Leishmania Prevention: Sandfly Control and Reservoir Management
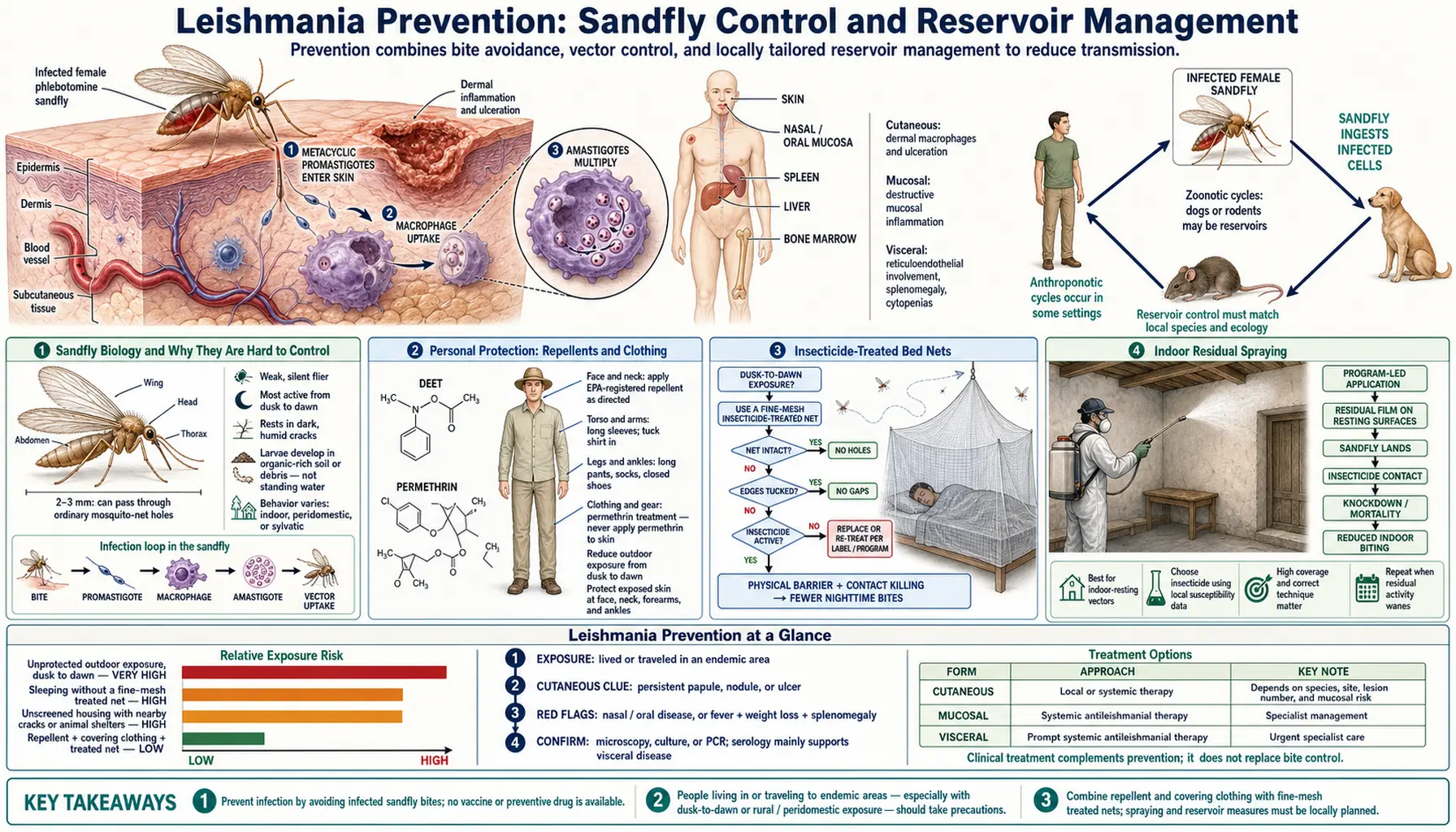
Unlike malaria, there is no licensed human vaccine against leishmaniasis. Prevention therefore rests entirely on avoiding sandfly bites and reducing the sandfly population and its animal reservoirs. Sandflies are significantly harder to control than mosquitoes: they are smaller, silent, and can pass through standard mosquito nets. Effective prevention requires a layered approach — personal protection with repellents and fine-mesh nets, community-level indoor residual spraying, reservoir management targeting the animal hosts that sustain transmission, and in some settings, vaccination of the canine reservoir. The South Asian elimination program, which has achieved dramatic case reductions in India, Nepal, and Bangladesh since 2005, demonstrates that integrated vector control combined with active case detection and treatment can push VL toward elimination.
