Babesia Hemolytic Anemia: Fever, Chills, and Red Cell Destruction
Hemolytic anemia is the defining pathological feature of babesiosis. Whether the infection is mild enough to be managed at home or severe enough to require intensive care, the destruction of red blood cells by the Babesia parasite is always occurring. Understanding how Babesia invades, replicates inside, and destroys red cells — and what that process produces as symptoms and laboratory findings — is the key to recognizing this disease and distinguishing it from malaria, influenza, and other causes of febrile hemolytic anemia.
Table of Contents
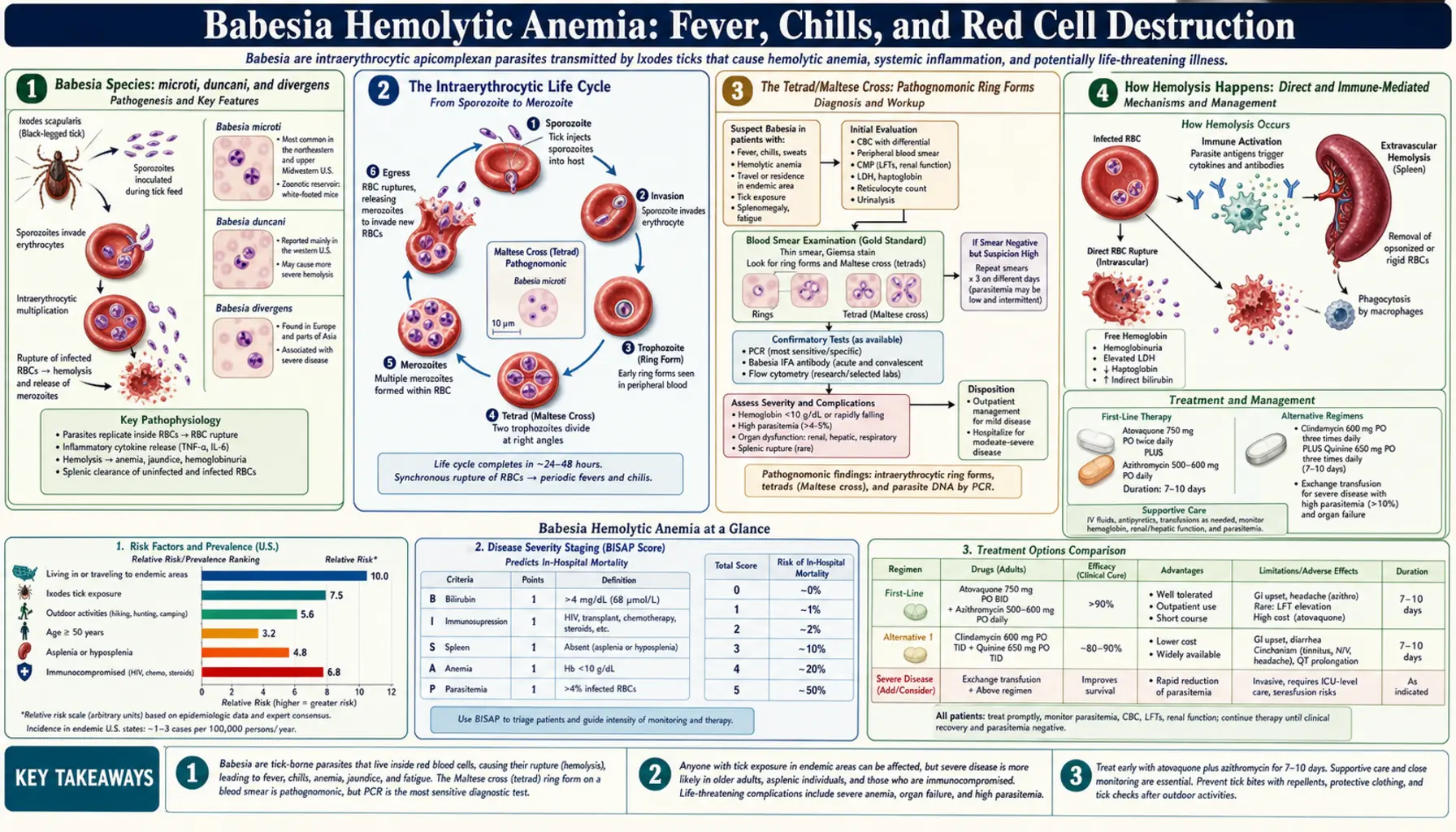
- Babesia Species: microti, duncani, and divergens
- The Intraerythrocytic Life Cycle
- The Tetrad/Maltese Cross: Pathognomonic Ring Forms
- How Hemolysis Happens: Direct and Immune-Mediated
- The Flu-Like Prodrome: Fever, Rigors, and Myalgia
- Hemoglobinuria: The Coca-Cola Urine Sign
- Laboratory Findings: What the Blood Work Shows
- Splenomegaly: The Spleen's Losing Battle
- Concurrent Lyme Disease: Amplified Symptoms
- Incubation Period and Timing of Symptom Onset
- Key Research Papers
- Connections
- Featured Videos
1. Babesia Species: microti, duncani, and divergens
Babesia microti is the dominant human pathogen in North America, responsible for the overwhelming majority of babesiosis cases diagnosed in the United States. It is transmitted by Ixodes scapularis, the black-legged (deer) tick, across the northeastern states (Maine south to New Jersey, particularly Massachusetts, Connecticut, Rhode Island, New York) and the upper Midwest (Wisconsin, Minnesota). B. microti is considered the mildest human Babesia species, though it can still cause severe and fatal disease in vulnerable patients.
