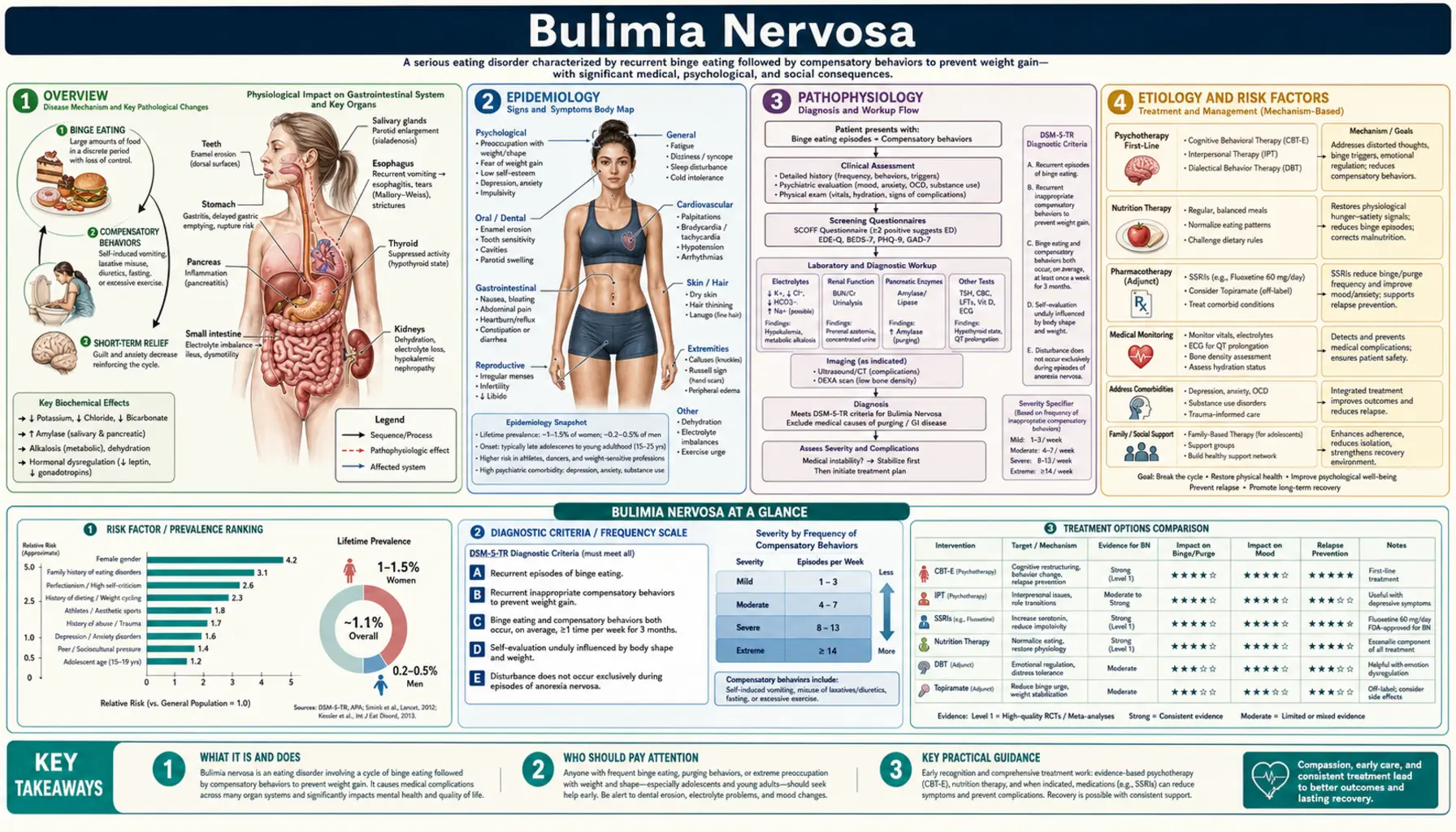
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Medical Complications
- Diagnosis
- Treatment
- Binge Eating Disorder
- Prognosis and Recovery
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Bulimia Nervosa (BN) is a serious eating disorder defined by recurrent cycles of binge eating — consuming a large amount of food in a discrete period accompanied by a subjective sense of loss of control — followed by compensatory behaviors intended to prevent weight gain. Unlike anorexia nervosa, most people with bulimia nervosa maintain a normal to above-normal body weight, which frequently delays recognition and treatment.