Table of Contents
- Sandfly Biology and Why They Are Hard to Control
- Personal Protection: Repellents and Clothing
- Insecticide-Treated Bed Nets
- Indoor Residual Spraying
- Environmental and Breeding Site Management
- Reservoir Control: Zoonotic CL (Rodent Reservoirs)
- Canine Reservoir Control and Dog Vaccination
- Human Vaccine Development
- South Asia VL Elimination Program
- Advice for Travelers to Endemic Areas
- Key Research Papers
- Connections
- Featured Videos
1. Sandfly Biology and Why They Are Hard to Control
The vectors of leishmaniasis are small blood-sucking flies in the genus Phlebotomus in the Old World (Europe, Asia, Africa, and the Middle East) and Lutzomyia in the New World (Central and South America). These insects are 2–3 mm in length — roughly one-third the size of a mosquito — and have several biological characteristics that make them substantially more difficult to control than mosquitoes.
Flight and feeding behavior:
- Sandflies fly close to the ground (within 1 meter); elevated sleeping on cots or beds provides some protection because sandflies rarely fly above 1 meter in search of a host
- Active predominantly at dusk, during the night, and at dawn (crepuscular-nocturnal); daytime exposure risk is low except in dense forest environments where canopy shade simulates dusk conditions
- Flight range is very limited: typically 200–300 meters from breeding sites; passive wind dispersal can extend this to 1–2 km; this means vector control measures have a local but not regional effect
- Silent flight: unlike the audible whine of mosquitoes, sandflies approach and bite silently, removing one behavioral warning cue
- Bites are often painless or mildly irritating; patients frequently cannot recall being bitten, even when acquiring significant infections
Breeding ecology:
- Sandfly larvae develop in soil rich in organic matter: leaf litter, compost piles, cracks in mud walls, rubble, animal burrows, grain stores, and peridomestic debris; they do not breed in standing water (unlike mosquitoes), making source reduction strategies different and more diffuse
- Temperature-sensitive: sandflies do not survive at temperatures below approximately 10°C; cold winters eliminate them from parts of their range seasonally; transmission is therefore most intense during warm months (April–October in South Asia, May–September in Mediterranean Europe)
- Humidity-sensitive: they prefer humid microenvironments; air conditioning (by reducing humidity and temperature) strongly deters sandflies indoors
Net mesh size challenge:
- Standard mosquito netting has a mesh aperture of 1.2–1.5 mm; Phlebotomus sandflies are small enough to pass through this mesh freely
- Fine-mesh nets with <0.6 mm aperture are required to physically exclude sandflies; such nets significantly impair airflow in hot climates, making them uncomfortable in tropical conditions without air conditioning
- Permethrin-impregnated standard nets (even with larger aperture) are effective because sandflies that land on the net to find an entry point absorb enough insecticide to be killed before they can bite
2. Personal Protection: Repellents and Clothing
Chemical repellents provide an individual layer of protection but are less effective against sandflies than against mosquitoes. The same active ingredients used for mosquitoes are used against sandflies, but sandflies appear to be less deterred by repellents — requiring more frequent reapplication and higher concentrations.
