Liposomal Amphotericin B for Visceral Leishmaniasis: WHO First-Line Therapy
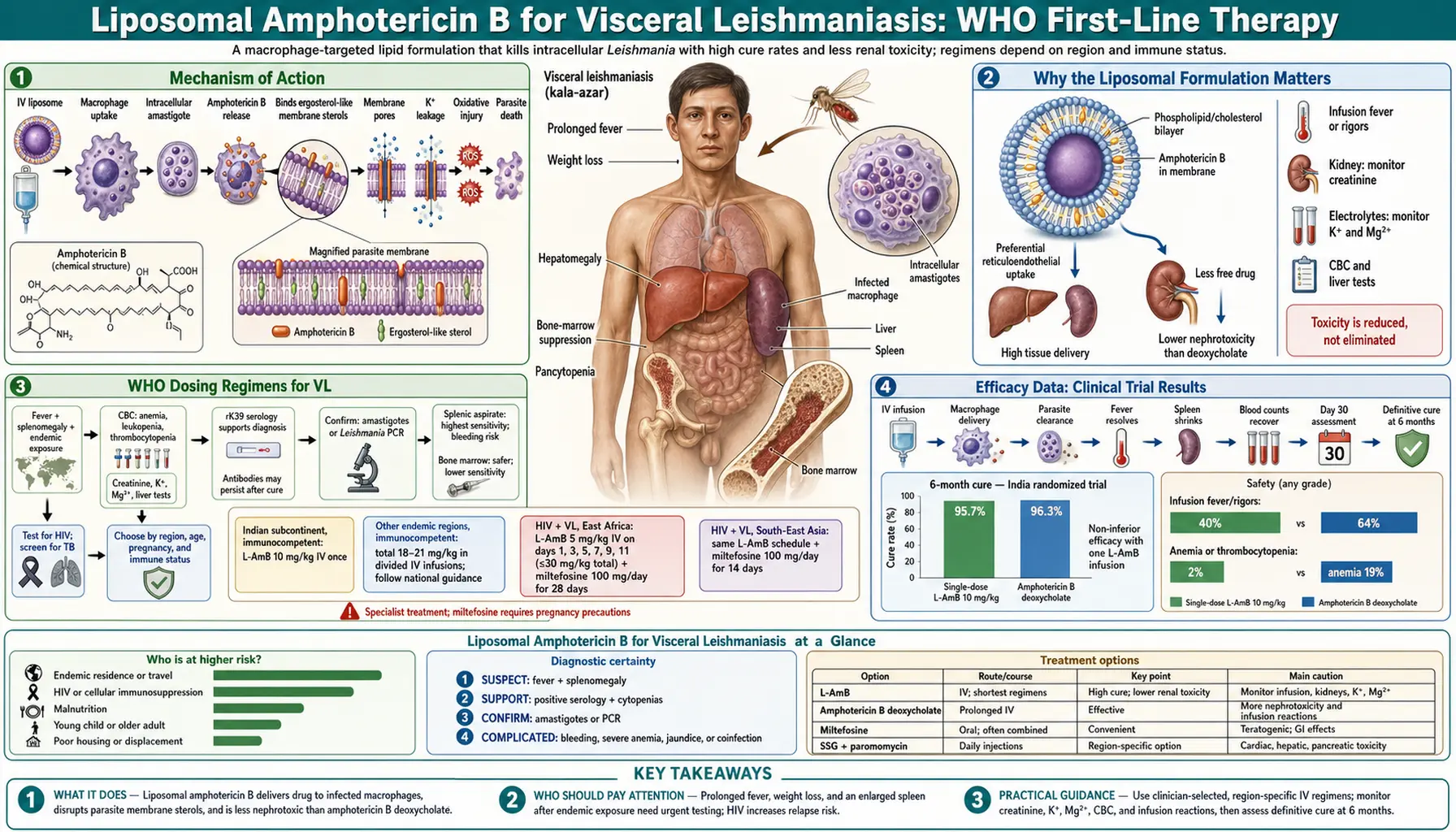
Liposomal amphotericin B (AmBisome) is the WHO-preferred first-line treatment for visceral leishmaniasis in South Asia, the Mediterranean basin, and Europe. It achieves cure rates of 95–99% in Indian VL with a single infusion, dramatically cutting treatment duration from the month-long courses previously required. The liposomal formulation was a breakthrough not just in efficacy but in tolerability: by encapsulating the antifungal drug amphotericin B inside phospholipid vesicles, it delivers the drug preferentially to macrophages — exactly where Leishmania lives — while drastically reducing the kidney damage that plagued the older conventional formulation.
