Severe Babesiosis: Life-Threatening Disease in Vulnerable Patients
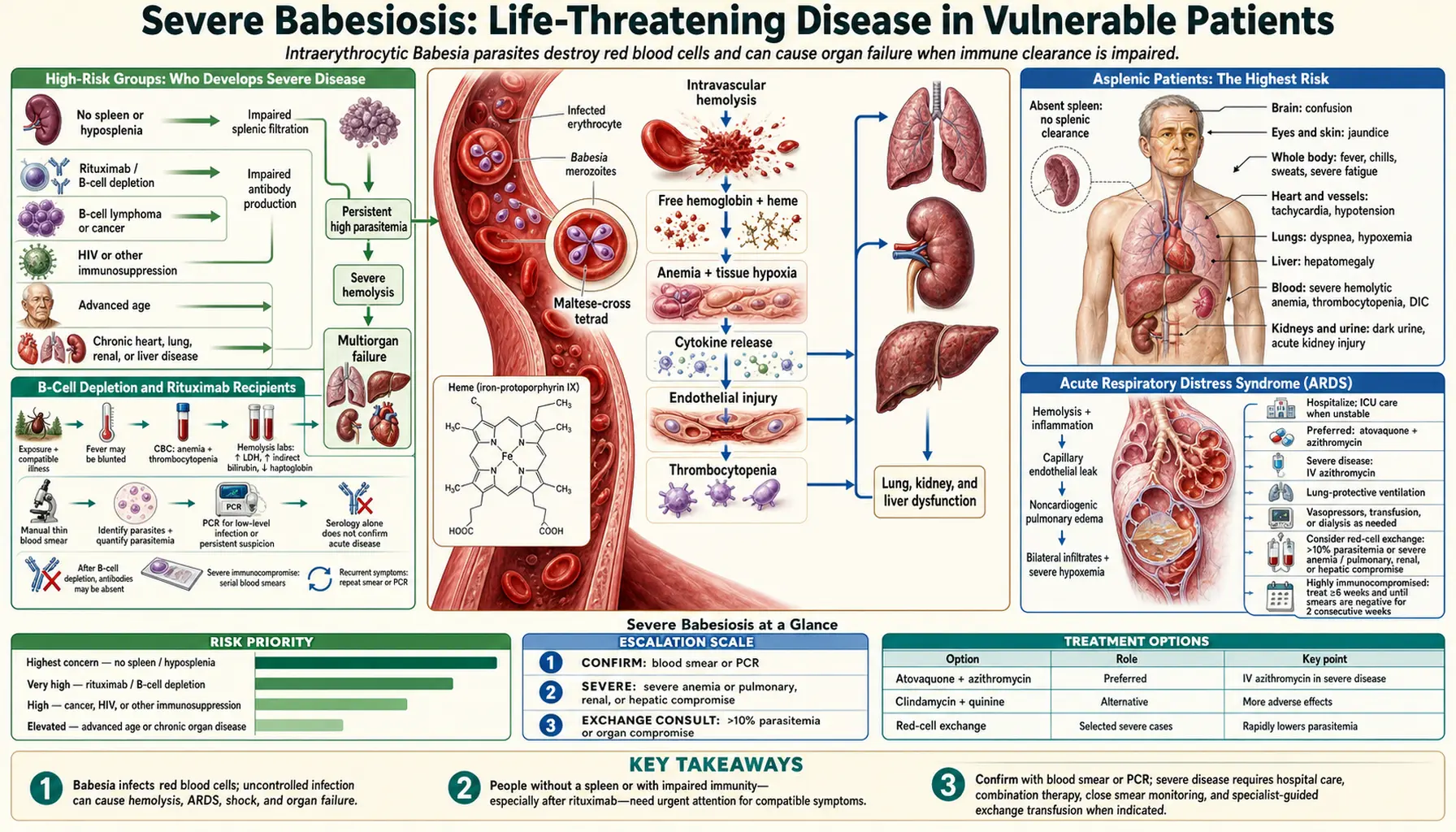
Most people with babesiosis get a bad flu-like illness and recover. But for a small and predictable group of patients — those without a spleen, those on immune-suppressing medications, those with HIV, and the elderly — babesiosis is a medical emergency. Parasitemia can climb to levels that destroy the majority of red blood cells in the body. Organs fail. Exchange transfusion becomes necessary. Intensive care is required. This page explains who is at risk, what goes wrong inside their bodies, and what the ICU management looks like.