DEET (N,N-diethyl-meta-toluamide):
- The most widely available repellent globally; effective against sandflies at concentrations of 20–35%
- Less durable protection against sandflies than mosquitoes: mosquito protection from 30% DEET lasts 4–6 hours; sandfly protection may require reapplication every 2–3 hours in high-exposure conditions
- Apply to all exposed skin at dusk and during the night in endemic areas; emphasis on lower legs and ankles (sandflies fly low)
- Safe for children aged ≥2 months at concentrations ≤30%; avoid application around eyes, mouth, or on hands of young children (hand-to-mouth transfer)
Picaridin (icaridin, KBR 3023):
- At 20% concentration, picaridin shows slightly superior efficacy against sandflies compared with equivalent-concentration DEET in controlled field studies
- Better skin feel than DEET (less greasy); safe for children; preferred by many users for cosmetic reasons
- Protection duration comparable to DEET for sandflies; reapply every 2–3 hours in high-risk conditions
Permethrin-treated clothing:
- Permethrin is a synthetic pyrethroid that can be applied to clothing (NOT directly to skin): it kills or stuns insects that contact treated fabric
- Long-sleeved shirts and long trousers treated with permethrin, combined with skin repellent on exposed areas, provide substantially better protection than either measure alone
- Pre-treated clothing (commercially available as "insect shield" fabrics) remains effective through multiple washes; DIY treatment requires reapplication
- Particularly effective when combined with tucking trousers into socks (sandflies are low-fliers and frequently bite ankles and lower legs)
Air conditioning: indoor air conditioning is one of the most effective personal protective measures available: it reduces indoor temperature and humidity below sandfly comfort ranges, and the airflow deters these weak fliers. Residents of air-conditioned bedrooms in endemic areas have significantly lower VL incidence than those in non-air-conditioned dwellings.
3. Insecticide-Treated Bed Nets
Insecticide-treated nets (ITN) and long-lasting insecticidal nets (LLIN) are a cornerstone of vector-borne disease prevention in endemic countries. For sandflies, the insecticide content of the net is more important than the physical mesh size, because standard nets with 1.2–1.5 mm aperture allow sandfly entry but kill them on contact with permethrin or deltamethrin impregnation.
Evidence for ITN effectiveness against VL:
- A landmark cluster-randomized trial in Bihar, India, demonstrated a 50–70% reduction in VL incidence in households using deltamethrin-impregnated bed nets compared with control households; this is among the strongest evidence for any vector control measure against VL
- Net use rates decline in communities not supported by active distribution and follow-up programs; compliance is lower when nets reduce airflow in hot climates
- Long-lasting insecticidal nets (LLIN, eg. PermaNet): release effective insecticide concentrations for 3+ years without re-treatment; preferred over conventionally treated nets for programmatic distribution
Net selection for sandfly prevention:
- Fine-mesh nets (<0.6 mm aperture): physically exclude sandflies without relying on insecticide contact; most effective option when untreated; significant disadvantage is reduced airflow and heat retention in tropical climates; appropriate in cooler highland settings or air-conditioned rooms
- Standard-aperture LLIN (permethrin or deltamethrin): preferred in hot climates; sandfly protection relies on insecticide contact kill; effective even after sandflies pass through mesh if they contact a sufficient area of net surface
- Combination: fine-mesh nets with insecticide impregnation offer maximal protection but maximum heat discomfort
Window and door screens: fine-mesh screens on windows and doors (or non-air-conditioned rooms with standard screens impregnated with insecticide) reduce indoor sandfly density. Sealing cracks and gaps in walls that serve as sandfly resting and breeding sites reduces the peridomestic population.
4. Indoor Residual Spraying
Indoor residual spraying (IRS) involves applying long-lasting insecticides to the interior walls and ceilings of homes, where sandflies rest after blood meals. It is the most powerful community-level vector control intervention currently available against VL vectors.