Table of Contents
- Mechanism of Action
- Why the Liposomal Formulation Matters
- WHO Dosing Regimens for VL
- Efficacy Data: Clinical Trial Results
- Nephrotoxicity: Comparison with Conventional AmphoB
- Infusion-Related Reactions and Premedication
- Monitoring During Treatment
- Use in HIV Co-infected Patients
- Pregnancy and Pediatric Use
- Use in Cutaneous and Mucocutaneous Leishmaniasis
- Key Research Papers
- Connections
- Featured Videos
1. Mechanism of Action
Amphotericin B kills Leishmania parasites by targeting ergosterol, the primary sterol in the Leishmania cell membrane. This is the same mechanism by which the drug kills fungi — both fungi and Leishmania protozoa use ergosterol as their primary membrane sterol, unlike mammalian cells, which use cholesterol. This biochemical difference is the pharmacological basis for selectivity: amphotericin B binds ergosterol with high affinity and forms pores in the membrane, disrupting its integrity and allowing ions to leak out, ultimately causing cell death.
The ergosterol selectivity is not absolute — amphotericin B also binds, with lower affinity, to cholesterol in mammalian cell membranes. This non-selective binding is responsible for the drug's toxicity, particularly the kidney toxicity (nephrotoxicity) that was the major limitation of conventional amphotericin B deoxycholate formulations. The liposomal formulation fundamentally changes the biodistribution of the drug, dramatically reducing the exposure of renal tubular cells while maintaining high drug delivery to macrophages.
Once inside a macrophage, liposomal particles are taken up by lysosomes, which release the amphotericin B in close proximity to the Leishmania amastigotes living within the phagolysosome. This targeted delivery is not simply a pharmacokinetic convenience — it concentrates the drug at exactly the site where the parasite resides, maximizing efficacy while limiting systemic exposure.
2. Why the Liposomal Formulation Matters
Conventional amphotericin B deoxycholate (AmB-d) — the original formulation — was effective against VL but caused such severe nephrotoxicity (acute kidney injury in 30–40% of patients), infusion-related reactions, and electrolyte disturbances (particularly hypokalemia and hypomagnesemia) that it required hospitalization, daily laboratory monitoring, and careful dose management. It was also typically administered over 30 days, making it logistically burdensome for health systems in endemic regions.
The liposomal formulation (AmBisome, developed in the 1990s) encapsulates amphotericin B inside unilamellar liposomes — small spherical vesicles made of phospholipids. These liposomes preferentially accumulate in reticuloendothelial system (RES) tissues — the spleen, liver, and bone marrow — which are precisely the organs where Leishmania parasites are most abundant in VL. This preferential targeting achieves two goals simultaneously: higher drug concentrations where the parasite lives, and lower drug concentrations in the kidney, where conventional AmphoB causes damage.
The practical result is dramatic: nephrotoxicity rates fall from 30–40% with conventional AmphoB to under 5% with liposomal AmphoB, infusion-related reactions become milder and less frequent, and treatment can be completed in days rather than weeks. A 2010 landmark trial demonstrated that a single dose of liposomal AmphoB (10 mg/kg) achieved a 95.7% cure rate in Indian VL — a result that would have been unimaginable with the conventional formulation.