The term was coined by British psychiatrist Gerald Russell in 1979, who described it as "an ominous variant of anorexia nervosa." The DSM-5 recognizes bulimia nervosa as a distinct eating disorder within the Feeding and Eating Disorders chapter, separate from anorexia nervosa and binge eating disorder. A defining psychological feature is that self-evaluation is unduly influenced by body shape and weight — the individual's sense of self-worth rises and falls with perceived control over eating and body appearance.
Shame and secrecy are central to the illness. Binge-purge cycles typically occur in private, and most patients conceal the behavior for years before seeking help. This secrecy, combined with the absence of the low body weight that often prompts medical attention in anorexia, means bulimia nervosa is significantly underdiagnosed. The average duration from onset to treatment is 5-10 years.
2. Epidemiology
Bulimia nervosa has a lifetime prevalence of approximately 1-3% in women and 0.5% in men. Point prevalence in high-risk groups — young women ages 16-35 — may reach 4-8%. It is the most commonly occurring eating disorder in clinical settings in Western countries. The female-to-male ratio is approximately 10:1 in clinical samples, though community studies suggest the ratio may be closer to 4:1, indicating significant underdiagnosis in males.
Peak age of onset is 16-20 years, later than anorexia nervosa (14-18 years) but still concentrated in adolescence and young adulthood. Onset before puberty is rare. Incidence appears to have peaked in the 1980s-1990s with Western dietary culture and may be decreasing slightly in recent cohorts, though prevalence remains high. BN is substantially more common in Western industrialized nations and in societies that idealize thinness, though it is increasingly recognized globally.
High-risk populations include ballet dancers, gymnasts, wrestlers, models, and athletes in weight-category sports — groups with performance pressures tied to body weight. College women show elevated prevalence (~3-5%). LGBTQ+ individuals, particularly gay and bisexual men, show higher rates than heterosexual men. Racial and ethnic disparities in diagnosis exist — Black, Hispanic, and Asian women are often underdiagnosed relative to White women despite similar or higher rates of disordered eating behaviors.
3. Pathophysiology
Neurobiological Reward Dysregulation
The binge-purge cycle in bulimia nervosa is maintained by a dysregulated reward system. Neuroimaging studies demonstrate altered dopaminergic signaling in the striatum, nucleus accumbens, and prefrontal cortex — the same circuitry implicated in substance use disorders. During binge eating, high-palatability foods trigger an exaggerated dopamine release in the mesolimbic pathway, producing a brief reward "rush." This is followed by a rapid drop-off, with dysphoria and guilt driving the compensatory purge, which in turn reduces acute distress — negatively reinforcing the cycle.
Serotonin dysregulation is particularly important in BN. Low central serotonin activity correlates with impulsivity, mood lability, and carbohydrate craving — all core features. Post-illness recovery studies show that acute tryptophan depletion (reducing serotonin precursor availability) rapidly reinstates depressed mood and body-image disturbance in recovered BN patients but not healthy controls, suggesting a trait serotonergic vulnerability that persists beyond the illness episode.
Hypothalamic Regulation of Hunger and Satiety
Normal satiety signaling is impaired in bulimia nervosa. Studies demonstrate reduced cholecystokinin (CCK) release following meals — CCK normally signals satiety via the vagus nerve to the hypothalamus. Leptin resistance and altered ghrelin dynamics (the hunger hormone) further undermine normal meal termination. Repeated purging behavior may worsen these dysregulations over time, creating a physiological substrate that perpetuates binging independent of the initial psychological triggers.
Cognitive and Emotional Processing
Functional neuroimaging reveals hyperactivation of the anterior insula (interoception and body awareness) combined with prefrontal hypoactivity (impulse control and cognitive reappraisal) in BN patients viewing food or body-related stimuli. This pattern mirrors the neurobiological signature of impulse-control disorders. Emotional regulation deficits are central: binges are frequently triggered by negative affect states (anxiety, boredom, loneliness, anger) and are perceived as tension-relieving, at least transiently.
