Amoebic Dysentery and Colitis
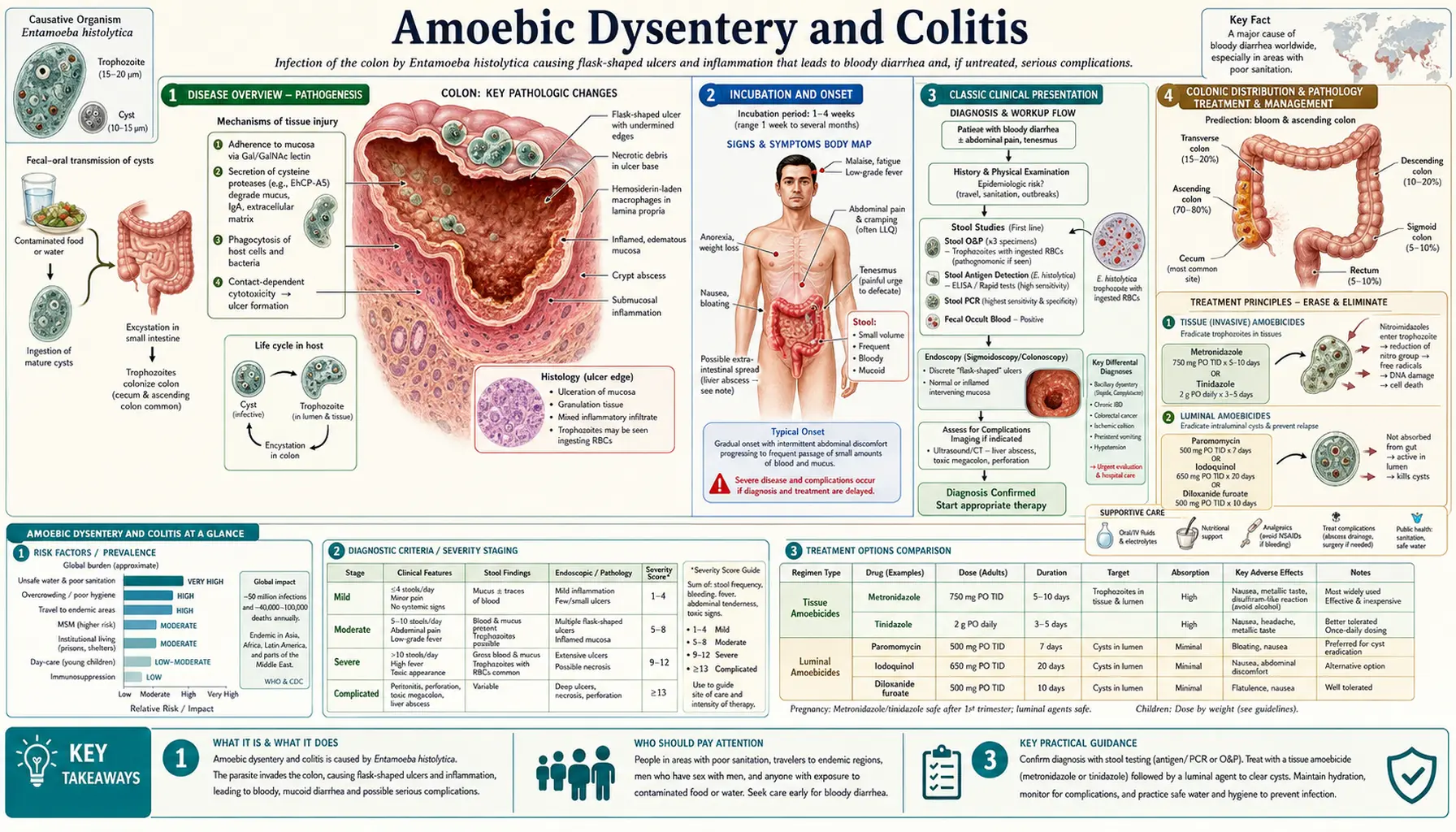
Table of Contents
- Disease Overview
- Incubation and Onset
- Classic Clinical Presentation
- Colonic Distribution and Pathology
- Fulminant Colitis and Toxic Megacolon
- Other Complications
- No Peripheral Eosinophilia — A Key Distinguisher
- Differential Diagnosis
- Key Research Papers
- Connections
- Featured Videos
1. Disease Overview
Amebic colitis — intestinal infection caused by invasive Entamoeba histolytica — is the intestinal form of amoebiasis that occurs when trophozoites penetrate the mucosa of the large intestine. The term amebic dysentery refers specifically to the syndrome of frequent, bloody, mucus-laden stools with cramping and tenesmus that marks moderate-to-severe mucosal invasion. Not all amebic colitis reaches this severity: at one extreme is mild, non-bloody diarrhea indistinguishable from many other causes; at the other is fulminant colitis with transmural necrosis carrying a mortality above 40%.