Table of Contents
- High-Risk Groups: Who Develops Severe Disease
- Asplenic Patients: The Highest Risk
- B-Cell Depletion and Rituximab Recipients
- Acute Respiratory Distress Syndrome (ARDS)
- Renal Failure: Hemoglobin Poisoning the Kidneys
- Disseminated Intravascular Coagulation (DIC)
- Splenic Rupture: A Rare Emergency
- Persistent and Relapsing Babesiosis
- Transfusion-Transmitted Babesiosis in the US
- Pathophysiology: How Parasites Block Tiny Blood Vessels
- ICU Management Overview
- Key Research Papers
- Connections
- Featured Videos
1. High-Risk Groups: Who Develops Severe Disease
Severe babesiosis is not random. It is concentrated in identifiable patient populations whose immune systems are impaired in specific ways that prevent them from controlling intraerythrocytic parasites. Knowing these risk factors allows clinicians to triage patients appropriately: a 35-year-old immunocompetent patient with mild babesiosis can often be managed as an outpatient with close telephone follow-up; an asplenic 68-year-old with any degree of symptomatic babesiosis should be hospitalized.
The core risk factors for severe babesiosis are: absence of a functional spleen (surgical splenectomy or functional asplenia from sickle cell disease or thalassemia major); B-cell immunodeficiency or depletion (from rituximab, B-cell lymphoma, common variable immunodeficiency, or other causes); HIV/AIDS particularly with CD4 counts below 200/μL; age greater than 50 years (with risk increasing progressively with age); organ transplant recipients on maintenance immunosuppression; and patients with malignancy or on systemic chemotherapy.
A parasitemia level above 4% is typically used as a clinical marker for severe disease and usually indicates hospitalization. Parasitemia above 10% often prompts consideration of exchange transfusion, particularly in asplenic patients. In immunocompetent patients, parasitemia rarely exceeds 10%; in asplenic patients, it can exceed 80% — meaning more than 4 out of 5 red blood cells in the body are infected.
2. Asplenic Patients: The Highest Risk
The spleen performs two functions that are absolutely critical for controlling intraerythrocytic parasites: physical filtration and immune orchestration. Surgically asplenic patients have neither. Patients with functional asplenia from sickle cell disease retain an intact spleen but it has become fibrotic and non-functional from repeated vaso-occlusive episodes — they are physiologically equivalent to surgically asplenic patients for the purpose of Babesia risk.
The spleen filters parasitized red blood cells because those cells are stiffer and less deformable than normal RBCs (the parasite changes the cell's structural proteins). The spleen's sinusoidal architecture forces cells to squeeze through narrow gaps; parasitized cells cannot do this and are trapped, then phagocytosed by splenic macrophages. Without this filtration, parasitized RBCs complete their full replication cycle unchecked, each bursting to release four new merozoites that immediately invade four new cells. The exponential growth of parasitemia in asplenic patients reflects the absence of this bottleneck.
Documented cases of babesiosis in asplenic patients have reached parasitemia levels of 80% and above — nearly every red blood cell in the body infected. At these levels, the patient is in multi-organ failure from combined effects of anemia so severe the tissues cannot receive adequate oxygen, massive free hemoglobin from lysing cells poisoning the kidneys, and cytokine storm from the scale of the immune response. Death can occur within 24–48 hours of presentation if exchange transfusion is not performed urgently and antiparasitic treatment is not initiated immediately.
For asplenic patients living in endemic areas (northeastern US, upper Midwest), the standard of care includes counseling about Babesia risk, instruction to seek immediate medical evaluation for any febrile illness during tick season, and wearing DEET/permethrin-treated clothing when outdoors. Some infectious disease specialists recommend wearing a medical alert bracelet identifying asplenic status.
3. B-Cell Depletion and Rituximab Recipients
Rituximab is a monoclonal antibody against the CD20 protein on B cells, widely used to treat B-cell lymphomas, rheumatoid arthritis, and certain autoimmune diseases. It depletes circulating B lymphocytes for months to years after treatment. B cells are the source of antibodies, and antibody responses are critical for clearing Babesia once initial parasitemia is controlled by cellular immune mechanisms.
