Amoebic Liver Abscess Drainage
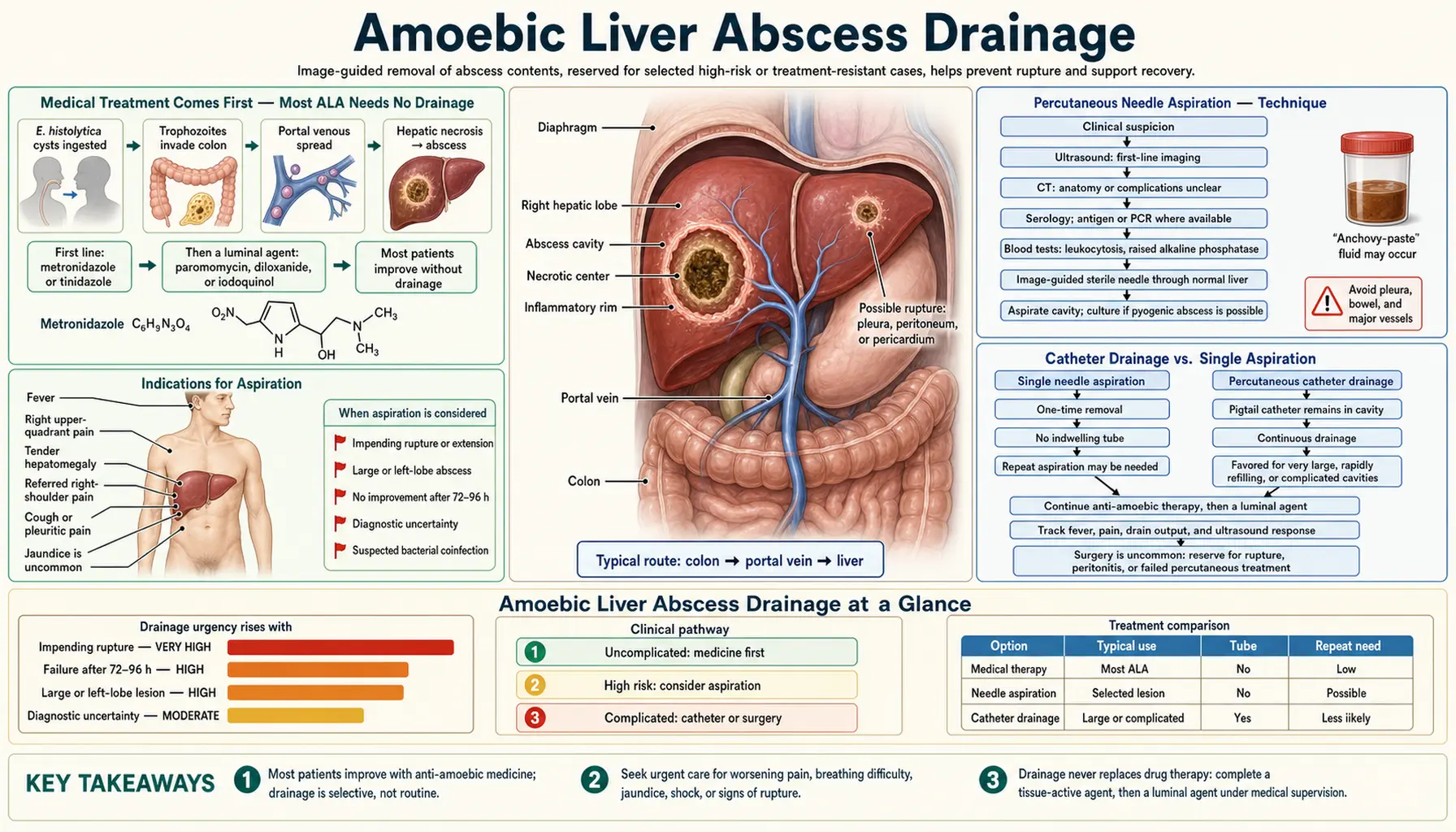
Table of Contents
- Medical Treatment Comes First — Most ALA Needs No Drainage
- Indications for Aspiration
- Percutaneous Needle Aspiration — Technique
- Catheter Drainage vs. Single Aspiration
- Open Surgical Drainage — When It Is Needed
- Left-Lobe Abscesses — Special Considerations
- Secondary Bacterial Superinfection
- Follow-Up Imaging and Cavity Resolution
- Always Complete the Luminal Amebicide Course
- Key Research Papers
- Connections
- Featured Videos
1. Medical Treatment Comes First — Most ALA Needs No Drainage
The most important principle in managing amebic liver abscess (ALA) is that most cases respond completely to drug therapy alone. Unlike pyogenic (bacterial) liver abscesses, which almost always require drainage for cure, ALA resolves in the majority of patients with nitroimidazole therapy (metronidazole or tinidazole) without any procedural intervention. This difference reflects the liquefied, non-loculated nature of amebic abscess material and the excellent tissue penetration of nitroimidazoles.