Amebic colitis occurs in a minority — roughly 10% — of people infected with true E. histolytica. The remaining 90% remain asymptomatic carriers, shedding cysts without experiencing intestinal disease. What triggers the transition from colonization to invasion remains incompletely understood but likely involves a combination of parasite virulence factors, host immune status, the composition of the intestinal microbiome, and nutritional state.
2. Incubation and Onset
The incubation period of amebic colitis — the time from ingestion of cysts to the appearance of symptoms — is classically stated as 2 to 4 weeks in most reviews and textbooks. However, this figure masks considerable variability. In some cases, particularly in travelers who acquire a large inoculum of cysts, symptoms can begin within days. In others, the parasite may reside quietly in the colon for months or even years before invasive disease begins, sometimes manifesting long after the person has returned from an endemic region.
The onset of symptoms is characteristically gradual — one of the clinical features that distinguishes amebic colitis from most bacterial dysenteries, which typically begin abruptly. A patient may notice slowly worsening loose stools over one to three weeks, with the addition of blood and mucus appearing as mucosal invasion deepens. This gradual progression means the diagnosis may not be considered early, and by the time the classic dysenteric picture is established, significant mucosal damage may already be present.
Fever, when it occurs, is usually low-grade in uncomplicated amebic colitis. High fever and systemic toxicity suggest complicated disease — fulminant colitis, perforation, or secondary bacterial infection.
3. Classic Clinical Presentation
The full syndrome of amebic dysentery includes several characteristic features, though not all are present in every patient:
- Bloody, mucus-containing diarrhea. The presence of blood and mucus in the stool reflects mucosal invasion and is the hallmark of amebic dysentery. The classic description is "red currant jelly stool" — a mixture of blood, mucus, and minimal fecal matter — when dysentery is well established. Blood quantity ranges from streaks to grossly bloody stools.
- Lower abdominal cramps. Diffuse or lower abdominal cramping that may worsen before defecation is almost universally present in symptomatic colitis.
- Tenesmus. The persistent, painful urge to defecate even with an empty or nearly empty bowel is a classic feature of rectal involvement and reflects inflammation of the rectosigmoid region.
- Diarrhea frequency. Stool frequency is variable — from 3 to 4 loose stools per day in mild disease to 10 or more small, bloody, mucous stools per hour in fulminant disease.
- Low-grade fever (typically <38.5°C in uncomplicated cases).
- Weight loss and malaise with prolonged or recurrent disease.
- Right-sided abdominal tenderness reflecting the predilection of E. histolytica for the cecum and ascending colon.
Dehydration is a concern in severe cases, particularly in children and elderly patients. Unlike cholera or rotavirus diarrhea, the primary risk in amebic dysentery is mucosal invasion and its complications rather than pure fluid loss.