4. Etiology and Risk Factors
Genetic Factors
- Heritability estimated at 55-83% from twin studies — comparable to or exceeding anorexia nervosa
- First-degree relatives of individuals with BN have a 3-10 fold increased risk of eating disorders
- Shared genetic architecture with major depressive disorder, anxiety disorders, and substance use disorders — reflected in high comorbidity rates
- Candidate genes implicated: 5-HT2A receptor gene (HTR2A), BDNF (brain-derived neurotrophic factor, Val66Met polymorphism), dopamine D4 receptor gene (DRD4)
Psychological Risk Factors
- Weight/shape concerns and dietary restraint — the most consistently replicated proximal risk factor; dieting precedes binge onset in most cases
- Low self-esteem and negative body image predating the illness onset
- Impulsivity and emotional dysregulation — difficulty tolerating negative affect without behavioral response
- Perfectionism — particularly socially prescribed perfectionism (belief others hold impossibly high standards)
- History of childhood trauma, particularly sexual abuse (odds ratio ~2-3 for eating disorders); emotional abuse and neglect also significant
- Anxiety disorders frequently precede BN onset, suggesting anxiety as a temperamental risk factor
Sociocultural Factors
- Thin-ideal internalization — the degree to which cultural ideals equating thinness with beauty and worth are adopted as personal standards
- Social media exposure — prospective studies link Instagram and body-comparison behaviors to eating disorder onset and maintenance
- Weight-related teasing and peer dieting during adolescence
- Weight-critical comments from family members, particularly during childhood and adolescence
- Participation in activities emphasizing weight or appearance: ballet, gymnastics, modeling, cheerleading
Biological Risk Factors
- Childhood obesity or being overweight — increases vulnerability to weight-related teasing and dieting behavior
- Early puberty — earlier menarche associated with increased risk, possibly via weight gain and social pressures
- Type 1 diabetes mellitus — "diabulimia" (deliberate insulin omission for weight control) occurs in ~30% of young women with T1DM; a dangerous combination associated with accelerated diabetic complications
5. Clinical Presentation
The Binge Episode
A binge eating episode in DSM-5 is defined by two features: (1) eating a larger amount of food than most people would eat under similar circumstances in a discrete period (typically under 2 hours); and (2) a sense of lack of control over eating. Amounts consumed can vary widely — from 1,000 to 5,000+ calories per episode — but the subjective experience of loss of control is more diagnostically important than the objective amount. Binge foods are typically high-calorie, high-fat, high-carbohydrate "forbidden" foods the individual normally restricts.
Binges often follow a predictable pattern: negative mood or interpersonal stressor → dietary restraint breaks → rapid, often mechanical eating → the binge → feelings of disgust, shame, and physical discomfort → compensatory behavior → brief relief → guilt and renewed restriction → next binge trigger. Patients frequently describe a dissociative or "autopilot" quality to binge episodes, eating until physically uncomfortable without conscious awareness of the volume consumed.
Compensatory Behaviors
Purging behaviors (80-90% of BN cases):
- Self-induced vomiting — most common, typically within 30-60 minutes of binge eating; initially requires manual stimulation but often becomes reflexive; provides immediate but incomplete calorie elimination (only 50-70% of calories expelled)
- Laxative abuse — stimulant laxatives (senna, bisacodyl) used to "prevent absorption"; largely ineffective (calories absorbed in small intestine before laxatives act in large intestine) but causes significant fluid and electrolyte loss
- Diuretic abuse — promotes water loss, not calorie loss; causes rapid hypokalemia and hyponatremia
- Enemas — less common, similar inefficacy and similar electrolyte risks as laxatives
Non-purging behaviors:
- Excessive exercise — compulsive exercise to "compensate" for calories; clinically significant when it persists despite illness/injury, causes distress when prevented, or is driven by guilt rather than enjoyment
- Fasting — extended periods of complete food restriction following a binge; contributes to the restriction-binge cycle
Physical Examination Signs
- Russell's Sign — calluses or scars on the dorsal surface of the hand, particularly the knuckles (from teeth repeatedly abrading skin during induced vomiting); present in approximately 10-15% of patients; named after Gerald Russell who described the disorder
- Parotid gland enlargement (sialadenosis) — bilateral, painless enlargement of the parotid glands producing characteristic "chipmunk cheeks"; caused by hypertrophy of salivary acinar cells in response to repeated vomiting; may persist for weeks after cessation of purging; can be confused with mumps
