Entamoeba histolytica Treatments
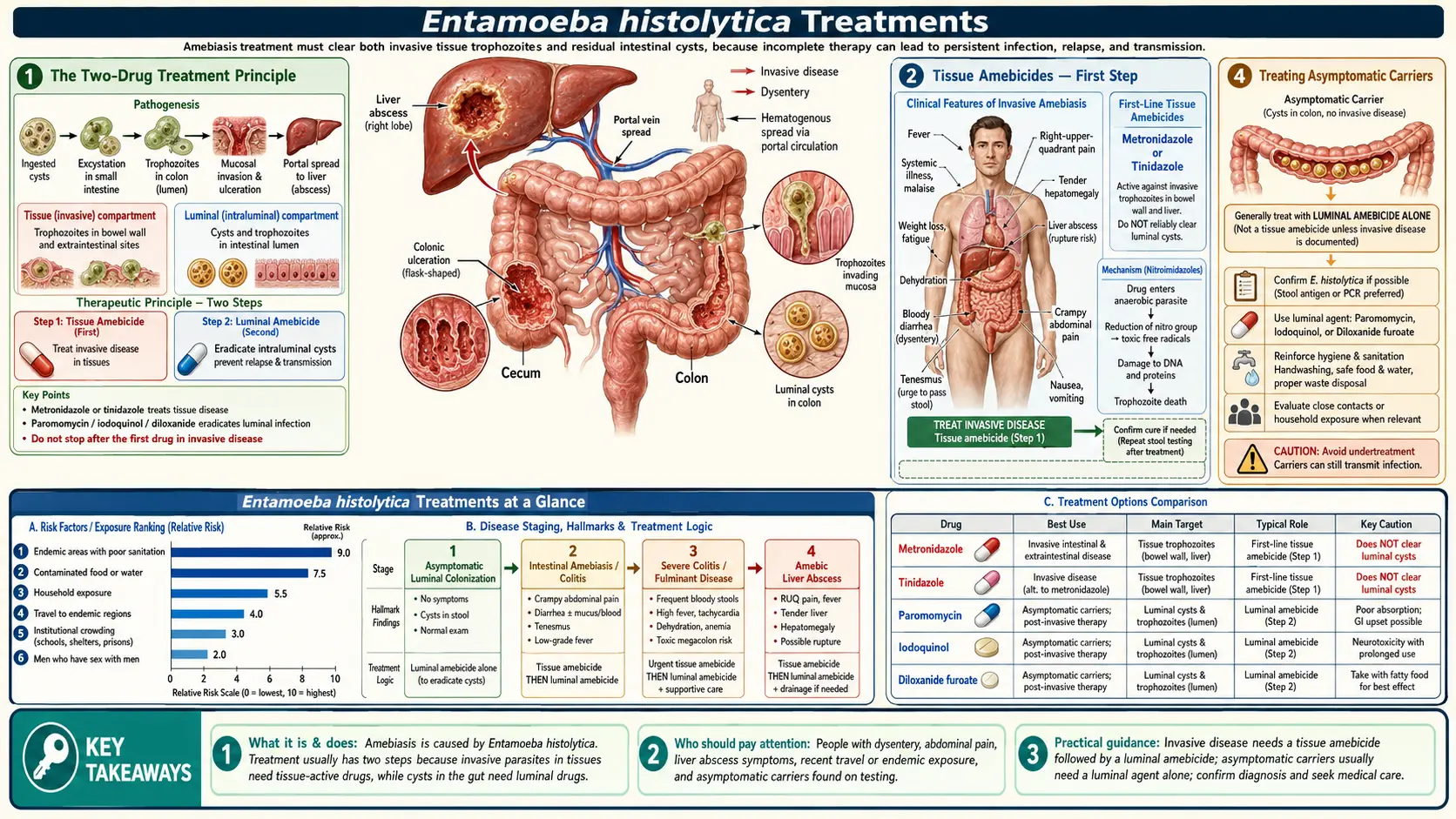
Table of Contents
- The Two-Drug Treatment Principle
- Tissue Amebicides — First Step
- Luminal Amebicides — Second Step
- Treating Asymptomatic Carriers
- Amebic Liver Abscess Treatment
- Surgical and Drainage Interventions
- Monitoring Treatment Response
- Special Populations
- Key Research Papers
- Connections
- Featured Videos
1. The Two-Drug Treatment Principle
Effective treatment of invasive amoebiasis requires a two-step, two-drug strategy that targets the parasite in both its tissue-invasive phase and its luminal cyst phase. This principle underpins all current treatment guidelines and is essential to understand before considering specific drugs:
- Step 1 — Tissue amebicide: A drug that penetrates tissues to kill trophozoites that have invaded the gut wall, liver, or other organs. The nitroimidazoles — primarily metronidazole and tinidazole — are the drugs of choice. They are rapidly absorbed and achieve high tissue concentrations, but they poorly penetrate the intestinal lumen and do not reliably eliminate cysts sitting in the gut.