Patients who have received rituximab and develop babesiosis face a specific and serious problem: persistent and relapsing infection. Even with an adequate course of atovaquone/azithromycin that reduces parasitemia to undetectable levels on smear, the parasite can persist at low levels detectable only by PCR, and then rebound when treatment is discontinued. This happens because the antibody response that normally consolidates parasite clearance is absent.
The clinical definition of relapsing/refractory babesiosis is persistent or recurring parasitemia after at least 6 weeks of treatment. Management of refractory babesiosis in B-cell-depleted patients is challenging: extended treatment regimens are required, typically 6 weeks or longer, guided by serial PCR testing every 2–4 weeks rather than by clinical symptoms alone (since PCR can detect low-level parasitemia that is asymptomatic). Some patients require treatment durations of 3–6 months before PCR becomes consistently negative.
Patients with B-cell lymphoma who are receiving active chemotherapy face a compound risk: both the lymphoma itself and the chemotherapy suppress immunity, and the timing of babesiosis exposure during an already immunosuppressed state can lead to rapidly progressive disease. Clinicians managing cancer patients in endemic areas should include babesiosis in the differential diagnosis of any febrile, anemic cancer patient during tick season.
4. Acute Respiratory Distress Syndrome (ARDS)
Acute respiratory distress syndrome is the most common severe organ manifestation of babesiosis and one of the primary causes of death in critically ill patients. ARDS in babesiosis develops through two concurrent mechanisms that amplify each other: microvascular obstruction by parasitized RBCs and cytokine-driven lung injury.
Parasitized RBCs are stiffer and less deformable than normal cells, and they display altered surface proteins that promote adhesion to the vascular endothelium of small pulmonary vessels. This cytoadherence — a mechanism also seen in severe Plasmodium falciparum malaria — causes parasitized cells to lodge in pulmonary capillaries, blocking blood flow and oxygen exchange. The consequence is hypoxemia despite normal airway anatomy, because the problem is at the level of the pulmonary capillaries, not the alveoli or airways.
Simultaneously, the massive immune response to widespread parasitemia triggers a cytokine storm: TNF-alpha, IL-6, IL-1, and other inflammatory mediators are produced in enormous quantities. These cytokines increase the permeability of the pulmonary endothelium, allowing protein-rich fluid to leak from pulmonary capillaries into the alveolar space. The alveoli fill with fluid (non-cardiogenic pulmonary edema), destroying their ability to exchange oxygen. This is the hallmark of ARDS.
Patients with babesiosis-associated ARDS present with rapidly worsening dyspnea, falling oxygen saturation on pulse oximetry, bilateral infiltrates on chest X-ray, and hypoxemia that does not correct with supplemental oxygen alone. Many require mechanical ventilation. The treatment is antiparasitic therapy to address the underlying cause combined with lung-protective ventilation strategies (low tidal volumes, positive end-expiratory pressure) to support oxygenation while the infection is brought under control.
5. Renal Failure: Hemoglobin Poisoning the Kidneys
Acute kidney injury (AKI) is a common complication of severe babesiosis, developing through two distinct but often simultaneous mechanisms: pigment nephropathy from free hemoglobin and direct glomerular injury from the systemic inflammatory response.
Pigment nephropathy begins with massive hemolysis. When parasitized RBCs lyse in large numbers, they release their hemoglobin content directly into the plasma. Under normal circumstances, a plasma protein called haptoglobin binds free hemoglobin and carries it safely to the liver for recycling. But in severe babesiosis, the rate of hemolysis overwhelms the supply of haptoglobin, and free hemoglobin accumulates in plasma (hemoglobinemia) and spills into the urine (hemoglobinuria — the "coca-cola urine" that patients notice). As free hemoglobin passes through the renal tubules, it precipitates, forming casts that physically obstruct tubular flow. Free heme (released from hemoglobin breakdown) is also directly toxic to tubular epithelial cells, causing oxidative damage and cell death.
The result is acute tubular necrosis — the most common form of intrinsic AKI. Laboratory findings include rising creatinine and BUN, a fall in urine output, and urine microscopy showing muddy brown granular casts (the hallmark of tubular injury). In severe cases, anuria develops and dialysis may be required.
Direct glomerular injury from immune complex deposition and cytokine-mediated endothelial damage adds a second pathway to kidney injury. Immune complexes containing Babesia antigens and host antibodies can deposit in glomerular capillaries, triggering complement activation and inflammatory injury. This membranoproliferative pattern of glomerular injury is less common than tubular injury but contributes to the overall kidney damage in severe cases.
