Amoebic Liver Abscess and Extraintestinal Disease
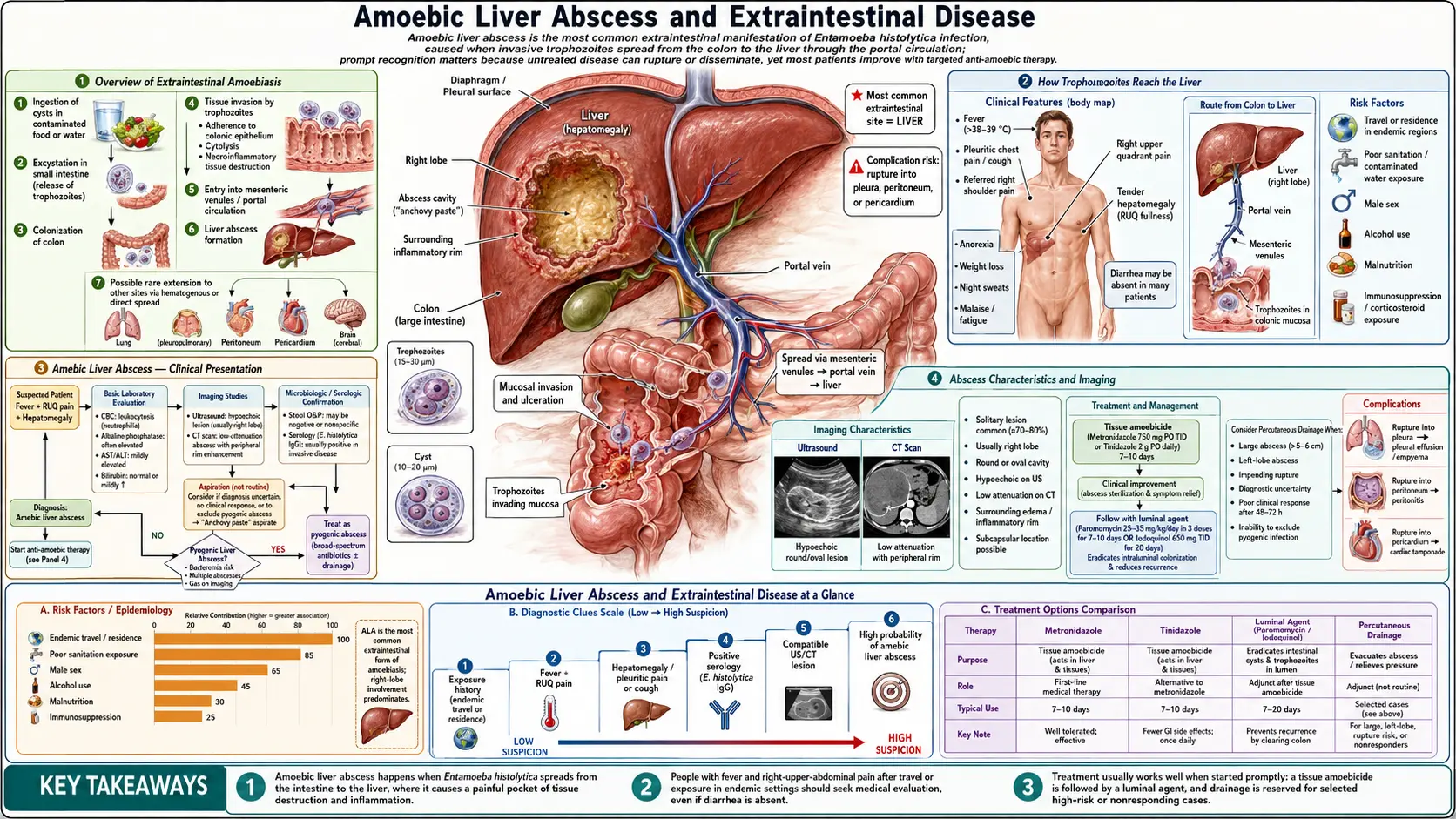
Table of Contents
- Overview of Extraintestinal Amoebiasis
- How Trophozoites Reach the Liver
- Amebic Liver Abscess — Clinical Presentation
- Abscess Characteristics and Imaging
- Why Many ALA Patients Have No GI Symptoms
- Risk Factors for Liver Abscess
- Rupture and Life-Threatening Complications
- Rare Extraintestinal Sites
- Key Research Papers
- Connections
- Featured Videos
1. Overview of Extraintestinal Amoebiasis
Extraintestinal amoebiasis occurs when Entamoeba histolytica trophozoites escape the gut wall, enter the bloodstream, and establish infection in organs beyond the intestine. The liver is overwhelmingly the most common target, accounting for the vast majority of extraintestinal cases; all other sites are comparatively rare. Amebic liver abscess (ALA) is the most important and most frequently encountered complication of invasive amoebiasis overall, not just of the extraintestinal form.