- Dental erosion (perimolysis) — acid-induced dissolution of dental enamel from repeated exposure to gastric acid; affects lingual (tongue-side) surfaces of upper incisors first; irreversible; dentists often identify bulimia before physicians or mental health providers
- Esophagitis and throat irritation — erosive esophagitis from acid exposure; pharyngeal erythema; submandibular lymphadenopathy
- Normal to above-normal BMI — absence of the emaciation that characterizes anorexia; can mislead clinicians into underestimating severity
6. Medical Complications
Electrolyte and Metabolic Disturbances
The most dangerous acute complications of bulimia nervosa are electrolyte abnormalities that can cause life-threatening cardiac arrhythmias:
- Hypokalemia (low potassium) — the most common and dangerous electrolyte disturbance; caused by vomiting (loss of gastric K+ and aldosterone-driven renal K+ wasting) and laxative/diuretic abuse; serum K+ below 3.0 mEq/L is a medical emergency; causes: muscle weakness, fatigue, cardiac arrhythmias, ECG changes (flattened T-waves, U-waves, QTc prolongation)
- Hypochloremic metabolic alkalosis — characteristic of vomiting-predominant BN; HCl loss from gastric acid → elevated blood pH; triggers compensatory bicarbonate retention; aldosterone release → paradoxically acidic urine despite systemic alkalosis
- Hyperchloremic metabolic acidosis — characteristic of laxative-predominant BN; loss of bicarbonate-rich colonic fluid; presents differently from vomiting-predominant type and requires different management
- Hyponatremia — dilutional or from diuretic abuse; severe hyponatremia (Na+ <125 mEq/L) risks cerebral edema and seizures
- Hypomagnesemia — contributes to cardiac arrhythmia risk and worsens hypokalemia (hypomagnesemia prevents renal K+ conservation)
Cardiovascular Complications
- Cardiac arrhythmias — electrolyte disturbances (especially hypokalemia + hypomagnesemia) cause QTc prolongation, ventricular ectopy, and potentially fatal ventricular tachycardia/fibrillation; sudden cardiac death, though less common than in anorexia, is reported
- Ipecac cardiomyopathy — historically important; ipecac syrup (once recommended for home poisoning treatment) contained emetine, a cardiotoxic alkaloid causing irreversible dilated cardiomyopathy; ipecac was withdrawn from the US market in 2003 but may persist in some households
- Mitral valve prolapse — reported at higher rates in BN patients; clinical significance debated
Gastrointestinal Complications
- Mallory-Weiss tears — longitudinal mucosal lacerations at the gastroesophageal junction from forceful vomiting; present with hematemesis (vomiting blood); usually self-limited but can be severe
- Boerhaave syndrome (spontaneous esophageal rupture) — rare but life-threatening; full-thickness esophageal perforation from vomiting pressure; surgical emergency
- Gastroparesis and delayed gastric emptying — impaired gastric motility from chronic purging; worsens the sensation of fullness that triggers bingeing
- Constipation and laxative dependence — chronic laxative abuse causes colonic hypomotility ("cathartic colon"); patients may experience severe constipation on cessation, requiring careful tapering
- Gastric dilation — rare but dangerous acute complication of massive binge eating; risk of gastric rupture
Endocrine and Reproductive Complications
- Menstrual irregularities — oligomenorrhea and irregular cycles in 40-50% of women with BN, though frank amenorrhea is less common than in anorexia nervosa (weight is usually maintained)
- Fertility impairment — higher rates of miscarriage and pregnancy complications; active BN is associated with increased obstetric risk
- Dental caries and periodontal disease — beyond enamel erosion; salivary bicarbonate reduction impairs acid buffering; increased risk of root surface caries
7. Diagnosis
DSM-5 Diagnostic Criteria for Bulimia Nervosa
- Criterion A: Recurrent episodes of binge eating. An episode is defined by: (1) eating, in a discrete period (2 hours), an amount that is larger than most individuals would eat under similar circumstances; AND (2) a sense of lack of control during the episode
- Criterion B: Recurrent inappropriate compensatory behaviors to prevent weight gain — self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise
- Criterion C: Binge eating and inappropriate compensatory behaviors both occur on average at least once a week for 3 months
- Criterion D: Self-evaluation is unduly influenced by body shape and weight
- Criterion E: Not occurring exclusively during episodes of anorexia nervosa
Severity specifiers (based on frequency of compensatory behaviors per week): Mild (1-3/week), Moderate (4-7/week), Severe (8-13/week), Extreme (14+/week).