DDT (dichlorodiphenyltrichloroethane):
- Remains highly effective against Phlebotomus sandflies; residual activity on mud or clay walls of 6–12 months after a single spray cycle
- Banned for agricultural use globally under the 2001 Stockholm Convention on Persistent Organic Pollutants; permitted for malaria and other vector control under strict WHO exemption, but most countries have phased out its use
- The South Asian VL elimination program achieved dramatic early success in part by leveraging existing malaria DDT IRS infrastructure, which incidentally controlled sandflies
Pyrethroid alternatives to DDT:
- Deltamethrin, alphacypermethrin, and lambda-cyhalothrin are the principal WHO-recommended pyrethroids for IRS against sandflies
- Residual activity shorter than DDT on mud walls: 3–6 months; requires two spray cycles per year in endemic regions
- Pyrethroid resistance has been documented in some Phlebotomus populations in high-IRS-pressure settings, raising concern about long-term IRS effectiveness
- Alternative insecticide classes (organophosphates such as malathion; carbamates such as bendiocarb) are used in resistance management rotational programs
IRS effectiveness depends on transmission type:
- Anthroponotic VL (L. donovani in South Asia): highly effective — the entire transmission cycle occurs between humans and the peridomestic sandfly; IRS reduces the biting rate on the reservoir (humans) directly
- Zoonotic VL and CL (with animal reservoirs): less effective in isolation because spraying the inside of human homes does not interrupt the animal–sandfly transmission cycle occurring outdoors; IRS must be combined with reservoir control
5. Environmental and Breeding Site Management
Reducing sandfly breeding habitat in and around human settlements can lower local vector density, though this approach is labor-intensive and community compliance-dependent. Unlike mosquito larval source reduction (targeting standing water), sandfly breeding site reduction targets organic matter in soil and peridomestic structures.
Practical measures:
- Clearing leaf litter, rubble, and organic debris from within 50 meters of homes; sandfly larvae require moist, organic-rich soil and cannot complete development in bare ground
- Sealing cracks in walls and floors (particularly mud or clay construction): these serve as both breeding sites and daytime resting refugia for adult sandflies
- Relocating livestock pens: animals serve as alternative blood meal sources for sandflies; keeping cattle and goats at a distance from sleeping areas reduces the peridomestic sandfly density
- Plastering walls: smooth plaster on interior walls reduces sandfly resting sites and allows IRS insecticide to be applied more effectively (insecticide runs off smooth surfaces less quickly than rough mud walls)
- Village-level clearing of vegetation within 100–200 meters of homes: reduces sandfly resting habitat; most effective for Phlebotomus papatasi (a CL vector that breeds in peridomestic rodent burrows)
6. Reservoir Control: Zoonotic CL (Rodent Reservoirs)
Many forms of cutaneous leishmaniasis in the Old World are zoonotic — the parasite cycles between sandflies and rodent reservoir hosts, with humans as incidental dead-end hosts who cannot sustain transmission. Understanding the reservoir is essential to controlling transmission, but rodent reservoir control has proven extremely difficult in practice.
Key Old World CL reservoirs:
- L. major (the dominant CL species of the Middle East, Central Asia, and Sub-Saharan Africa): reservoir is primarily fat sand rats (Psammomys obesus) and gerbils (Meriones species); these rodents live in burrow systems in arid and semi-arid scrubland
- L. tropica (urban CL in South Asia, the Middle East, and East Africa): reservoir includes Cavia porcellus and dogs in some settings; transmission in dense urban environments can become partially anthroponotic
Rodent control challenges:
- Rodenticide campaigns targeting burrow systems are expensive, ecologically disruptive, and have produced limited or short-lived results in field programs; gerbil and sand rat populations recover rapidly after control measures end
- Ecological disruption (plowing agricultural land, destroying burrow systems) can temporarily reduce rodent density but may displace the reservoir further into fringe peridomestic areas
- No cost-effective, scalable rodent reservoir control strategy has been validated for large-scale CL prevention; most programs default to human personal protection and IRS instead
7. Canine Reservoir Control and Dog Vaccination
In the Mediterranean basin (southern Europe, North Africa, the Middle East) and Latin America (Brazil, Colombia, Venezuela), the primary reservoir of L. infantum/chagasi VL is domestic and peridomestic dogs. Dogs develop a chronic, often asymptomatic infection that makes them a sustained source of parasite for sandflies. Controlling the canine reservoir is therefore central to reducing human VL risk in these regions — but the methods available are each limited by cost, logistics, or ethics.
