Cutaneous and Mucosal Leishmaniasis: Skin Ulcers and Tissue Destruction
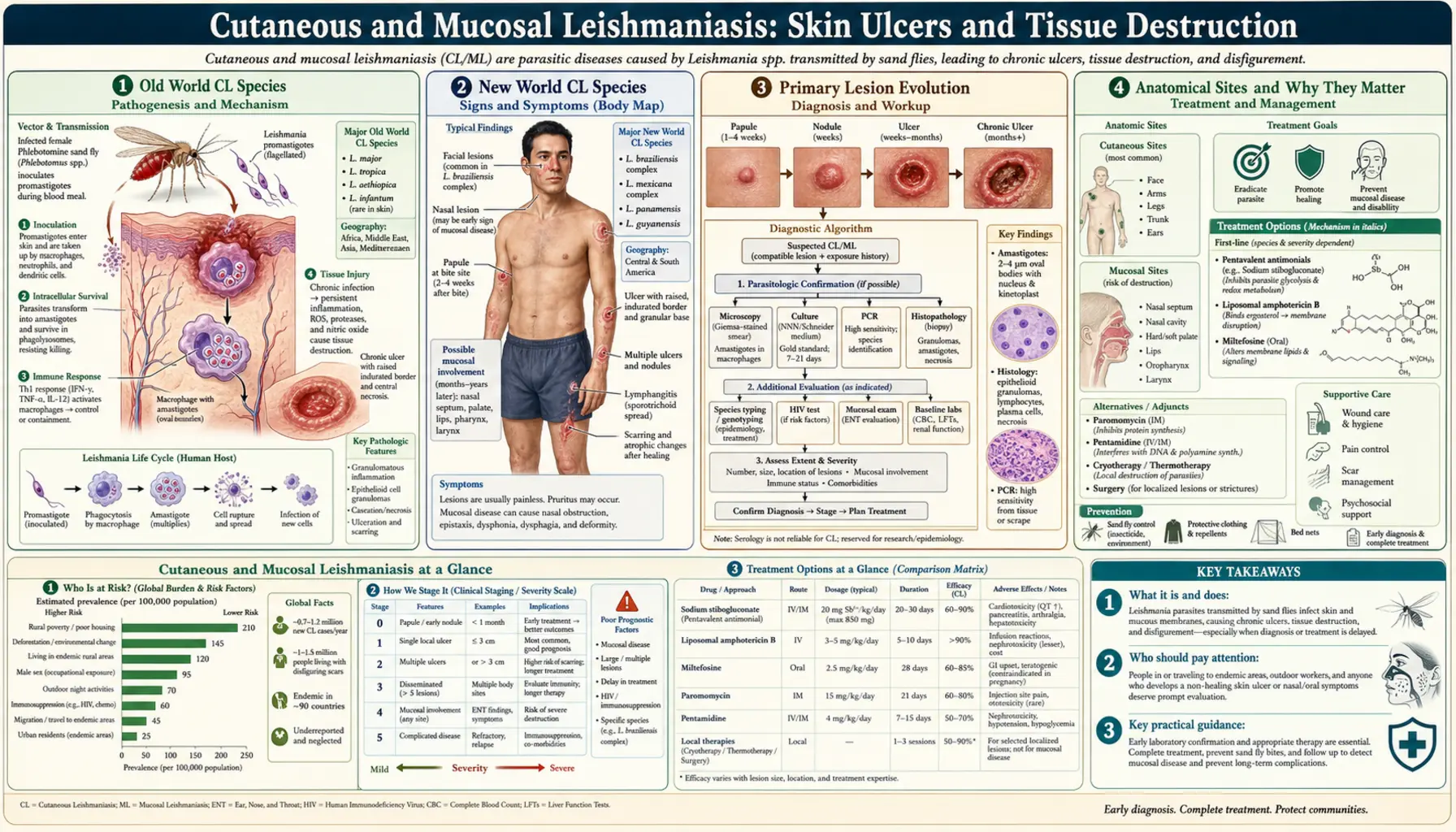
Cutaneous leishmaniasis (CL) is the most common form of the disease, producing characteristic painless ulcers at sandfly bite sites on exposed skin. Mucocutaneous leishmaniasis (MCL), called espundia, is a destructive late complication in which parasites — almost always L. braziliensis in Latin America — migrate from skin to the mucous membranes of the nose, mouth, and throat, causing relentless tissue destruction that never heals spontaneously.