3. WHO Dosing Regimens for VL
WHO 2010 guidelines and subsequent updates recommend liposomal amphotericin B as first-line therapy for VL in South Asia, with two main regimen options depending on healthcare system capacity and clinical context:
Regimen A — Single dose (South Asia preferred):
- 10 mg/kg IV as a single infusion over 2–4 hours
- Highly effective in Indian subcontinent VL: 95.7% initial cure in pivotal trial
- Dramatically simplifies logistics: one hospital visit, one dose, one infusion
- Recommended by WHO for India, Nepal, Bangladesh where L. donovani sensitivity is confirmed
- Less effective in East Africa and Mediterranean where species differ (>90% but not equivalent to Indian data)
Regimen B — Multi-dose (widely applicable):
- 3 mg/kg/day IV on days 1, 2, 3, 4, 5, and then day 10 (total 18 mg/kg over 10 days)
- Allows dose-splitting to reduce infusion burden per session
- Used in Mediterranean, East Africa, and for HIV co-infected patients
- Efficacy 90–98% in immunocompetent VL patients across regions
HIV co-infection regimen (higher total dose):
- 4 mg/kg/day IV on days 1–5, 10, 17, 24, 31, and 38 (total 40 mg/kg)
- Higher total dose reflects lower cure rates in immunosuppressed patients and higher relapse risk
- Followed by monthly secondary prophylaxis: 3–5 mg/kg IV every 4 weeks until CD4 >200 cells/μL
Combination regimens (South Asia — increasingly preferred):
- Liposomal AmphoB single dose 5 mg/kg + miltefosine 7 days: 97.5% initial cure; simplifies treatment course
- Liposomal AmphoB single dose 5 mg/kg + paromomycin 10 days IM: 95%+ efficacy; no oral drug compliance issue
- Combination rationale: lower dose of each drug, shorter course, reduces resistance selection pressure
4. Efficacy Data: Clinical Trial Results
The efficacy of liposomal amphotericin B for VL is among the best-documented of any drug in tropical medicine, supported by multiple randomized controlled trials across different regions and species.
Key trial results:
- Sundar et al. 2010 (NEJM) — Single-dose trial, India: 304 patients with confirmed VL in Bihar randomized to single-dose liposomal AmphoB 10 mg/kg vs. conventional AmphoB deoxycholate 1 mg/kg × 20 days; definitive cure at 6 months: 95.7% (liposomal) vs. 95.8% (conventional); liposomal arm: 0 nephrotoxicity-related discontinuations vs. 2 in conventional; dramatically simpler administration — Search PubMed
- East Africa multi-centre trial (LEAP 2011): liposomal AmphoB 30 mg/kg total over 21 days vs. SSG+paromomycin; liposomal arm 85% initial cure vs. 91% for combination; lower in East Africa than India, confirming species-dependent efficacy differences
- Mediterranean pediatric VL: liposomal AmphoB 3 mg/kg/day × 5 days then day 10 (total 18 mg/kg) achieves 97–100% cure in immunocompetent children with L. infantum VL; standard of care in European pediatric centers
- HIV/VL co-infection: cure rates 70–85% for initial treatment; relapse rates without secondary prophylaxis 60–80% at 12 months; secondary prophylaxis reduces relapse to 20–30%
The consistency of >95% cure rates across multiple independent trials in South Asia is exceptional and places liposomal AmphoB among the most effective drugs in clinical medicine for any parasitic disease.
5. Nephrotoxicity: Comparison with Conventional AmphoB
The nephrotoxicity of amphotericin B was the major obstacle to its widespread use in VL for decades. Conventional AmphoB deoxycholate causes kidney injury through two mechanisms: direct tubular toxicity (causing tubular dysfunction, potassium and magnesium wasting, and renal tubular acidosis) and vasoconstriction of renal afferent arterioles (reducing glomerular filtration rate). Nephrotoxicity was so predictable with conventional AmphoB that it was essentially expected — the question was not whether the kidneys would be affected but how severely.