ALA is a distinct clinical syndrome from amebic colitis. The two can occur together, but they often present quite separately — a patient may develop ALA weeks to years after an episode of intestinal amoebiasis that was mild or unrecognized, and many ALA patients present without any ongoing bowel symptoms. This temporal and symptomatic separation makes ALA a diagnosis that must be actively considered in any febrile patient with right upper quadrant pain and a relevant exposure history, even in the absence of diarrhea.
2. How Trophozoites Reach the Liver
The route from gut to liver follows the anatomy of the portal circulation:
- Invasive trophozoites penetrate the mucosa of the large intestine, particularly the cecum and ascending colon.
- From the submucosal tissue they enter mesenteric venules — the small veins draining the bowel wall — and are carried into the portal vein.
- Portal blood flows directly into the liver, where trophozoites lodge in small portal venules.
- There they destroy hepatocytes and incite an inflammatory response, with progressive coalescence of necrotic zones into an abscess cavity.
The right lobe of the liver is affected in the great majority of cases — roughly 80–90% of ALA are right-sided. This reflects the streaming of blood in the portal vein: flow from the right colon (where the cecum sits) tends to stream toward the right lobe. Left-lobe abscesses, though less common, are clinically important because of their proximity to the pericardium — a left-lobe ALA that ruptures anteriorly can enter the pericardial sac, causing the most acutely life-threatening complication of amoebiasis.
3. Amebic Liver Abscess — Clinical Presentation
The onset of ALA is usually subacute over days to a few weeks. The characteristic triad is:
- Fever — typically 38–40°C, often with sweats and chills. Fever in ALA tends to be more prominent than in uncomplicated amebic colitis, where it is often low-grade.
- Right upper quadrant pain — dull, aching, and progressive. The pain can be referred to the right shoulder (diaphragmatic irritation) and may worsen with inspiration or movement. Left-lobe abscesses produce epigastric pain and may present more centrally.
- Tender hepatomegaly — the liver is enlarged and tender on palpation, often point-tender at the intercostal spaces overlying the abscess.
Systemic features include malaise, fatigue, anorexia, and weight loss. Jaundice is uncommon in ALA unless the abscess compresses biliary structures, or secondary bacterial infection has occurred. Elevated alkaline phosphatase (ALP) is the most consistent laboratory abnormality, often markedly raised. C-reactive protein (CRP) is typically very high. Transaminases (AST/ALT) are variably elevated. Leukocytosis with a neutrophil predominance is common.
4. Abscess Characteristics and Imaging
The contents of an amebic liver abscess are the classic "anchovy paste" or "chocolate sauce" — a semi-liquid, reddish-brown to dark-brown, odorless material composed of necrotic hepatocyte debris, dead trophozoites, and liquefied liver. The absence of odor distinguishes it from pyogenic bacterial abscess pus; bacterial superinfection, however, produces a foul-smelling purulent aspirate and represents a complication rather than the natural ALA state.