Prevention of AKI in babesiosis relies on the same measures that work for other pigment nephropathy syndromes: aggressive intravenous hydration (to dilute tubular hemoglobin concentrations and maintain urine flow) combined with rapid antiparasitic treatment to stop the ongoing hemolysis. Exchange transfusion also reduces AKI risk by rapidly removing parasitized RBCs before they can lyse and release more hemoglobin.
6. Disseminated Intravascular Coagulation (DIC)
Disseminated intravascular coagulation (DIC) is a paradoxical coagulation disorder that causes both inappropriate clotting throughout the vasculature and simultaneous bleeding. It occurs in severe babesiosis through the systemic activation of the clotting cascade triggered by the massive cytokine release accompanying high-grade parasitemia and rapid RBC lysis.
In DIC, tissue factor — normally sequestered inside cells — is exposed at massive scale when cells (including RBCs) lyse and die. Tissue factor activates the extrinsic coagulation pathway, generating thrombin throughout the vasculature. Thrombin converts fibrinogen to fibrin, and fibrin microthrombi form in small blood vessels throughout multiple organ systems simultaneously. These microthrombi impair blood flow to organs (contributing to the multi-organ failure of severe babesiosis) and also consume clotting factors and platelets faster than the liver and bone marrow can replace them.
The clinical picture of DIC is therefore: laboratory evidence of coagulopathy (prolonged PT, prolonged PTT, falling fibrinogen, elevated D-dimer and fibrin degradation products), combined with thrombocytopenia (already present in babesiosis from platelet consumption in the spleen and immune destruction) and, in advanced DIC, spontaneous bleeding from venipuncture sites, mucosal surfaces, or gastrointestinal tract. Management involves treating the underlying cause (antiparasitic therapy for babesiosis), supporting with fresh frozen plasma (FFP) to replenish clotting factors, and transfusing platelets when counts fall below 10,000–20,000/μL or when the patient is actively bleeding.
7. Splenic Rupture: A Rare Emergency
Splenic rupture is a rare but life-threatening complication of babesiosis. The spleen enlarges (splenomegaly) as it attempts to filter the increasing numbers of parasitized RBCs from the circulation. An enlarged spleen has a larger, more fragile parenchyma with a capsule under greater tension. Physical trauma — even minor, such as a cough, sneeze, or turning over in bed — can cause the capsule to tear and the spleen to rupture, producing rapid intraperitoneal hemorrhage.
Spontaneous splenic rupture (without antecedent trauma) has been reported in babesiosis. The clinical presentation is sudden onset of severe left upper quadrant or left shoulder pain (Kehr's sign, from diaphragmatic irritation by blood), hemodynamic instability (tachycardia, hypotension, pallor), and a rapidly falling hemoglobin. Ultrasound confirms free fluid in the peritoneum; CT scan of the abdomen characterizes the extent of splenic injury.
Management of splenic rupture in babesiosis requires simultaneous antiparasitic treatment (the underlying infection must be controlled to prevent recurrence) and surgical or radiological management of the hemorrhage. Splenectomy (surgical removal of the ruptured spleen) is the traditional approach for hemodynamically unstable patients. Splenic artery embolization is an option for hemodynamically stable patients with appropriate injury patterns. The paradox of splenic rupture in babesiosis is that splenectomy removes the spleen that has been protecting the patient against Babesia, potentially converting a patient with moderate parasitemia into an asplenic patient with the attendant risk of rapidly escalating parasitemia — requiring immediate post-splenectomy antiparasitic therapy and close parasitemia monitoring.
8. Persistent and Relapsing Babesiosis
Standard antiparasitic therapy for babesiosis is effective in most patients, clearing parasitemia and resolving symptoms within 1–2 weeks. But in a subset of immunocompromised patients — particularly those with B-cell deficiencies who cannot mount an antibody response — the parasite is never fully cleared. After an initial clinical response, parasitemia rebounds when treatment is discontinued, or the patient develops symptomatic relapse weeks to months later.
Persistent babesiosis is formally defined as parasitemia detectable by PCR for more than 3 months, or recurring symptoms after treatment with documented parasitemia on PCR or smear. The key patients at risk are: rituximab recipients (B-cell depleted), patients with B-cell lymphoma, patients with common variable immunodeficiency (CVID), patients with HIV/AIDS and low CD4 counts, and patients receiving other immunosuppressive regimens that specifically target B-cell function.