Nephrotoxicity comparison:
- Conventional AmphoB deoxycholate: acute kidney injury (creatinine rise >2× baseline or rise >0.5 mg/dL) in 30–40% of patients; permanent renal damage less common but documented; hypokalemia requiring supplementation in 50–70%
- Liposomal AmphoB (AmBisome): clinically significant nephrotoxicity in <5% of patients; hypokalemia less frequent and usually mild; rarely requires discontinuation for renal reasons
- Mechanism of difference: liposomes are not filtered by the kidney glomerulus and do not concentrate in renal tubular cells; the drug reaches macrophages (liver, spleen, bone marrow) before being cleared by the RES, minimizing renal exposure
In practical terms: a patient receiving conventional AmphoB required daily creatinine and electrolyte monitoring and was at significant risk of needing dose reduction or cessation. A patient receiving liposomal AmphoB still requires baseline and end-of-treatment labs, but the risk of treatment-limiting nephrotoxicity is low enough that it rarely changes clinical management.
6. Infusion-Related Reactions and Premedication
Despite the superior tolerability of liposomal AmphoB compared with conventional formulations, infusion-related reactions (IRR) remain a clinical reality that requires proactive management. IRRs are most common with the first two to three infusions and diminish in frequency and severity with subsequent doses as patients appear to develop tolerance.
Clinical features of IRR:
- Typically begin 30–45 minutes into the infusion (occasionally at infusion end)
- Fever and rigors (chills) — the most common manifestation; can be severe
- Hypotension — usually mild and responsive to slowing the infusion rate and IV fluid bolus
- Nausea and vomiting
- Headache, myalgia, and flushing
- Rarely: bronchospasm or more severe anaphylactoid reactions
Standard premedication protocol:
- Paracetamol (acetaminophen) 1000 mg orally or IV 30 minutes before infusion
- Diphenhydramine (Benadryl) 25–50 mg IV 30 minutes before infusion
- Some centers also add hydrocortisone 50–100 mg IV before the first one or two doses
- Meperidine (pethidine) 25–50 mg IV can abort rigors if they occur during infusion
Infusion rate management:
- Standard infusion over 2 hours; slowing to 4 hours reduces IRR frequency and severity
- If a mild IRR occurs, slow the infusion rate, administer diphenhydramine, and reassess; do not stop unless hemodynamically unstable
- If hypotension occurs: stop infusion temporarily, administer IV normal saline bolus 250–500 mL, monitor vital signs, restart at half the infusion rate when hemodynamically stable
- Severe anaphylactoid reactions: stop infusion, epinephrine 0.5 mg IM, airway management per protocol; permanent discontinuation warranted
7. Monitoring During Treatment
Despite the improved safety profile of liposomal AmphoB, appropriate laboratory monitoring during treatment is standard practice. The frequency and scope of monitoring are less intensive than for conventional AmphoB but should not be omitted.
Baseline (before first dose):
- Serum creatinine and blood urea nitrogen (renal function baseline)
- Serum electrolytes: sodium, potassium, magnesium (hypokalemia and hypomagnesemia can occur and compound cardiac risk)
- Complete blood count (CBC): platelet count (thrombocytopenia can occur; also reflects disease severity)
- Liver function tests: transaminases, bilirubin (hepatic involvement is common in VL itself)
During multi-dose treatment (days 1–10 regimen):
- Serum creatinine and potassium at day 5 and after last dose
- Vital signs and symptom monitoring with each infusion (for IRR)
- Platelet count at day 5 for patients with severe baseline thrombocytopenia
Single-dose treatment (10 mg/kg):
- Serum creatinine and potassium 24–48 hours post-infusion
- Clinical reassessment at day 30 for fever resolution and spleen size
- Definitive cure assessment at 6 months (clinical: absence of fever, weight gain, spleen regression)
Treatment failure: defined as persistent fever or failure of spleen to decrease in size at day 30. If initial cure is not achieved with liposomal AmphoB, re-treatment with a higher total dose or switch to combination therapy with miltefosine is the typical approach.