Ultrasound is the first-line imaging modality:
- ALA appears as a round or oval hypoechoic (dark) lesion, typically with a well-defined wall and internal echoes from debris.
- Most abscesses are solitary (single large cavity), though multiple abscesses occur in roughly 10–20% of cases.
- Right lobe, posterior segment involvement is most common.
CT scan provides additional detail about lobe involvement, proximity to major vessels and bile ducts, and evidence of rupture into adjacent structures — particularly useful when drainage is being planned or complications are suspected.
The combination of a compatible clinical picture + right-lobe hypoechoic lesion on ultrasound + positive serology (see Diagnosis page) is sufficient to initiate treatment in most settings without waiting for needle aspiration to confirm the diagnosis. Aspiration is reserved for specific clinical indications (see the Liver Abscess Drainage page).
5. Why Many ALA Patients Have No GI Symptoms
Epidemiological studies consistently show that up to 70% of patients presenting with amebic liver abscess have no concurrent diarrhea, and many have no history of intestinal symptoms at all. This appears paradoxical — how can the liver be infected without gut involvement? Several mechanisms explain this:
- Temporal separation: Intestinal invasion may have been mild, transient, or even subclinical months to years earlier. By the time ALA presents, the bowel infection may have resolved spontaneously while a few trophozoites that reached the liver have been silently expanding.
- Asymptomatic intestinal carriage at time of presentation: Some patients have ongoing intestinal colonization without symptoms; stool antigen testing or PCR at the time of ALA presentation may be positive even without diarrhea.
- Low stool positivity rate: At the time of ALA presentation, stool examination for trophozoites or cysts is positive in only 10–40% of patients — partly because the intestinal phase may be winding down, and partly because stool-cyst shedding is intermittent.
The clinical implication is clear: the absence of diarrhea must never be used to exclude ALA. Any febrile patient with right upper quadrant pain and a risk-factor history (travel, endemic residence, MSM, immunosuppression) deserves hepatic imaging and amoebiasis serology regardless of bowel symptoms.
6. Risk Factors for Liver Abscess
Not all patients with E. histolytica infection progress to ALA. Several host factors strongly influence this risk:
- Male sex: ALA is 7–12 times more common in men than women in most series. The reason is incompletely understood but may involve hormonal influences on hepatic immune responses; animal model data suggest estrogen is protective via effects on hepatic macrophage activity.
- Alcohol use: Heavy alcohol consumption impairs hepatic macrophage (Kupffer cell) function and is consistently associated with increased ALA risk and larger abscess size.
- Malnutrition: Severe malnutrition impairs innate immune defenses at multiple levels and is associated with both more frequent and more severe amebic disease.
- Age: ALA most commonly affects men aged 20–50 years in endemic regions. Children and the elderly are less commonly affected but may have more severe outcomes.
- HIV and immunosuppression: Although classical series describe ALA as occurring in immunocompetent individuals, immunosuppression from any cause increases risk and may impair response to treatment.
- Travel: Travelers from non-endemic countries who visit endemic regions are at risk during travel; ALA may not manifest until weeks to months after return, when the index of suspicion has dropped.
7. Rupture and Life-Threatening Complications
Untreated or late-diagnosed ALA can rupture into adjacent structures. The direction of rupture and the target structure determine the clinical presentation and prognosis:
- Pleuropulmonary rupture (most common complication): Right-lobe abscesses adjacent to the dome of the liver can rupture through the diaphragm into the right pleural space, producing a right-sided pleural effusion or empyema (pus in the pleural space). Further extension into the right lung parenchyma produces hepatobronchial fistula — a dramatic presentation where the patient coughs up "chocolate sauce" material. Surprisingly, this complication often responds well to medical treatment alone if identified promptly.