Laboratory Evaluation
All patients with suspected BN should have baseline labs to detect electrolyte abnormalities and complications:
- Basic metabolic panel (BMP) — serum Na+, K+, Cl-, CO2 (bicarbonate), BUN, creatinine, glucose; detects hypokalemia, metabolic alkalosis (vomiting), metabolic acidosis (laxatives)
- Magnesium — often not included in BMP; critical to check, as hypomagnesemia worsens hypokalemia and independently increases arrhythmia risk
- CBC — anemia, leukopenia (less common than in anorexia)
- Serum amylase — elevated in ~70% of active BN patients due to parotid gland hyperstimulation; a useful objective marker of active purging and response to treatment
- Thyroid function tests (TSH/free T4) — hypothyroidism can cause weight gain and binge tendencies; hyperthyroidism can mimic BN anxiety features
- ECG — assess QTc interval; QTc >450ms warrants cardiology consultation; QTc >500ms is associated with high arrhythmia risk
Differential Diagnosis
Anorexia Nervosa, Binge-Purge Subtype: Differentiated by significantly low body weight meeting AN criteria — the same binge-purge behaviors with AN-level weight meet AN (binge-purge type) criteria rather than BN. Binge Eating Disorder (BED): recurrent binge eating without compensatory behaviors; often presents with overweight/obesity rather than normal weight. Kleine-Levin Syndrome: rare neurological disorder with episodic hypersomnia and compulsive eating. Kluver-Bucy Syndrome: bilateral temporal lobe damage causing hypersexuality and hyperphagia. Major Depressive Disorder with atypical features: hyperphagia and weight gain, but lacks the binge-purge cycle and body image disturbance. Borderline Personality Disorder: frequently comorbid; impulsive bingeing may occur in the context of emotional dysregulation without meeting full BN criteria.
8. Treatment
Cognitive Behavioral Therapy (CBT-E)
Enhanced Cognitive Behavioral Therapy (CBT-E), developed by Christopher Fairburn at Oxford, is the first-line, most evidence-based treatment for bulimia nervosa. Across meta-analyses, CBT-E produces binge cessation rates of 30-50% and binge/purge frequency reductions of 50-80% at treatment end. The standard protocol is 20 sessions over 20 weeks in the "focused" form, with an optional "broad" form addressing additional comorbid concerns (perfectionism, interpersonal difficulties, low self-esteem).
Core CBT-E components:
- Self-monitoring — daily food record tracking all eating, associated thoughts/feelings, and purging behaviors; externalizes the cycle and creates awareness
- Regular eating — establishing 3 planned meals + 2 snacks per day regardless of hunger signals; disrupts the dietary restraint → binge → purge cycle
- Cognitive restructuring — identifying and challenging distorted beliefs about body shape, weight, food, and self-worth; addressing overvaluation of shape and weight as the core psychopathology
- Body image interventions — reducing avoidance of body checking and exposure to feared body areas
- Relapse prevention — identifying personal high-risk situations and developing individualized coping strategies
Interpersonal Psychotherapy (IPT)
IPT achieves outcomes comparable to CBT-E over longer follow-up (8-12 months) despite acting through a completely different mechanism — targeting the interpersonal context of the eating disorder rather than eating behaviors directly. IPT identifies one of four interpersonal problem areas: grief, role disputes, role transitions, or interpersonal deficits. It is an alternative first-line option for patients who decline or do not respond to CBT-E.
Dialectical Behavior Therapy (DBT)
DBT has strong evidence for BN with comorbid borderline personality disorder or significant emotional dysregulation. DBT targets the affect dysregulation pathway to bingeing — binges occur in response to intolerable emotions, and DBT skills (distress tolerance, emotion regulation, interpersonal effectiveness, mindfulness) provide alternative coping strategies. Guided self-help DBT manuals exist for less severe presentations.