Management of persistent babesiosis requires longer treatment durations, often 6 weeks or longer, and should be guided by serial PCR testing rather than clinical symptoms alone. The reason PCR monitoring is essential is that patients may become symptom-free while still harboring detectable parasitemia; stopping treatment at symptom resolution in these patients leads to clinical relapse. The goal of treatment is two consecutive negative PCR tests 2–4 weeks apart before therapy is discontinued. Some patients require treatment for 3–6 months.
For patients on rituximab who develop persistent babesiosis, the options are limited: the rituximab cannot always be safely discontinued (it may be keeping a life-threatening lymphoma in remission), and alternative anti-Babesia regimens have limited evidence. Extended atovaquone/azithromycin treatment is the standard approach, with clindamycin/quinine considered for treatment failures. Infectious disease specialist involvement is essential.
9. Transfusion-Transmitted Babesiosis in the US
Transfusion-transmitted babesiosis is the most frequently reported transfusion-transmitted parasitic infection in the United States, with over 250 confirmed cases reported to the CDC. The actual number is substantially higher, as many cases go undiagnosed or are not reported. Babesia microti can survive in stored red blood cells, platelets, and fresh frozen plasma under standard blood bank refrigeration for the duration of the typical storage period (up to 42 days for packed red cells).
The mechanism is straightforward: an asymptomatic donor in an endemic area donates blood while unknowingly parasitemic. The stored blood product is transfused to a recipient — who is typically immunocompromised, elderly, or otherwise medically fragile. The recipient's immune system is unable to control the parasitemia effectively, and babesiosis develops 1–9 weeks after the transfusion.
The FDA approved the first nucleic acid test (NAT) screening assay for Babesia in blood donations in 2019, enabling direct detection of B. microti DNA in donor blood. Several high-burden states (including New York, Connecticut, Massachusetts, Minnesota, and Wisconsin) implemented this screening in 2019–2020, and early data show significant reductions in transfusion-transmitted cases from screened states. However, screening is not yet universal across all US blood collection centers, and the approved assay targets primarily B. microti — potentially missing B. duncani or other species.
Clinicians evaluating immunocompromised or elderly patients with unexplained fever and hemolytic anemia should ask specifically about recent blood transfusions. The 1–9 week incubation period means the connection to a transfusion is not always clinically obvious, particularly when the transfusion occurred weeks before symptoms began.
10. Pathophysiology: How Parasites Block Tiny Blood Vessels
Beyond hemolysis, Babesia damages multiple organ systems through a mechanism shared with severe falciparum malaria: cytoadherence of parasitized red blood cells to vascular endothelium, causing microvascular obstruction.
Parasitized RBCs undergo profound structural changes. The parasite exports proteins to the RBC membrane that alter its surface characteristics: the cell becomes less deformable (stiffer), develops surface knob-like protrusions displaying parasite-derived adhesion molecules, and expresses altered surface antigens that promote binding to endothelial receptors. In the microcirculation — where capillary diameters are close to or smaller than the RBC diameter, requiring cells to deform to pass through — these stiffer, cytoadherent parasitized RBCs become lodged.
The organs most vulnerable to microvascular obstruction are those with high-density microvascular beds and high metabolic oxygen demands: the lungs (hence ARDS), the kidneys (contributing to AKI), the brain (potentially causing confusion, seizures, or coma in severe cases), and the heart (contributing to cardiac failure in extreme parasitemia). This multi-organ vulnerability explains why severe babesiosis presents as multi-organ failure rather than as an isolated hematological problem.
The cytokine storm that accompanies high-grade parasitemia amplifies this vascular injury. TNF-alpha and other pro-inflammatory cytokines increase endothelial permeability, exacerbating the leakage of fluid into tissues (contributing to pulmonary edema in the lungs and general third-spacing). They also upregulate the expression of endothelial adhesion molecules, further promoting the lodging of parasitized cells. The combination of mechanical obstruction from stiff parasitized cells and cytokine-driven endothelial dysfunction creates a pathological cycle that, without treatment, progresses to irreversible organ failure.