Serological screening and euthanasia of seropositive dogs (Brazil, historical):
- Brazil's national program required serological screening of dogs in endemic municipalities followed by euthanasia of rdogs testing positive for anti-Leishmania antibodies; this program was in place from the 1950s through the 2000s
- Efficacy was disputed: epidemiological studies showed limited correlation between dog culling rates and human VL incidence, possibly because: (1) seropositive dogs were often replaced by new susceptible dogs; (2) serological tests have imperfect sensitivity and specificity; (3) the sandfly–dog cycle continued in wildlife and peridomestic populations even when domestic dogs were culled
- Massive public opposition and animal welfare advocacy significantly undermined the program; Brazil's Federal Council of Medicine of Veterinary Medicine formally opposed euthanasia as the primary control strategy
Dog treatment with antileishmanial drugs:
- Miltefosine and meglumine antimoniate can suppress L. infantum in infected dogs; treatment clears clinical disease but does not reliably achieve sterile cure — dogs remain infectious to sandflies even after apparent clinical recovery
- WHO does NOT recommend treating infected dogs as a primary public health measure because: (1) treatment does not reliably stop transmission; (2) treating dogs with drugs used for human VL risks accelerating resistance development
- Dog treatment for clinical disease is a veterinary welfare decision, not a public health one
Dog vaccination (the most promising current approach):
- Leish-Tec (Brazil, approved 2014): recombinant L. donovani A2 antigen + saponin adjuvant; field trials showed reduction in canine VL incidence in vaccinated dogs; reduces infectiousness of vaccinated dogs to sandflies; used in national programs in Brazil
- CaniLeish (Europe, European Medicines Agency approved 2011): purified excreted/secreted proteins of L. infantum + QA-21 adjuvant; reduces risk of developing active clinical leishmaniasis in exposed dogs by approximately 70% in field conditions; does not prevent infection but significantly reduces parasite burden and infectiousness to sandflies
- Dog vaccination is now the preferred control approach in Mediterranean Europe and increasingly in Brazil; the vaccination strategy aims to reduce the sandfly infectious pool size by reducing parasite burden in the reservoir
Deltamethrin-impregnated dog collars (Scalibor collar):
- Highly effective at preventing sandfly bites on dogs by killing sandflies that contact the collar; field studies in Italy, Spain, and Iran show 65–90% reduction in sandfly biting on collared dogs
- By protecting dogs from sandfly bites, collars both prevent infection of currently uninfected dogs AND reduce the probability that sandflies feeding on infected dogs will acquire the parasite (since sandflies must feed on a dog to acquire infection, but the collar kills them before they can feed successfully)
- Collar must be replaced every 6 months; compliance with replacement schedule affects effectiveness
- Mass collar deployment in endemic villages shows community-level reduction in canine seroprevalence and, in some studies, reduction in human cases
8. Human Vaccine Development
No licensed human vaccine against any form of leishmaniasis existed as of 2026. The historical observation that natural cutaneous leishmaniasis infection confers durable, often lifelong, immunity to reinfection with the same species established that protective immunity is achievable — the immune system can control Leishmania. This provides a biological basis for vaccination, and it spurred a century of vaccine development efforts that have yet to yield a licensed product.