Pharmacotherapy
Fluoxetine (Prozac) 60 mg/day is the only FDA-approved pharmacotherapy for bulimia nervosa. The dose required for BN (60 mg/day) is 3× the standard antidepressant dose (20 mg/day) — this is not a typo. Fluoxetine reduces binge frequency by approximately 67% and purge frequency by approximately 56% versus placebo in clinical trials. Important caveats:
- Fluoxetine is NOT recommended as monotherapy — combination with CBT-E is superior to either alone
- Use caution in patients with active severe electrolyte abnormalities — SSRIs lower the seizure threshold, and QTc prolongation from hypokalemia is worsened by drugs that prolong the QT interval (though fluoxetine's QT effects are modest)
- Avoid bupropion — associated with a significantly increased risk of seizures in patients who purge; contraindicated in active BN
- Other SSRIs (sertraline, citalopram) show efficacy in smaller trials but lack FDA approval for BN
- Topiramate (an anticonvulsant) reduces binge/purge frequency in controlled trials but causes cognitive side effects and is not a first-line option
Nutritional Rehabilitation and Medical Stabilization
Unlike anorexia nervosa, hospitalization solely for nutritional rehabilitation is rarely required in BN (most patients are not underweight). However, inpatient or intensive outpatient medical stabilization is indicated when:
- Serum K+ below 3.0 mEq/L despite outpatient supplementation
- QTc prolongation above 450-500 ms
- Hematemesis or Mallory-Weiss tear
- Active suicidality or comorbid substance use requiring monitored detoxification
- Purging frequency so high (multiple times daily) that outpatient structure cannot interrupt the cycle
Nutritional counseling focuses on nutritional rehabilitation (eliminating deficiencies), structured eating (regular mealtimes), and challenge meals (exposure to feared "binge" foods in a controlled setting to reduce their power as triggers).
9. Binge Eating Disorder (BED)
Binge Eating Disorder (BED) was elevated from a research diagnosis to a full DSM-5 eating disorder in 2013, distinguishing it from BN primarily by the absence of regular compensatory behaviors. BED is now recognized as the most prevalent eating disorder in the US general population — lifetime prevalence approximately 3.5% in women and 2.0% in men — exceeding anorexia and bulimia combined.
DSM-5 Criteria for BED
- Recurrent binge eating episodes (same definition as BN: large amount + loss of control)
- Binge episodes associated with 3+ of the following: eating faster than normal; eating until uncomfortably full; eating large amounts when not hungry; eating alone due to embarrassment; feeling disgusted, depressed, or guilty afterward
- Marked distress about binge eating
- Occurring at least once a week for 3 months
- No regular compensatory behaviors (distinguishes from BN)
Key Differences Between BN and BED
BED frequently co-occurs with obesity (though not universally — BED occurs across all weight categories). The psychological core is similar (shame, loss of control, mood-triggered bingeing) but without the compensatory behavior cycle. Treatment approaches differ: BED responds well to CBT-E, DBT, and IPT, but the pharmacological approach differs — lisdexamfetamine (Vyvanse) is the only FDA-approved medication for moderate-to-severe BED (not fluoxetine), and weight loss approaches that are contraindicated in BN (caloric restriction, behavioral weight loss programs) may be cautiously integrated in BED treatment planning alongside eating disorder therapy.
10. Prognosis and Recovery
Bulimia nervosa has a better prognosis than anorexia nervosa but remains a serious illness with significant chronicity. At 10-year follow-up, approximately 50-70% of patients achieve full recovery. However, 30-40% experience a chronic or relapsing course. Partial recovery (reduced frequency but not full remission) is common.
Mortality rate in BN is approximately 2-3% per decade (compared to 5-10% per decade in anorexia nervosa). Causes of death include cardiac arrhythmia (from electrolyte disturbances) and suicide — suicide risk is 10-fold elevated relative to the general population in BN. Comorbid substance use disorder and borderline personality disorder significantly worsen prognosis.
Positive prognostic factors: shorter illness duration before treatment, absence of comorbid personality disorder or substance use, higher social support, and engagement with structured CBT-E. Negative prognostic factors: early onset, longer duration before treatment, severe compensatory behavior frequency, comorbid impulsivity, and weight/shape overvaluation severity.
The concept of "full recovery" in eating disorders research requires absence of all diagnostic criteria plus functioning at a level comparable to healthy controls — a high bar. Many patients achieve symptomatic remission while retaining residual body image concerns. Ongoing engagement with recovery supports (therapy, peer support groups, ongoing monitoring) improves long-term outcomes.
11. Recent Research and Advances
Gut Microbiome and Eating Disorders
Emerging research suggests the gut-brain axis may be dysregulated in bulimia nervosa. Studies have identified alterations in gut microbiome composition in BN patients compared to healthy controls, with potential effects on serotonin synthesis (90% of the body's serotonin is produced in the gut) and appetite signaling. Whether microbiome changes precede or follow illness onset remains unclear.