Table of Contents
- Old World CL Species
- New World CL Species
- Primary Lesion Evolution
- Anatomical Sites and Why They Matter
- Natural Course and Scarring
- Secondary Bacterial Infection
- Mucocutaneous Leishmaniasis: Espundia
- Diffuse Cutaneous and Leishmania Recidivans
- Key Research Papers
- Featured Videos
1. Old World CL Species
Old World cutaneous leishmaniasis occurs in southern Europe, the Middle East, Central Asia, South Asia, and Sub-Saharan Africa, transmitted by Phlebotomus sandflies. Three main species account for most Old World CL:
Leishmania major causes the "rural" or "wet sore" form of CL predominant in the deserts and steppes of the Middle East, Central Asia (Kazakhstan, Uzbekistan, Turkmenistan), the Indian subcontinent, and Sub-Saharan Africa. Its natural reservoir is the great gerbil (Rhombomys opimus) and other burrowing rodents. Human infection is zoonotic — humans are incidental hosts when they enter the rodent habitat for agriculture or military operations. L. major lesions are typically "wet," with significant exudation and crust formation, and tend to self-heal within 3–6 months in immunocompetent patients, leaving permanent depressed scars.
Leishmania tropica causes the "urban" or "dry sore" form, also called "oriental sore." It is primarily anthroponotic — humans are the main reservoir. It is endemic in cities and towns across Afghanistan, Iran, Iraq, Pakistan, Turkey, India, and the Mediterranean fringe. L. tropica lesions are "dry," with less exudation, and heal more slowly: 1–3 years is typical, and some cases persist for 5 or more years. This species is also associated with a relapsing form called leishmaniasis recidivans (see below).
Leishmania aethiopica is restricted to the Ethiopian and Kenyan highlands where its reservoir is the rock hyrax (Procavia capensis and related species). It causes a spectrum of disease ranging from classical self-healing CL to diffuse cutaneous leishmaniasis (DCL) in patients with specific immune defects. L. aethiopica does not carry mucocutaneous risk but its diffuse form is extremely difficult to treat.
2. New World CL Species
New World cutaneous leishmaniasis is transmitted by Lutzomyia sandflies across Latin America from Mexico through Argentina. The diversity of species is far greater than in the Old World, and several have clinically important differences:
Leishmania braziliensis (subgenus Viannia) is the most clinically important New World species because 1–5% of cutaneous infections progress to mucocutaneous leishmaniasis months to years after the initial skin ulcer. It is endemic throughout Central and South America, particularly in Brazil, Bolivia, Peru, and Venezuela, and is associated with forest and agricultural occupational exposure. Identifying L. braziliensis by PCR species typing in a CL patient has immediate therapeutic implications: systemic treatment is indicated even for apparently mild localized disease, precisely to prevent MCL progression.
Leishmania mexicana (subgenus Leishmania) causes "chiclero's ulcer" or "bay sore" in Mexico, Central America, and adjacent South America. It was historically common among workers who harvested chicle (chewing gum base) from jungle trees. It typically causes painless single ulcers on the ear pinna (auricular CL) that are notoriously slow to heal — the pinna's poor blood supply slows healing and impairs drug delivery. L. mexicana does not cause MCL.
Leishmania guyanensis causes "pian bois" (forest yaws) in the Amazon basin and Guiana Shield (Guyana, Suriname, French Guiana, northern Brazil). It is distinctive in often producing multiple lesions along the lymphatics draining the primary site — a sporotrichoid pattern. L. guyanensis has intrinsic resistance to meglumine antimoniate (Glucantime) in some endemic areas, so treatment response must be monitored carefully.