Leishmanization (historical):
- Deliberate inoculation with live L. major from human lesions (leishmanization) was practiced for centuries in the Middle East and Central Asia as a form of variolation: parents would inoculate children on a covered body part to induce a controlled CL lesion and lifelong immunity, protecting against facial scarring from natural infection
- Practiced in the Soviet Union, Israel, and Iran into the 1970s–80s; abandoned because: (1) risk of progressive or uncontrolled lesions; (2) risk of mucocutaneous spread in susceptible individuals; (3) batch standardization was impossible; (4) regulatory and ethical barriers to intentional infection with a pathogen
- Demonstrates proof-of-concept for sterilizing immunity but is not a modern vaccine strategy
Current pipeline (as of 2026):
- LEISH-F3+GLA-SE (Infectious Disease Research Institute / Eisai): fusion protein combining three Leishmania antigens (nucleoside hydrolase NH36, sterol 24-c-methyltransferase SMT, and a polyprotein antigen) formulated with synthetic TLR4 agonist GLA in stable emulsion adjuvant; Phase 2 clinical trials in Brazil and Bangladesh ongoing (targeting VL and CL); Phase 1 showed excellent safety and immunogenicity with strong Th1 bias (IFN-gamma, TNF-alpha induction)
- ChAd63-KH (Oxford/Wellcome Centre for Human Genetics): chimpanzee adenovirus 63 vector expressing Leishmania kinetoplastid membrane protein 11 (KMP-11) and hydrophilic acylated surface protein B (HASPB); designed for VL; Phase 2b trials in East Africa; adenoviral vector platform allows single-dose immunization and strong cellular immune response
- PKDL prophylaxis vaccine: a distinct goal of vaccine development in South Asia is a vaccine to prevent PKDL after VL treatment, since PKDL sustains transmission; considered a high-priority target by the South Asian elimination program
- Challenges: correlates of protective immunity are not fully defined; animal models (mice) do not reliably predict human protection; the duration of vaccine-induced immunity required for field effectiveness is not established; clinical endpoints for vaccine trials require long follow-up and large sample sizes in heterogeneous endemic populations
9. South Asia VL Elimination Program
The South Asian VL elimination program, launched jointly by India, Nepal, and Bangladesh in 2005 with WHO support, set the ambitious target of reducing VL incidence below 1 case per 10,000 population per year (at the sub-district level) by 2015. The target date was extended as progress proved slower than optimistic projections, but the program has achieved substantial and real reductions in case counts — among the most dramatic successes of any regional NTD control program.
Program pillars:
- Indoor residual spraying (IRS): two rounds per year in high-incidence districts; initial DDT (leveraging existing malaria control infrastructure) transitioned to synthetic pyrethroids as DDT use declined; IRS remains the cornerstone vector control measure
- Insecticide-treated nets (ITN/LLIN): distributed to high-risk households in high-incidence blocks; proven to reduce transmission independently of IRS
- Active case detection: trained village health workers (ASHAs in India) trained to recognize VL signs (fever >2 weeks, splenomegaly) and refer for rK39 rapid testing; early diagnosis reduces the duration of human infectiousness and the reservoir
- Free diagnosis and treatment: rK39 RDT and all first-line VL treatments (including liposomal AmphoB and miltefosine) provided free of charge under national programs; removing financial barriers to treatment reduces the untreated reservoir
- PKDL management: PKDL patients are an important treatment priority because they are clinically apparent skin-disease patients who sustain sandfly transmission; the program includes PKDL surveillance and treatment to reduce this reservoir component
Achievements: India achieved a 95% reduction in reported VL cases between 2005 and 2020 (from approximately 45,000 cases/year to <2,000/year). Nepal and Bangladesh achieved comparable reductions. Some districts and blocks have met the 1/10,000 elimination target. These reductions are real — cross-validated by serological surveys and healthcare utilization data, not just passive reporting changes.
Remaining challenges: PKDL prevalence remains a reservoir concern; climate change is expanding the geographic range of Phlebotomus vectors northward in South Asia and Europe; asymptomatic L. donovani infection rates in the community (detected by PCR and serology) remain high even in areas meeting the case-count target; and the elimination program requires sustained funding and political commitment in settings with competing health priorities.
10. Advice for Travelers to Endemic Areas
Travelers from non-endemic countries visiting leishmaniasis-endemic areas face meaningful risk, particularly if they are immunocompromised (including patients on biologics, corticosteroids, or immunosuppressants; HIV-positive individuals; and organ transplant recipients). No licensed pre-exposure prophylaxis exists; protection relies entirely on personal measures.