- Step 2 — Luminal amebicide: A drug that acts specifically within the intestinal lumen (the inside channel of the bowel) to eliminate remaining cysts and any intestinal trophozoites not cleared by the tissue amebicide. The luminal amebicide must always follow the tissue amebicide to prevent relapse and to stop ongoing cyst shedding.
Skipping the second step is a common error that results in a high relapse rate. Even after successful tissue-phase treatment of amebic colitis or liver abscess, intestinal cysts persist and can re-invade at any time. The luminal amebicide closes this loop.
2. Tissue Amebicides — First Step
Nitroimidazoles are prodrugs activated by the parasite's anaerobic ferredoxin-dependent electron-transport system. The activated form generates cytotoxic free radicals that damage DNA and other critical cell components specifically within the anaerobic or microaerophilic environment of the parasite — a selectivity that spares aerobic host cells from the same damage.
- Metronidazole — the most widely used and studied agent. Standard dosing for invasive amebic colitis: 750 mg three times daily for 10 days (adults). For amebic liver abscess, some guidelines use 750 mg three times daily for 5–10 days; others use higher-dose shorter courses. IV formulation is available for severe or complicated disease. Side effects include metallic taste, nausea, and a disulfiram-like reaction with alcohol — patients must abstain from alcohol during treatment and for 48 hours after stopping.
- Tinidazole — a newer nitroimidazole with a longer half-life, better tolerability, and simpler dosing: 2 g once daily for 3 days (colitis) or 3–5 days (liver abscess). Now considered a preferred alternative to metronidazole in many guidelines for its convenience and reduced side-effect burden.
- Secnidazole — a third nitroimidazole with an even longer half-life, allowing single-dose treatment (2 g once) for uncomplicated intestinal amoebiasis; not as widely available globally.
- Ornidazole — used in some countries; similar mechanism and efficacy to metronidazole.
3. Luminal Amebicides — Second Step
Luminal agents act within the intestinal lumen and are poorly absorbed — this pharmacokinetic property is both their limitation (they do not reach tissues) and their strength (they achieve high intraluminal concentrations with low systemic toxicity).
- Paromomycin — the preferred luminal amebicide. It is an aminoglycoside antibiotic that is not absorbed from the gut. It disrupts protein synthesis in ameba ribosomes, killing trophozoites and cysts in the intestinal lumen. Dosing: 500–750 mg three times daily for 10 days. Minimal systemic toxicity; most side effects (nausea, loose stools) are gastrointestinal and local. Available in many countries.
- Diloxanide furoate — an alternative luminal amebicide, particularly used in some endemic countries where paromomycin is less available. Dosing: 500 mg three times daily for 10 days. Mechanism involves disruption of ameba cytoplasm. Generally well tolerated.
- Iodoquinol — an older luminal amebicide (iodinated quinoline); still used in some settings. Requires longer courses and has higher risk of adverse effects with prolonged use (optic neuritis at very high doses historically). Less preferred where paromomycin or diloxanide are available.
4. Treating Asymptomatic Carriers
Whether and when to treat asymptomatic carriers of E. histolytica depends on context:
- Non-endemic settings (e.g., travelers, immigrants in high-income countries): Current guidelines generally recommend treating confirmed E. histolytica carriers with a luminal amebicide alone (tissue amebicide is not needed for asymptomatic, non-invasive infection). Paromomycin or diloxanide furoate for 10 days eliminates intestinal colonization, prevents future invasive disease, and stops cyst shedding that could infect contacts. Species confirmation by antigen or PCR is essential before treating — treating asymptomatic E. dispar carriers is unnecessary and should be avoided.
- Endemic settings: The decision is more complex because reinfection after treatment is common. Mass treatment programs for all ameba-positive individuals in high-burden communities are not current practice; targeted treatment of identified E. histolytica carriers remains the standard approach where testing is available.
- Immunocompromised patients: Any confirmed E. histolytica carrier who is immunosuppressed should be treated promptly, as the risk of progression to invasive disease is higher.
5. Amebic Liver Abscess Treatment
Amebic liver abscess (ALA) responds dramatically and often rapidly to nitroimidazole therapy alone, without the need for drainage in most cases. This is one of the features that distinguishes ALA from pyogenic bacterial abscess, which typically requires drainage.
- Initiate a tissue amebicide (metronidazole or tinidazole) promptly upon clinical diagnosis — do not wait for aspiration or serology confirmation in a high-probability case.
- Fever typically begins to improve within 48–72 hours of starting nitroimidazole therapy. Failure to improve by 72–96 hours is an indication to reassess: consider diagnostic aspiration, secondary bacterial superinfection, or alternative diagnosis.