8. Use in HIV Co-infected Patients
Visceral leishmaniasis in an HIV-co-infected person is a fundamentally different disease. HIV depletes CD4+ T cells and impairs the interferon-gamma-mediated macrophage activation that is the cornerstone of immune control of Leishmania. The result: higher parasite burdens, atypical presentations (including gastrointestinal involvement, pulmonary disease, and multisystem dissemination not seen in immunocompetent patients), lower cure rates with standard treatment, and near-universal relapse without secondary prophylaxis.
Treatment approach for HIV/VL co-infection:
- Liposomal AmphoB is the preferred drug — antimonials carry greater risk of cardiac toxicity in immunosuppressed patients, and miltefosine alone shows lower efficacy in HIV-positive patients
- Higher total dose required: WHO recommends 4 mg/kg on days 1–5, 10, 17, 24, 31, and 38 (total 40 mg/kg) vs. 18 mg/kg for immunocompetent patients
- Initial cure rates: 70–85% (significantly lower than >95% in immunocompetent patients)
- Concurrent antiretroviral therapy (ART): start or optimize ART as soon as clinically feasible; immune reconstitution is the only sustainable long-term strategy; CD4 rise to >200 cells/μL is required before secondary prophylaxis can be discontinued
Secondary prophylaxis:
- Without secondary prophylaxis, 60–80% of HIV/VL patients relapse within 12 months of initial cure
- WHO-recommended regimen: liposomal AmphoB 3–5 mg/kg IV every 3–4 weeks (monthly)
- Discontinue when CD4 >200 cells/μL on stable ART for at least 6 months, with undetectable viral load
- Renal monitoring at each secondary prophylaxis dose
Immune reconstitution inflammatory syndrome (IRIS) in HIV/VL: as ART restores immune function, a paradoxical worsening of VL symptoms can occur (IRIS). This is clinically important to distinguish from treatment failure. In IRIS, parasitologic cure may already be achieved (negative PCR) while inflammatory symptoms worsen. Management: continue ART, do not re-treat VL without evidence of parasitologic relapse; short course of corticosteroids in severe IRIS.
9. Pregnancy and Pediatric Use
Pregnancy: VL in pregnancy is associated with very high maternal and fetal mortality if untreated — miscarriage rates exceed 80% in untreated VL, and maternal mortality approaches 100% without treatment. This makes the treatment decision clear: untreated VL kills; treatment is necessary. Liposomal AmphoB is the preferred agent in pregnancy because: (1) the conventional alternatives (pentavalent antimonials) are teratogenic and carry cardiac risks; (2) miltefosine is Category D (embryotoxic/teratogenic in animals) and absolutely contraindicated in pregnancy; (3) liposomal AmphoB's teratogenic risk in humans appears low based on case series, though animal data show dose-dependent teratogenicity at very high doses. Published case series of liposomal AmphoB use in pregnancy have documented successful outcomes without major fetal harm when used for VL or invasive fungal infections, but formal controlled data are lacking. The standard dosing regimen is used; monitoring for nephrotoxicity and electrolyte disturbance is maintained.
Pediatric use: liposomal AmphoB is very well-tolerated in children and is the treatment of choice for VL in pediatric patients. The mg/kg doses are the same as for adults. Mediterranean pediatric VL caused by L. infantum (which occurs in children aged 1–5 years predominantly) is successfully treated with the 18 mg/kg multi-dose regimen, with cure rates of 97–100% in clinical series. Infusion rates are adjusted by body weight and infused over 2 hours. IRRs occur in children but are generally well-managed with standard premedication.
10. Use in Cutaneous and Mucocutaneous Leishmaniasis
While liposomal AmphoB is best established for VL, it has an important role in CL and MCL treatment, primarily for disease that is refractory to first-line agents or in patients for whom antimonials and miltefosine are contraindicated.