Clinical response to medical treatment is typically rapid and reassuring:
- Fever resolves within 48–72 hours of starting a nitroimidazole in most patients with uncomplicated ALA.
- Pain and tenderness improve over 1–2 weeks.
- Appetite and systemic wellbeing return within the first week.
The decision to perform drainage is therefore not a default but a carefully considered exception — reserved for specific clinical scenarios where drug therapy alone is insufficient or where the risk of complications from the abscess itself outweighs the procedural risk.
2. Indications for Aspiration
The following are the principal indications for percutaneous needle aspiration of an amebic liver abscess:
- Large abscess (>5 cm in diameter). Large abscesses carry a higher risk of spontaneous rupture. Aspiration reduces abscess volume rapidly, relieving pressure and lowering rupture risk. Many guidelines use >5 cm as the threshold; some specialists advocate aspiration for any abscess >10 cm or whenever the abscess wall appears thin or is abutting the liver capsule on imaging.
- Left-lobe location. Left-lobe ALA is a strong indication for aspiration regardless of size, due to the proximity of the left lobe to the pericardium. Left-lobe abscesses can rupture anteriorly into the pericardial sac, causing cardiac tamponade — a rapidly fatal complication. Prophylactic aspiration is generally recommended for all left-lobe ALA detected before rupture.
- Failure to improve after 72 hours of medical therapy. Persistent fever, unabated pain, and no systemic improvement after 72–96 hours of nitroimidazole therapy at adequate dosing should trigger reassessment including aspiration. Failure to improve may indicate a very large abscess, secondary bacterial superinfection, diagnostic uncertainty, or (rarely) drug-related issues.
- Diagnostic uncertainty. When it is unclear whether the hepatic lesion is amebic or pyogenic in origin — particularly if serology is equivocal and the clinical picture is atypical — aspiration of abscess fluid provides material for laboratory analysis to differentiate the two. Amebic abscess fluid is characteristically odorless and chocolate-brown ("anchovy paste"); pyogenic abscess material is purulent and foul-smelling. Gram stain and culture of the aspirate will identify bacteria if present.
- Abscess threatening imminent rupture on imaging (thin-walled, abutting the diaphragm or liver capsule, or with satellite collections suggesting early extrahepatic spread).
- Pregnant patients with large ALA — increased intraabdominal pressure and the risk of rupture with potential consequences for fetal outcome may lower the threshold for drainage.
3. Percutaneous Needle Aspiration — Technique
Ultrasound-guided percutaneous needle aspiration is the standard approach to ALA drainage when intervention is indicated. The procedure is performed under real-time ultrasound imaging, allowing the operator to visualize the needle tip within the abscess cavity continuously and to avoid hepatic vessels and biliary ducts.
Key technical points:
- The approach is typically transcostal (through an intercostal space) or subcostal, depending on abscess location.
- A large-bore needle (18–20 gauge for diagnostic aspiration; 14–16 gauge for therapeutic drainage of viscid material) is advanced under ultrasound guidance to the center of the abscess cavity.
- As much of the liquid contents as possible is aspirated in a single session. The characteristic chocolate-brown, odorless "anchovy paste" material confirms amebic etiology clinically; send fluid for Gram stain, bacterial culture (to exclude superinfection), and PCR for E. histolytica if available.
- Trophozoites are found in the aspirated material in only approximately 15–30% of cases — they tend to be at the abscess periphery rather than in the necrotic central fluid, so a negative trophozoite search in the aspirate does not exclude ALA.
- Following aspiration, the needle is withdrawn and the patient is observed for 4–6 hours for signs of bleeding or bile leak before discharge (in straightforward cases) or continued inpatient monitoring.
Repeat aspiration can be performed if the abscess reaccumulates symptomatic volume after the first aspiration, though this is uncommon in ALA with concurrent adequate medical therapy. In most cases a single aspiration combined with metronidazole is sufficient for definitive treatment.