4. Colonic Distribution and Pathology
E. histolytica has a well-documented predilection for specific regions of the colon. The cecum and ascending colon are most frequently involved, followed by the rectosigmoid. This right-sided predominance is thought to reflect the greater stasis and longer transit time in the cecum, allowing trophozoites more opportunity for contact with the mucosa, as well as the cecum's proximity to the ileocecal valve where excystation occurs. Right-sided tenderness on physical examination — sometimes mimicking acute appendicitis — is therefore a classic finding.
Skip lesions — discrete areas of ulceration separated by stretches of normal-appearing mucosa — are the endoscopic hallmark of amebic colitis. This pattern contrasts with the continuous mucosal inflammation of ulcerative colitis, though the two can be confused, with serious consequences (see Section 8 on differential diagnosis). The classic pathological lesion is the flask-shaped ulcer:
- Trophozoites breach the thin surface epithelium at a small point.
- They then spread laterally through the submucosa, which offers less resistance than the epithelium.
- The result is an ulcer narrow at the luminal opening and wide at its base — shaped like a flask or bottle.
- The ulcer base may contain trophozoites, necrotic tissue, blood, and mucus.
- In severe disease, adjacent flask ulcers may coalesce, producing large areas of mucosal denudation.
5. Fulminant Colitis and Toxic Megacolon
Fulminant amebic colitis is a medical emergency with a mortality rate exceeding 40% even with aggressive treatment. It is defined by extensive transmural necrosis of the colon, hemodynamic instability, and systemic toxicity. Toxic megacolon — colonic dilatation >6 cm with systemic signs of toxicity — is the most feared complication and carries a mortality rate approaching 50–80% in historical series.
Risk factors for fulminant disease include:
- Corticosteroid administration — the most dangerous precipitant; corticosteroids can convert subclinical or mild amebic colitis to fulminant disease by suppressing the macrophage and T-cell responses that normally limit trophozoite invasion.
- Young children, particularly those <2 years old.
- Malnutrition and severe immunosuppression.
- Pregnancy — particularly the third trimester and postpartum period.
Misdiagnosis as inflammatory bowel disease (IBD) is a well-recognized and potentially fatal error. Amebic colitis can closely mimic ulcerative colitis or Crohn's disease both clinically and endoscopically. When IBD is incorrectly diagnosed and treated with high-dose corticosteroids or other immunosuppressants, the resulting immune suppression can allow E. histolytica to invade rapidly and without restraint. Every patient being considered for IBD induction therapy in an endemic area or with a travel history should have amoebiasis excluded by stool antigen testing or PCR before immunosuppression is started.
6. Other Complications
Beyond fulminant colitis, intestinal amoebiasis can produce several distinct complications:
- Intestinal perforation. Transmural invasion of the bowel wall leads to perforation and fecal peritonitis. Perforation can also result from toxic megacolon. Perforation with peritonitis carries a very high mortality and requires emergency surgical intervention alongside antiparasitic therapy.
- Amoeboma. An amoeboma is a granulomatous, tumor-like inflammatory mass that forms in the bowel wall as a chronic host response to trophozoite invasion. Most commonly found in the cecum or sigmoid colon, amoebomas can appear on imaging as an annular constricting lesion that closely mimics colonic carcinoma, leading to unnecessary surgery when the parasitic cause is not recognized. They resolve with antiparasitic treatment.
- Appendicitis-like syndrome. Cecal involvement can produce right iliac fossa pain and tenderness indistinguishable clinically from acute appendicitis. Cases of amebic involvement of the appendix itself have been reported.
- Chronic non-dysenteric amebic colitis. Some patients develop intermittent loose stools, flatulence, and abdominal discomfort persisting for years without frank dysentery — a pattern sometimes misattributed to irritable bowel syndrome.
- Rectovaginal or perianal fistulae. Rare complications of deep perirectal invasion.