Cutaneous leishmaniasis: liposomal AmphoB is used for: (1) CL caused by Viannia subgenus species (especially L. braziliensis) that carry mucosal risk and fail antimonial treatment; (2) diffuse CL in immunocompromised patients; (3) CL in patients who cannot receive antimonials (cardiac disease, pancreatitis history) or miltefosine (pregnancy, women without contraception). Standard dosing: 3 mg/kg/day IV × 5–7 days (total 15–21 mg/kg); cure rates for CL are lower than for VL (60–80%) because skin penetration of liposomal particles may be less efficient than macrophage targeting in the RES.
Mucocutaneous leishmaniasis: MCL requires systemic treatment; liposomal AmphoB is increasingly preferred over antimonials given the far better tolerability (avoiding cardiac and pancreatic toxicities of antimonials during long-course treatment) and avoidance of teratogenicity concerns vs. miltefosine in women of childbearing age. WHO recommends liposomal AmphoB for MCL when available: 3 mg/kg/day × 10 days (total 30 mg/kg); cure rates for MCL 70–80%; recurrence monitoring at 6–12 months required as mucosal disease can smolder.
Key Research Papers
Peer-reviewed trials, pharmacology reviews, and clinical guidelines covering liposomal amphotericin B in visceral leishmaniasis across regions and populations. PMID links open the PubMed record.
- Sundar S, Chakravarty J, Agarwal D, et al. Single-dose liposomal amphotericin B for visceral leishmaniasis in India. N Engl J Med. 2010;362(6):504–512 — Search PubMed
- Olliaro PL, Shamsuzzaman TAK, Manica M, et al. Combination treatments for visceral leishmaniasis in East Africa. Lancet Infect Dis. 2015;15(9):1012–1018 — Search PubMed
- Alvar J, Vélez ID, Bern C, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS ONE. 2012;7(5):e35671 — Search PubMed
- Sundar S, Singh A, Rai M, et al. Efficacy of miltefosine in the treatment of visceral leishmaniasis in India after a decade of use. Clin Infect Dis. 2012;55(4):543–550 — Search PubMed
- Dorlo TPC, Balasegaram M, Beijnen JH, de Vries PJ. Miltefosine: a review of its pharmacology and therapeutic efficacy in the treatment of leishmaniasis. J Antimicrob Chemother. 2012;67(11):2576–2597 — Search PubMed
- Sundar S, Sinha PK, Rai M, et al. Comparison of short-course multidrug treatment with standard therapy for visceral leishmaniasis in India. Bull World Health Organ. 2011;89(10):726–734 — Search PubMed
- Mondal D, Hasnain MG, Hossain MS, et al. Study on drug efficacy for visceral leishmaniasis in Bangladesh. Trans R Soc Trop Med Hyg. 2019;113(9):556–564 — Search PubMed
- Musa AM, Mbui J, Khalil EA, et al. Efficacy and safety of liposomal amphotericin B versus miltefosine for treatment of post-kala-azar dermal leishmaniasis in Sudan and India. PLoS Negl Trop Dis. 2019;13(8):e0007673 — Search PubMed
- Chappuis F, Sundar S, Hailu A, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007;5(11 Suppl):S7–S16 — Search PubMed
- Cota GF, de Sousa MR, Fereguetti TO, et al. The cure rate after placebo or no therapy in American cutaneous leishmaniasis. PLoS Negl Trop Dis. 2016;10(2):e0004361 — Search PubMed
Live PubMed Searches
Each link opens a live PubMed query for current literature.
- Liposomal AmphoB VL
- AmBisome single dose kala-azar
- AmphoB ergosterol Leishmania mechanism
- Liposomal AmphoB nephrotoxicity reduction
- VL HIV co-infection treatment
- AmphoB infusion reactions premedication
- MCL amphotericin treatment
- Leishmaniasis pregnancy treatment
Connections
- All Parasites
- Leishmania: Leishmaniasis Overview
- Treatments Hub
- Miltefosine and Antimonials
- Prevention and Vector Control
- Symptoms Hub
- Visceral Leishmaniasis (Kala-Azar)
- Cutaneous & Mucosal Leishmaniasis
- Malaria
- Infectious Disease