Leishmania peruviana causes "uta" in the high dry valleys of the Andes in Peru and Argentina at elevations above 900 m. Its reservoir is the domestic dog. Uta lesions are typically small, single, and self-healing, resembling Old World L. major disease more than other New World forms.
3. Primary Lesion Evolution
The natural history of a cutaneous leishmaniasis lesion follows a predictable sequence, though the pace and ultimate appearance vary by species. Understanding this timeline helps clinicians distinguish CL from other tropical skin diseases and know when to intervene.
The first sign is a small, firm, non-tender papule appearing at the bite site 1–4 weeks after the sandfly feed. At this stage it may resemble an insect bite reaction or a small furuncle, and most patients — and even many clinicians in non-endemic areas — pay it little attention. Over the following 2–4 weeks the papule enlarges and becomes a nodule, often reaching 1–2 cm in diameter with a firm, indurated base. The overlying skin takes on a dark pink or violaceous hue.
The central portion of the nodule then begins to break down: the epidermis erodes and the center undergoes necrosis and ulceration. The result is the classic CL ulcer: a "punched-out" or "volcano crater" appearance with a central concave area and a raised, firm, indurated wall. The base of the ulcer may be clean and granulating (especially in early disease), crusted, or covered with a dried seropurulent exudate. Most CL ulcers are painless or only mildly tender — the painlessness despite significant tissue destruction is a diagnostically useful feature. Satellite papules may develop at the lesion periphery, and regional draining lymph nodes frequently enlarge.
Lesions may reach 3–5 cm in diameter and remain stable for months before either slowly healing (Old World species) or persisting indefinitely (immunocompromised patients, certain species). The entire ulcerative phase can last from 3 months to several years depending on species and host factors. Eventually, the ulcer base granulates and re-epithelializes from the margins inward, leaving a permanent, often sunken scar — the stigmata of leishmaniasis that can last a lifetime.
4. Anatomical Sites and Why They Matter
An extremely useful clinical clue in diagnosing CL is the strict limitation of lesions to exposed skin surfaces. Sandflies are too small and weak to bite through ordinary clothing; they can only feed where skin is uncovered. Lesions therefore occur exclusively on the face, ears, neck, forearms, dorsum of the hands, lower legs, and feet — the areas exposed when wearing normal attire in endemic regions.
The face — particularly the cheeks, nose, and forehead — is the most consequential site. Facial CL lesions cause the most severe disfigurement and the greatest psychosocial burden, particularly for women and girls in cultures where facial appearance is central to social and marital prospects. The psychological impact of a large, crusted, ulcerating facial lesion in a teenage girl in rural Afghanistan or Morocco is profound and often lasting long after the skin heals.
The auricular pinna (ear cartilage) is a site of particular clinical importance because L. mexicana preferentially ulcerates the ear, and the poor vascular supply of cartilaginous tissue both slows natural healing and impairs systemic drug delivery to the lesion. Auricular CL lesions may take years to heal spontaneously and respond slowly to treatment. Untreated cases can result in cartilage destruction and permanent deformity of the ear.
The distribution of lesions also provides epidemiological information. Multiple lesions on the lower legs and feet suggest transmission in a setting where people walk barefoot or wear sandals in endemic areas. Lesions on forearms and hands point to agricultural occupational exposure. A single facial lesion in a returned traveler is the most common presentation in non-endemic countries.
5. Natural Course and Scarring
The natural history of cutaneous leishmaniasis without treatment depends predominantly on the infecting species and the patient's immune status. Most Old World CL caused by L. major in immunocompetent people heals spontaneously within 3–6 months, leaving a permanent scar. This tendency to self-heal reflects the development of a robust Th1 immune response (cellular immunity) that activates macrophages to kill intracellular parasites. Once healed, immunity to L. major reinfection is typically lifelong — a phenomenon called "leishmanization" that was historically exploited in some Middle Eastern countries by deliberate inoculation with L. major to provide protected scarring on a cosmetically inconspicuous body site before natural infection could scar the face.