- Pain and tenderness improve over 1–2 weeks. The abscess cavity on imaging resolves very slowly — over 3 to 12 months in many cases — and this slow radiological resolution is not a sign of treatment failure. Imaging should not be used as the primary endpoint of treatment response.
- After completing the tissue amebicide course, follow with a full course of luminal amebicide (paromomycin or diloxanide furoate) to eliminate intestinal cysts.
6. Surgical and Drainage Interventions
Most cases of ALA do not require invasive intervention. The principal indications for aspiration or drainage are covered in detail on the Liver Abscess Drainage page. In brief:
- Percutaneous needle aspiration (ultrasound-guided) is the preferred approach when drainage is needed — single aspiration is usually sufficient for ALA; catheter drainage is rarely necessary.
- Indications for aspiration: abscess >5 cm (rupture risk), left-lobe location (pericardial rupture risk), failure to improve after 72 hours of medical treatment, diagnostic uncertainty.
- Open surgical drainage is reserved for intraperitoneal rupture requiring peritoneal lavage, or secondary bacterial abscess not amenable to percutaneous drainage.
- Fulminant amebic colitis / toxic megacolon may require emergency colectomy if medical treatment fails — a high-mortality scenario requiring coordinated surgical and medical management.
7. Monitoring Treatment Response
Response to treatment is primarily monitored clinically:
- Fever resolution within 48–72 hours of starting nitroimidazoles confirms therapeutic response to ALA.
- Symptomatic improvement in diarrhea, pain, and systemic symptoms over days to 1–2 weeks in colitis.
- Stool antigen or PCR testing can be repeated 4 weeks after treatment to confirm eradication, though this is not always performed in routine practice if clinical response is clear.
- Liver imaging should not be repeated frequently to monitor ALA resolution — the cavity shrinks slowly over months and persistent cavity on imaging at 1–2 months does not indicate treatment failure. Follow-up imaging at 3–6 months is appropriate for large abscesses or when clinical course is uncertain.
- Serology remains positive for months to years after successful treatment and cannot be used to confirm cure.
8. Special Populations
- Pregnancy: Metronidazole is generally avoided in the first trimester if possible; tinidazole is contraindicated throughout pregnancy (limited safety data, potential fetal harm in animal models). Paromomycin (luminal only) is considered safer in pregnancy for asymptomatic colonization because it is not absorbed. Severe invasive amoebiasis in pregnancy requires treatment — the risk of untreated disease outweighs drug risk in most scenarios; decisions should involve specialist consultation.
- Pediatric patients: Dosing is weight-based. Metronidazole and tinidazole are used in children at appropriate pediatric doses. Paromomycin is the preferred luminal agent in children.
- HIV-infected patients: Standard treatment regimens apply. There is no evidence that HIV infection significantly reduces efficacy of nitroimidazoles, but immune reconstitution may take longer and monitoring should be more frequent.
- Drug resistance: Clinical resistance to nitroimidazoles in E. histolytica has been experimentally induced in the laboratory but is not a recognized clinical problem in current practice. Treatment failure should prompt reassessment of the diagnosis rather than assumption of drug resistance.
9. Key Research Papers
Selected peer-reviewed literature on treatment of amoebiasis and amebic liver abscess.
- Haque R et al. Amebiasis. N Engl J Med. — Search PubMed.
- Shirley DT et al. Global burden, diagnostics, and therapeutics for amebiasis. Open Forum Infect Dis. — Search PubMed.
- Petri WA Jr et al. Enteric infection and dehydration. Sci Transl Med. — Search PubMed.
- Moonah SN et al. Amebiasis pathogenesis. PLoS Pathog. — Search PubMed.
- Bercu TE et al. Amebic colitis — new insights. Curr Gastroenterol Rep. — Search PubMed.
- Espinosa-Cantellano M, Martínez-Palomo A. Pathogenesis of intestinal amebiasis. Clin Microbiol Rev. — Search PubMed.
- Blessmann J et al. Epidemiology, diagnosis, and treatment of liver abscess. Clin Microbiol Infect. — Search PubMed.
- Fotedar R et al. Laboratory diagnostics for Entamoeba species. Clin Microbiol Rev. — Search PubMed.
- Shirley DT, Watanabe K, Moonah S. Significance of amebiasis. PLoS Negl Trop Dis. — Search PubMed.
- Marie C, Petri WA Jr. Virulence regulation in E. histolytica. Annu Rev Microbiol. — Search PubMed.
Live PubMed Searches
- Amoebiasis metronidazole tinidazole treatment
- Amoebiasis paromomycin luminal amebicide
- Amebic liver abscess medical treatment
- Entamoeba histolytica asymptomatic treatment
Connections
- All Parasites
- Metronidazole and Tissue Amebicides
- Liver Abscess Drainage
- Prevention and Water Safety
- Entamoeba Symptoms Overview
- Diagnosis — Stool, Antigen, and Serology
- Entamoeba histolytica Main Page
- Infectious Disease