7. No Peripheral Eosinophilia — A Key Distinguisher
A diagnostically important negative finding in amebic colitis is the absence of peripheral blood eosinophilia. Eosinophil counts remain normal in amoebiasis, even in severe invasive disease. This stands in sharp contrast to helminthic (worm) infections — such as strongyloidiasis, ascariasis, hookworm infection, and toxocariasis — which characteristically produce marked eosinophilia during their tissue-invasive phases. Schistosomiasis, another important cause of bloody diarrhea in endemic regions, also causes eosinophilia.
When a patient presents with bloody diarrhea and a very high eosinophil count, the differential tilts away from amoebiasis and toward helminthic disease. Conversely, the absence of eosinophilia is fully consistent with amebic colitis and should not be used to dismiss it. This distinction helps clinicians prioritize diagnostic testing when laboratory resources are limited.
Similarly, leukocytosis is inconsistent in uncomplicated amebic colitis — white blood cell counts may be normal or only mildly elevated. Marked leukocytosis suggests secondary bacterial infection or fulminant disease.
8. Differential Diagnosis
Amebic colitis shares clinical and endoscopic features with several other conditions that must be considered:
- Bacillary dysentery (Shigella, Campylobacter, enteroinvasive E. coli, Salmonella): typically more abrupt onset, often with higher fever; stool culture distinguishes them. Shigella in particular causes a similar clinical syndrome of bloody diarrhea and tenesmus.
- Inflammatory bowel disease (ulcerative colitis, Crohn's disease): the most dangerous misdiagnosis; see Section 5. Chronicity, extraintestinal manifestations, and negative amebiasis serology/antigen tests help distinguish IBD from amebic colitis.
- Ischemic colitis: sudden onset, usually in older patients with vascular risk factors; typically affects the watershed areas (splenic flexure, sigmoid).
- Cytomegalovirus colitis: occurs in immunosuppressed patients; biopsy shows characteristic CMV inclusion bodies.
- Colonic carcinoma: amoeboma may mimic colonic cancer on imaging; treatment response to metronidazole confirms the parasitic cause.
- Balantidium coli infection: another protozoan causing dysentery, rare in humans; distinguished by its very large ciliated trophozoites on microscopy.
9. Key Research Papers
Selected peer-reviewed literature on amebic colitis and dysentery, including pathogenesis, clinical features, and complications.
- Haque R et al. Amebiasis. N Engl J Med. — Search PubMed.
- Shirley DT et al. Global burden, diagnostics, and therapeutics for amebiasis. Open Forum Infect Dis. — Search PubMed.
- Petri WA Jr et al. Enteric infection and dehydration. Sci Transl Med. — Search PubMed.
- Moonah SN et al. Amebiasis pathogenesis. PLoS Pathog. — Search PubMed.
- Bercu TE et al. Amebic colitis — new insights. Curr Gastroenterol Rep. — Search PubMed.
- Espinosa-Cantellano M, Martínez-Palomo A. Pathogenesis of intestinal amebiasis. Clin Microbiol Rev. — Search PubMed.
- Blessmann J et al. Epidemiology and liver abscess treatment. Clin Microbiol Infect. — Search PubMed.
- Fotedar R et al. Laboratory diagnostics for Entamoeba species. Clin Microbiol Rev. — Search PubMed.
- Shirley DT, Watanabe K, Moonah S. Significance of amebiasis. PLoS Negl Trop Dis. — Search PubMed.
- Marie C, Petri WA Jr. Virulence regulation in E. histolytica. Annu Rev Microbiol. — Search PubMed.
Live PubMed Searches
- Amebic colitis Entamoeba histolytica
- Amebic dysentery bloody diarrhea
- Fulminant amebic colitis toxic megacolon
- Amoeboma bowel amoebiasis
Connections
- All Parasites
- Entamoeba Symptoms Overview
- Liver Abscess and Extraintestinal Disease
- Diagnosis — Stool, Antigen, and Serology
- Metronidazole and Tissue Amebicides
- Entamoeba histolytica Main Page
- Gastroenterology
- Infectious Disease