Leishmania tropica lesions heal more slowly (1–3 years) and leave deeper, more hypertrophic scars. L. braziliensis and other New World species generally heal more slowly than Old World CL. In all cases, healing does not mean the parasite is eradicated — Leishmania amastigotes can persist for years in scar tissue in small numbers, maintaining immune stimulation that may also account for long-term immunity but also carrying the theoretical risk of reactivation if immunosuppression occurs decades later.
For patients who are immunocompromised — from HIV infection, organ transplant immunosuppression, malnutrition, or inherited immune defects — CL does not self-heal. Lesions may continue to enlarge, multiple new lesions may appear (disseminated CL), or the disease may take the non-healing diffuse form. Immunocompromised patients require systemic antileishmanial treatment regardless of the species.
6. Secondary Bacterial Infection
Open CL ulcers are highly susceptible to secondary bacterial infection, particularly in tropical environments with high ambient temperatures, humidity, and dust. The warm, moist, protein-rich wound environment is an ideal bacterial culture medium, and the patient's use of traditional plant-based remedies — common in endemic rural areas — may introduce additional organisms.
Secondary bacterial infection can dramatically alter the clinical appearance of a CL ulcer, covering it with purulent exudate, surrounding it with cellulitis, causing regional lymphangitis, and producing a painful lesion (CL ulcers themselves are painless — pain almost always signals secondary bacterial infection or unusual species). This transformation makes CL resemble a pyogenic tropical ulcer, furuncle, or even anthrax. In settings where microscopy and PCR are unavailable, secondary-infected CL lesions are routinely misdiagnosed and treated with antibiotics alone, delaying specific antileishmanial therapy by months.
Secondary bacterial organisms commonly include Staphylococcus aureus, beta-hemolytic streptococci, and gram-negative enteric organisms. In patients who have applied traditional remedies, environmental molds and other organisms may also colonize. Empirical antibacterial treatment of the secondary infection should accompany (not replace) antileishmanial therapy when both are present. Wound debridement and regular dressing changes improve healing and reduce the bacterial load in the ulcer.
7. Mucocutaneous Leishmaniasis: Espundia
Mucocutaneous leishmaniasis (MCL), known in Latin America as espundia, is the most disfiguring complication of leishmaniasis short of fatal kala-azar. It is caused almost exclusively by Leishmania braziliensis and related species of the Viannia subgenus. MCL occurs when parasites escape from the primary skin ulcer and spread hematogenously or via lymphatics to the nasopharyngeal mucosa — a sanctuary that, for reasons not yet fully understood, proves particularly hospitable to L. braziliensis.
The timing of MCL onset is one of its most treacherous features. The primary cutaneous lesion may have healed months to years — sometimes a decade — before MCL manifests. Patients and physicians may have entirely forgotten the original skin ulcer. The first symptoms are benign-sounding: persistent nasal stuffiness, a runny nose, nosebleeds. These are easily attributed to allergies, sinusitis, or a common cold.
Without treatment, the destruction progresses relentlessly. The nasal septum — made of cartilage that lacks the bone's capacity for regeneration — perforates and collapses. The cartilaginous framework of the nose loses its support and the nose flattens forward and downward, merging with the upper lip in the characteristic "tapir nose" or "tapir mouth" deformity. The infection spreads to the hard and soft palate, producing erosions that may perforate the palate and allow communication between the oral and nasal cavities. The tonsillar pillars, uvula, pharynx, and larynx can all be involved. Laryngeal destruction causes hoarseness, dysphagia, and eventually threatens the airway with life-threatening obstruction.
Psychologically and socially, MCL is devastating. Patients lose the ability to eat solid food, to speak clearly, and to interact socially without stigma. In rural South American communities, MCL carries severe social consequences including abandonment, unemployment, and social exclusion. Treatment with systemic antileishmanials stops progression but cannot restore destroyed tissue. Reconstructive surgery may be required to rebuild nasal passages and airways after the infection is controlled.
The risk factors for MCL progression from primary CL include: infection with L. braziliensis (most important), delay in treatment of CL (longer CL → more risk of mucosal seeding), multiple or large CL lesions, immunosuppression, and male sex (men have higher rates than women, possibly from higher occupational forest exposure and delayed treatment-seeking). The precise immunological mechanism of mucosal tropism is not fully understood; both parasite factors and a maladaptive immune response (excessive inflammatory response that damages tissue while failing to clear parasites) appear to contribute.