Before travel:
- Understand which form of leishmaniasis is present in the destination: CL risk in the Middle East, Morocco, Central Asia, Peru, and Colombia; VL risk in rural Bihar, southern Sudan, Ethiopia, and the Mediterranean basin
- Immunocompromised travelers to VL-endemic areas should consult an infectious disease specialist before departure; the risks are substantially higher in this group
- Purchase picaridin 20% or DEET 30% repellent; purchase permethrin spray for clothing treatment if not using pre-treated garments
- Book air-conditioned accommodation where possible; window screens in non-AC rooms
During travel:
- Apply repellent to all exposed skin from dusk to dawn; reapply every 2–3 hours; cover lower legs and ankles particularly
- Wear permethrin-treated long-sleeved shirts and long trousers at dusk and during the night
- Sleep under an insecticide-treated net in non-air-conditioned rooms; fine-mesh net preferred in air-conditioned rooms
- Avoid outdoor activities at dawn and dusk in sandfly-infested areas when possible
After travel:
- CL: report any slowly healing skin ulcer that appeared weeks to months after travel to an endemic area, regardless of whether you recall being bitten; see a travel medicine or infectious disease specialist
- VL: prolonged fever (>2 weeks), weight loss, and left-sided abdominal fullness (splenomegaly) in someone returned from an endemic area warrants VL evaluation; rK39 serology and full blood count (pancytopenia) are the initial tests
- Incubation period: CL typically 2 weeks to 2 months; VL 2 months to several years; VL presenting years after return from an endemic area is well-documented in European patients
Key Research Papers
Peer-reviewed field studies, systematic reviews, and program evaluations on sandfly vector control, reservoir management, dog vaccination, human vaccine trials, and the South Asian elimination program. PMID links open the PubMed record.
- Olliaro PL, Shamsuzzaman TAK, Manica M, et al. Combination treatments for visceral leishmaniasis in East Africa. Lancet Infect Dis. 2015;15(9):1012–1018 — Search PubMed
- Alvar J, Vélez ID, Bern C, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS ONE. 2012;7(5):e35671 — Search PubMed
- Chappuis F, Sundar S, Hailu A, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007;5(11 Suppl):S7–S16 — Search PubMed
- Sundar S, Sinha PK, Rai M, et al. Comparison of short-course multidrug treatment with standard therapy for visceral leishmaniasis in India. Bull World Health Organ. 2011;89(10):726–734 — Search PubMed
- Musa AM, Mbui J, Khalil EA, et al. Efficacy and safety of liposomal amphotericin B versus miltefosine for treatment of post-kala-azar dermal leishmaniasis in Sudan and India. PLoS Negl Trop Dis. 2019;13(8):e0007673 — Search PubMed
- Mondal D, Hasnain MG, Hossain MS, et al. Study on drug efficacy for visceral leishmaniasis in Bangladesh. Trans R Soc Trop Med Hyg. 2019;113(9):556–564 — Search PubMed
- Sundar S, Chakravarty J, Agarwal D, et al. Single-dose liposomal amphotericin B for visceral leishmaniasis in India. N Engl J Med. 2010;362(6):504–512 — Search PubMed
- Sundar S, Singh A, Rai M, et al. Efficacy of miltefosine in the treatment of visceral leishmaniasis in India after a decade of use. Clin Infect Dis. 2012;55(4):543–550 — Search PubMed
- Dorlo TPC, Balasegaram M, Beijnen JH, de Vries PJ. Miltefosine: a review of its pharmacology and therapeutic efficacy in the treatment of leishmaniasis. J Antimicrob Chemother. 2012;67(11):2576–2597 — Search PubMed
- Cota GF, de Sousa MR, Fereguetti TO, et al. The cure rate after placebo or no therapy in American cutaneous leishmaniasis. PLoS Negl Trop Dis. 2016;10(2):e0004361 — Search PubMed
Live PubMed Searches
Each link opens a live PubMed query for current literature.
- Sandfly vector control
- ITN / LLIN for VL
- IRS leishmaniasis India
- Canine leishmaniasis vaccine
- Repellent efficacy sandflies
- Leishmaniasis human vaccine trials
- South Asia VL elimination program
- Zoonotic leishmaniasis reservoir control
Connections
- All Parasites
- Leishmania: Leishmaniasis Overview
- Treatments Hub
- Liposomal Amphotericin B
- Miltefosine and Antimonials
- Symptoms Hub
- Visceral Leishmaniasis (Kala-Azar)
- Cutaneous & Mucosal Leishmaniasis
- Malaria
- Infectious Disease