Neuromodulation Approaches
Transcranial magnetic stimulation (TMS) targeting the dorsolateral prefrontal cortex has shown preliminary efficacy in small trials, reducing binge frequency and improving impulse control. Deep brain stimulation (DBS) of the nucleus accumbens is under investigation for treatment-refractory cases. These approaches remain experimental but offer hope for patients who have not responded to established treatments.
Digital and App-Based CBT-E
Technology-delivered CBT-E via smartphone apps and therapist-guided online platforms achieves outcomes comparable to face-to-face therapy in moderate-severity BN, with dramatically lower barriers to access. Apps like Recovery Record and platform-based programs have demonstrated RCT-level evidence, addressing the critical shortage of trained eating disorder specialists globally.
Ketamine and Novel Pharmacology
Given the overlap between BN and OCD/anxiety spectrum disorders, low-dose ketamine infusions are under investigation for treatment-refractory BN. GLP-1 receptor agonists (semaglutide, liraglutide), which reduce appetite and binge eating in BED, are being cautiously studied in BN populations, though weight loss effects require careful management in this population.
12. References & Research
- Fairburn CG, Cooper Z, Doll HA, O'Connor ME, Bohn K, Hawker DM, Wales JA, Murphy R. Transdiagnostic cognitive-behavioral therapy for patients with eating disorders: a two-site trial with 60-week follow-up. Am J Psychiatry. 2009;166(3):311-319. PMID: 19074978
- Shapiro JR, Berkman ND, Brownley KA, Sedway JA, Lohr KN, Bulik CM. Bulimia nervosa treatment: a systematic review of randomized controlled trials. Int J Eat Disord. 2007;40(4):321-336 — Search PubMed
- Flament MF, Bissada H, Spettigue W. Evidence-based pharmacotherapy of eating disorders. Int J Neuropsychopharmacol. 2012;15(2):189-207. PMID: 21414249
- Slade E, Keeney E, Mavranezouli I, Dias S, Fou L, Stockton S, Saxon L, Waller G, Turner H, Creed C, Hodsoll J, Bhattacharya R, Bhattacharya S, Maclachlan H, Welton NJ. Treatments for bulimia nervosa: a network meta-analysis. Psychol Med. 2018;48(16):2629-2636 — Search PubMed
- Kaye WH, Fudge JL, Paulus M. New insights into symptoms and neurocircuit function of anorexia nervosa. Nat Rev Neurosci. 2009;10(8):573-584. PMID: 19603056
- Steiger H, Gauvin L, Israel M, Kin NY, Koerner N, Paris J, Young SN. Association of serotonin and cortisol indices with childhood abuse in bulimia nervosa. Arch Gen Psychiatry. 2001;58(9):837-843 — Search PubMed
- Smink FR, van Hoeken D, Hoek HW. Epidemiology of eating disorders: incidence, prevalence and mortality rates. Curr Psychiatry Rep. 2012;14(4):406-414. PMID: 22644309
- Treasure J, Claudino AM, Zucker N. Eating disorders. Lancet. 2010;375(9714):583-593 — Search PubMed
- Walsh BT, Sysko R. Broad categories for the diagnosis of eating disorders (BCD-ED): an alternative system for classification. Int J Eat Disord. 2009;42(8):754-764 — Search PubMed
- Wolfe BE, Jimerson DC, Orlova C, Mantzoros CS. Effect of dieting on plasma leptin, soluble leptin receptor, adiponectin and resistin levels in healthy volunteers. Clin Endocrinol (Oxf). 2004;61(3):332-338 — Search PubMed
- Crow SJ, Peterson CB, Swanson SA, Raymond NC, Specker S, Eckert ED, Mitchell JE. Increased mortality in bulimia nervosa and other eating disorders. Am J Psychiatry. 2009;166(12):1342-1346 — Search PubMed
- Russell G. Bulimia nervosa: an ominous variant of anorexia nervosa. Psychol Med. 1979;9(3):429-448. PMID: 482466
Connections
- Psychiatry
- Anorexia Nervosa
- Eating Disorders Overview
- Anxiety Disorders
- Major Depressive Disorder
- Borderline Personality Disorder
- OCD
- Addiction
- Potassium
- Magnesium
- Lab Tests: Electrolytes
- All Conditions