4. Catheter Drainage vs. Single Aspiration
For pyogenic liver abscesses, percutaneous catheter drainage — leaving an indwelling drain in place for continuous drainage over days — is standard practice and often required. For amebic liver abscesses, catheter drainage is generally not the preferred approach:
- ALA material is characteristically non-viscid enough to be evacuated adequately through a needle in a single aspiration, without leaving a drain.
- The amebic abscess cavity does not reaccumulate rapidly after aspiration combined with effective antiparasitic therapy — continuous drainage is therefore usually unnecessary.
- Catheter drains carry risks of secondary infection, catheter displacement, leakage of bile, and prolonged procedural exposure; these risks are not justified for a condition that typically responds to a single aspiration.
- An exception may be made for very large abscesses (>10 cm) with very thick or particulate content that cannot be adequately evacuated through a needle alone, or when imaging suggests multiloculation — but these are uncommon scenarios in ALA.
When catheter drainage is placed for ALA (as opposed to pyogenic abscess), the drain should be removed as soon as output ceases and clinical improvement is confirmed, typically within a few days.
5. Open Surgical Drainage — When It Is Needed
Open surgical intervention for ALA is required in a minority of cases and is reserved for specific complications:
- Intraperitoneal rupture: When an ALA ruptures through the liver capsule into the peritoneal cavity, the patient develops acute abdomen from amebic peritonitis. Peritoneal lavage and sometimes partial hepatectomy are required alongside systemic antiparasitic therapy. This is the most common surgical emergency in ALA management.
- Pericardial tamponade from left-lobe rupture: Requires emergency pericardiocentesis (which can be percutaneous) alongside immediate antiparasitic therapy; open pericardial drainage may be required if tamponade recurs or a pericardial drain cannot be placed.
- Failure of percutaneous drainage: Rare cases where repeat needle aspiration fails to adequately decompress the abscess or where the abscess location (posterior right-lobe, closely adjacent to major hepatic vein or inferior vena cava) makes percutaneous access unsafe.
- Empyema or hepatobronchial fistula requiring decortication: If pleuropulmonary extension results in trapped empyema or a persistent hepatobronchial fistula not responsive to medical therapy and percutaneous drainage, thoracic surgical intervention may be required.
- Secondary bacterial infection with loculated pyogenic abscess formation: When ALA becomes superinfected with bacteria and the material becomes purulent and loculated, simple needle aspiration may be inadequate; open or laparoscopic drainage may be required.
6. Left-Lobe Abscesses — Special Considerations
Left-lobe ALA deserves specific attention because of its proximity to the pericardium and the life-threatening nature of pericardial rupture. Key points for left-lobe disease:
- Clinical presentation may be atypical: Left-lobe abscess causes epigastric pain rather than the classic right upper quadrant pain of right-lobe disease. This can mislead clinicians toward other diagnoses (peptic ulcer, pancreatitis) and delay imaging of the liver.
- Prophylactic aspiration is recommended for all left-lobe abscesses detected before rupture, regardless of size or initial clinical response to medical therapy. The margin of safety between an intact left-lobe ALA and pericardial tamponade is very narrow — elective percutaneous aspiration carries far lower risk than watchful waiting.
- Emergency pericardiocentesis protocol: All centers managing left-lobe ALA should have immediate access to pericardiocentesis capability. Patients with left-lobe ALA who deteriorate acutely — new hypotension, distant heart sounds, new pulsus paradoxus — require emergency echocardiography to rule out tamponade.
- ECHO monitoring: Serial echocardiography during the initial phase of treatment for left-lobe ALA has been recommended by some experts to detect early pericardial effusion before it becomes hemodynamically significant.
7. Secondary Bacterial Superinfection
Secondary bacterial infection of an amebic liver abscess fundamentally changes its management and prognosis:
- Clinical clues to superinfection: foul-smelling aspirate, purulent rather than chocolate-brown material, failure to improve within 72 hours of nitroimidazoles, rising leukocytosis with marked left shift, new rigors and toxic appearance.
- Laboratory confirmation: Gram stain and aerobic/anaerobic culture of aspirated material revealing bacteria. The most common organisms are enteric gram-negative bacteria (E. coli, Klebsiella) and anaerobes that have seeded the abscess via the portal venous route from the bowel.
- Management: Add broad-spectrum antibiotics covering gram-negative organisms and anaerobes (e.g., piperacillin-tazobactam, or a combination of a cephalosporin plus metronidazole) alongside antiparasitic therapy. Drainage is almost always required for superinfected ALA — catheter drainage rather than single aspiration is appropriate given the bacterial infection.