8. Diffuse Cutaneous and Leishmania Recidivans
Diffuse cutaneous leishmaniasis (DCL) is a rare but severe form occurring in patients with specific immune defects, particularly anergy (inability to mount a delayed-type hypersensitivity response to Leishmania antigens). It is most commonly caused by L. aethiopica in Africa or L. amazonensis and L. mexicana in Latin America. In DCL, the immune system fails to limit the infection to the bite site; instead, parasites disseminate through the skin, producing hundreds of non-ulcerating nodules covering the face, ears, trunk, and extremities. The lesions are teeming with parasites (unlike classic CL, which has few parasites per high-power field). DCL is extremely difficult to treat, as the poor cell-mediated immune response means drugs that work by activating macrophages are less effective. Treatment with liposomal amphotericin B may achieve partial response, but relapse is common.
Leishmania recidivans (also called lupoid leishmaniasis) is a chronic relapsing form caused primarily by L. tropica. The primary CL ulcer heals in the center while new papules develop at its margin, slowly migrating outward over years or decades. The central scar appears healed while the active border continues to expand. Biopsies of the active margin show few parasites, and the lesion pattern resembles lupus vulgaris (cutaneous tuberculosis) histologically. The Montenegro skin test (a delayed-type hypersensitivity test to Leishmania antigen) is strongly positive, indicating that the patient has a Th1 immune response to the parasite but cannot fully clear it from the skin. Leishmania recidivans may persist for 20 or more years without treatment, causing progressively expanding facial scarring.
Key Research Papers
Peer-reviewed studies on cutaneous and mucocutaneous leishmaniasis pathogenesis, clinical features, and outcomes. PMID links open the abstract on PubMed.
- Chappuis F, et al. Visceral Leishmaniasis: What Are the Needs for Diagnosis, Treatment and Control? Nat Rev Microbiol. 2007. — Search PubMed
- Alvar J, et al. Leishmaniasis Worldwide and Global Estimates of Its Incidence. PLoS ONE. 2012. — Search PubMed
- Reithinger R, et al. Cutaneous Leishmaniasis. Lancet Infect Dis. 2007. — Search PubMed
- Bern C. Visceral Leishmaniasis. N Engl J Med. 2015. — Search PubMed
- Schriefer A, et al. Mucosal Leishmaniasis: Epidemiology, Clinical Presentation, and Treatment Outcomes. Clin Infect Dis. 2009. — Search PubMed
- van Griensven J, Diro E. Visceral Leishmaniasis. Infect Dis Clin North Am. 2019. — Search PubMed
- Sundar S, Singh A. Recent Developments in the Treatment of Visceral Leishmaniasis. Ther Adv Infect Dis. 2016. — Search PubMed
- Monge-Maillo B, Lopez-Velez R. Therapeutic Options for Visceral Leishmaniasis. Drugs. 2013. — Search PubMed
- Bhatt S, et al. The global distribution and burden of leishmaniasis. Lancet. 2019. — Search PubMed
- Marsden PD. Mucosal leishmaniasis ("espundia" Escomel, 1911). Trans R Soc Trop Med Hyg. 1986. — Search PubMed
Live PubMed Searches
- Cutaneous leishmaniasis L. major ulcer
- L. braziliensis mucocutaneous disease
- Espundia mucosal leishmaniasis
- Diffuse cutaneous leishmaniasis
- L. tropica urban oriental sore
- Leishmaniasis recidivans lupoid
Connections
- All Parasites
- Leishmania Overview
- Leishmania: Symptoms Hub
- Visceral Leishmaniasis (Kala-Azar)
- Diagnosis: Microscopy & PCR
- Treatments Hub
- Miltefosine & Antimonials
- Prevention & Vector Control
- Dermatology
- Infectious Disease
- All Conditions
- Leishmaniasis — the disease overview covering all three clinical forms, global burden, and treatment.