- Pericardial rupture (most lethal complication): Left-lobe ALA can rupture anteriorly into the pericardial sac, causing acute cardiac tamponade. This is an emergency requiring simultaneous antiparasitic therapy and pericardiocentesis. Mortality is high even with aggressive management. Left-lobe location is an indication for prophylactic drainage even in asymptomatic patients with a large abscess.
- Intraperitoneal rupture: An abscess rupturing through the liver capsule into the peritoneal cavity produces feculent or amebic peritonitis requiring emergency surgical washout alongside medical therapy.
- Secondary bacterial infection: Superinfection of the abscess cavity with enteric bacteria produces pyogenic ALA on top of amebic ALA, changing the clinical picture dramatically and usually mandating drainage in addition to antibiotics plus antiparasitic drugs.
8. Rare Extraintestinal Sites
Beyond the liver and its direct neighbors, E. histolytica can disseminate hematogenously to other organs:
- Cerebral amoebiasis: The most feared rare complication. Trophozoites reach the brain via systemic blood flow from the liver. Presentation is a rapidly progressive space-occupying lesion with fever, headache, focal neurological deficits, and seizures — a picture similar to bacterial brain abscess or high-grade CNS tumor. Imaging shows a ring-enhancing lesion. Mortality is very high because the diagnosis is rarely made in time; most cases are identified post-mortem or found coincidentally at surgery for what was thought to be a bacterial or fungal brain abscess.
- Pulmonary amoebiasis without hepatic involvement: Primary pulmonary amoebiasis without the hepatic route is possible but very rare; most pulmonary disease is secondary to hepatic ALA rupture.
- Cutaneous and genitourinary amoebiasis: Perianal and perineal skin lesions can occur through direct extension from a perforated rectal ulcer. Penile or vulvar amoebiasis has been reported, typically via fistulous tracks from pelvic disease or through sexual contact.
- Splenic, renal, and cardiac amoebiasis: Individually case-report-level rarities representing end-stage hematogenous seeding in severely immunocompromised patients or in the setting of untreated disseminated disease.
9. Key Research Papers
Selected peer-reviewed literature on amebic liver abscess and extraintestinal amoebiasis.
- Haque R et al. Amebiasis. N Engl J Med. — Search PubMed.
- Shirley DT et al. Global burden and therapeutics for amebiasis. Open Forum Infect Dis. — Search PubMed.
- Petri WA Jr et al. Enteric infection and dehydration. Sci Transl Med. — Search PubMed.
- Bercu TE et al. Amebic colitis — new insights. Curr Gastroenterol Rep. — Search PubMed.
- Moonah SN et al. Amebiasis pathogenesis. PLoS Pathog. — Search PubMed.
- Espinosa-Cantellano M, Martínez-Palomo A. Pathogenesis of intestinal amebiasis. Clin Microbiol Rev. — Search PubMed.
- Blessmann J et al. Epidemiology, diagnosis, and treatment of liver abscess. Clin Microbiol Infect. — Search PubMed.
- Fotedar R et al. Laboratory diagnostics for Entamoeba species. Clin Microbiol Rev. — Search PubMed.
- Shirley DT, Watanabe K, Moonah S. Significance of amebiasis. PLoS Negl Trop Dis. — Search PubMed.
- Marie C, Petri WA Jr. Virulence regulation in E. histolytica. Annu Rev Microbiol. — Search PubMed.
Live PubMed Searches
- Amebic liver abscess treatment
- Amebic liver abscess rupture pericardium
- Entamoeba histolytica extraintestinal dissemination
- Amebic pleuropulmonary hepatobronchial fistula
Connections
- All Parasites
- Entamoeba Symptoms Overview
- Amoebic Dysentery and Colitis
- Diagnosis — Stool, Antigen, and Serology
- Liver Abscess Drainage
- Metronidazole and Tissue Amebicides
- Entamoeba histolytica Main Page
- Nephrology & Hepatology