11. ICU Management Overview
Patients with severe babesiosis require intensive care unit management addressing multiple simultaneous organ-level problems while antiparasitic therapy attacks the underlying cause. The general approach includes:
- Antiparasitic therapy: Clindamycin plus quinine (IV/oral) for severe disease — more effective than atovaquone/azithromycin in high-parasitemia disease. Do not wait for species confirmation before starting treatment if clinical and smear/PCR findings are consistent with babesiosis.
- Exchange transfusion: Indicated when parasitemia exceeds 10%, when there is severe hemolysis with organ failure, or in asplenic patients with rapidly deteriorating course. Exchange transfusion physically removes parasitized RBCs and replaces them with donor cells, rapidly reducing parasitemia and removing mediators of hemolysis and inflammation.
- Oxygen support and mechanical ventilation: For ARDS. Lung-protective ventilation with low tidal volumes (6 mL/kg ideal body weight) and adequate PEEP to maintain oxygenation.
- Renal replacement therapy: Continuous renal replacement therapy (CRRT) or intermittent hemodialysis for patients with severe AKI, anuria, or fluid overload complicating respiratory management.
- Coagulopathy management: FFP for DIC-related coagulopathy, platelet transfusion for severe thrombocytopenia with active bleeding.
- Intravenous hydration: Aggressive IV fluids to maintain urine output and dilute tubular hemoglobin concentrations, balanced against the risk of fluid overload in patients with concurrent ARDS or cardiac dysfunction.
- Serial parasitemia monitoring: Blood smear and PCR every 24–48 hours during the acute phase to confirm response to treatment and guide exchange transfusion decisions.
Most patients who survive the acute severe phase make full recoveries, though anemia and fatigue may persist for weeks as the bone marrow restores the depleted red cell mass. Follow-up PCR testing at 4–6 weeks after treatment completion confirms parasitological cure in immunocompetent patients; immunocompromised patients require longer and more frequent follow-up.
Key Research Papers
Critical studies on severe babesiosis, immunocompromised presentations, and ICU management.
- Hatcher JC, Greenberg PD, Antique J, Jimenez-Lucho VE. Severe babesiosis in Long Island: review of 34 cases and their complications. Clin Infect Dis. 2001;32(8):1117–1125. PMID: 11283800
- Krause PJ, Gewurz BE, Hill D, et al. Persistent and relapsing babesiosis in immunocompromised patients. Clin Infect Dis. 2008;46(3):370–376 — Search PubMed
- Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366(25):2397–2407 — Search PubMed
- Leiby DA. Transfusion-transmitted Babesia spp.: bull's-eye on Babesia microti. Clin Microbiol Rev. 2011;24(1):14–28 — Search PubMed
- Herwaldt BL, Linden JV, Bosserman E, Young C, Olkowska D, Wilson M. Transfusion-associated babesiosis in the United States: a description of cases. Ann Intern Med. 2011;155(8):509–519 — Search PubMed
- Gubernot DM, Lucey CT, Lee KC, Conley GB, Holness LG, Wise RP. Babesia infection through blood transfusions: reports received by the US FDA, 1997–2007. Clin Infect Dis. 2009;48(1):25–30. PMID: 19035776
- Bloch EM, Kumar S, Krause PJ. Persistence of Babesia microti infection in humans. Pathogens. 2019;8(1):11 — Search PubMed
- Lobo CA, Rodriguez M, Cursino-Santos JR. Babesia and red cell invasion. Curr Opin Hematol. 2012;19(3):170–177 — Search PubMed
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis. Clin Infect Dis. 2006;43(9):1089–1134 — Search PubMed
- Vannier EG, Diuk-Wasser MA, Ben Mamoun C, Krause PJ. Babesiosis. Infect Dis Clin North Am. 2015;29(2):357–370 — Search PubMed
Live PubMed Searches
- Severe babesiosis asplenic/splenectomy
- Babesia immunocompromised relapsing persistent
- Babesiosis ARDS respiratory failure
- Babesia transfusion blood donor screening
- Babesiosis exchange transfusion ICU
- Babesia rituximab B-cell depletion
Connections
- All Parasites
- Babesia Overview
- Babesia Symptoms Hub
- Hemolytic Anemia & Flu Symptoms
- Diagnosis: Blood Smear & PCR
- Babesia Treatments Hub
- Atovaquone & Azithromycin Treatment
- Exchange Transfusion & Severe Disease
- Tick Prevention & Environmental Control
- Hematology
- Lyme Disease
- Malaria
- Babesiosis — the main disease overview behind these severe presentations.