- Prognosis: Superinfected ALA carries a higher mortality than uncomplicated ALA and requires more prolonged treatment. Hospital stay is extended and drain management is more complex.
8. Follow-Up Imaging and Cavity Resolution
One of the most misunderstood aspects of ALA management is the expected tempo of radiological resolution. The abscess cavity on imaging shrinks very slowly — often over 3 to 12 months after successful treatment — and a persistent cavity at 1–2 months after treatment is not a sign of failure.
What to expect on follow-up imaging:
- At 1 month: the cavity may have shrunk in size but is still well visible on ultrasound; this is entirely normal with effective treatment.
- At 3 months: most cavities are smaller; some have developed a more echogenic (echobright) appearance, reflecting fibrotic replacement.
- At 6–12 months: most cavities have resolved or left only a small residual scar.
- Some patients retain a small calcified scar permanently — not clinically significant.
Clinical rather than radiological response is the primary treatment endpoint. Once fever has resolved, pain has improved, and the patient is clinically well, imaging should not drive decisions about continued or repeated therapy. The most common error in ALA management is repeating imaging at 1–2 months, seeing a persistent cavity, and incorrectly concluding that treatment has failed — leading to unnecessary re-treatment, additional aspiration, or extended courses of nitroimidazoles.
Repeat imaging is appropriate if clinical symptoms recur, if baseline imaging showed a very large abscess requiring confirmation of size reduction, or if left-lobe disease or pericardial proximity is being monitored.
9. Always Complete the Luminal Amebicide Course
Whether or not drainage is performed, every patient treated for ALA must complete a course of luminal amebicide (paromomycin 500 mg three times daily for 10 days, or diloxanide furoate 500 mg three times daily for 10 days) after completing the nitroimidazole tissue-active course.
The reason is the same as for intestinal amoebiasis: nitroimidazoles achieve excellent tissue concentrations but poor luminal concentrations, meaning intestinal cysts may persist even after hepatic disease is cured. Without luminal amebicide treatment:
- Intestinal cysts persist and the patient continues to shed the parasite.
- Risk of recurrent intestinal invasion and potentially recurrent ALA persists.
- The patient remains a source of infection for household contacts and the community.
This step is sometimes omitted in clinical practice when the presenting physician is focused on the dramatic hepatic disease and loses sight of the intestinal reservoir. Ensuring the luminal agent is prescribed and completed is a key quality-of-care measure in ALA management.
10. Key Research Papers
Selected peer-reviewed literature on amebic liver abscess drainage and management.
- Haque R et al. Amebiasis. N Engl J Med. — Search PubMed.
- Petri WA Jr et al. Enteric infection and gut microbiome. Sci Transl Med. — Search PubMed.
- Bercu TE et al. Amebic colitis — new insights. Curr Gastroenterol Rep. — Search PubMed.
- Shirley DT et al. Global burden, diagnostics, therapeutics for amebiasis. Open Forum Infect Dis. — Search PubMed.
- Moonah SN et al. Amebiasis pathogenesis. PLoS Pathog. — Search PubMed.
- Espinosa-Cantellano M, Martínez-Palomo A. Pathogenesis of intestinal amebiasis. Clin Microbiol Rev. — Search PubMed.
- Blessmann J et al. Epidemiology, diagnosis, and treatment of amebic liver abscess. Clin Microbiol Infect. — Search PubMed.
- Fotedar R et al. Laboratory diagnostics for Entamoeba species. Clin Microbiol Rev. — Search PubMed.
- Shirley DT, Watanabe K, Moonah S. Significance of amebiasis. PLoS Negl Trop Dis. — Search PubMed.
- Marie C, Petri WA Jr. Virulence regulation in E. histolytica. Annu Rev Microbiol. — Search PubMed.
Live PubMed Searches
- Amebic liver abscess drainage aspiration
- Amebic liver abscess percutaneous ultrasound
- Amebic liver abscess pericardial rupture
- Amebic abscess resolution imaging follow-up
Connections
- Entamoeba Treatments Overview
- Metronidazole and Tissue Amebicides
- Prevention and Water Safety
- Liver Abscess and Extraintestinal Disease
- Diagnosis — Stool, Antigen, and Serology
- Entamoeba histolytica Main Page
- Nephrology & Hepatology
- All Parasites