Babesia duncani is the second confirmed human pathogen in North America, found along the West Coast — California, Washington, and Oregon. It causes clinically more severe hemolysis than B. microti, and published case reports include fatal outcomes in patients who did not have the classic risk factors (asplenia or immunocompromise). This makes B. duncani the more dangerous species to encounter in the western United States. Clinicians in California, in particular, should be aware that a patient presenting with tick-bite exposure and hemolytic anemia may have a more aggressive organism than the northeastern B. microti.
Babesia divergens is the primary human pathogen in Europe, transmitted by Ixodes ricinus. It is dramatically more virulent than either North American species. In asplenic patients — who have no spleen to filter parasitized red cells — B. divergens infection is frequently fatal within 24–48 hours of symptom onset if treatment is delayed. Even in patients with intact spleens, B. divergens causes higher parasitemia and more severe organ involvement than B. microti. Published case fatality rates for B. divergens in asplenic European patients exceed 40% in older series, though aggressive treatment and exchange transfusion have improved outcomes in more recent reports. Species identification therefore matters clinically: a European traveler presenting with hemolytic fever after a tick bite in France or the Netherlands requires a different index of suspicion than a Massachusetts hiker.
Additional rare human-pathogenic species include Babesia venatorum (formerly EU1, found in Europe) and Babesia sp. MO1 (reported from Missouri). As molecular diagnostic tools improve, additional species are likely to be identified as human pathogens.
2. The Intraerythrocytic Life Cycle
Babesia is an obligate intraerythrocytic parasite. Unlike many other protozoan parasites that cycle through multiple tissue compartments, Babesia targets red blood cells almost exclusively during its asexual replication phase in humans. This extreme specificity for RBCs is what makes hemolytic anemia the central feature of babesiosis and what distinguishes it biologically from malaria (which has both hepatic and erythrocytic stages) and from Lyme disease (which targets connective tissue).
The life cycle begins when an infected Ixodes tick injects sporozoites into the bloodstream during a blood meal. Sporozoites attach rapidly to the surface of red blood cells via specific ligand-receptor interactions involving the RBC surface glycoprotein glycophorin A. This attachment is remarkably efficient: B. microti merozoites can invade RBCs within seconds of contact in vitro. After invasion, the parasite is enclosed in a parasitophorous vacuole within the RBC cytoplasm.
Inside the RBC, the parasite undergoes asexual replication by binary fission — dividing once to form two merozoites, then twice to form four merozoites. This process takes approximately 8–12 hours for B. microti at physiological temperature. When division is complete, the four daughter merozoites are arranged in a characteristic tetrad configuration. The RBC membrane then ruptures (a process called egress), releasing the merozoites into the plasma, where they rapidly invade new RBCs and repeat the cycle.
Each burst of merozoite release from a cohort of synchronously infected RBCs produces a spike of fever — not from the direct parasitic activity, but from the inflammatory mediators (cytokines, particularly TNF-alpha and IL-6) released by the host immune system in response to the debris from lysed RBCs and to parasite antigens released into the bloodstream. This is why babesiosis fever, like malaria fever, can be periodic and cyclical, though the cycles are often less precisely timed than the classic tertian or quartan fever patterns of Plasmodium.
3. The Tetrad/Maltese Cross: Pathognomonic Ring Forms
The tetrad form — four merozoites joined at their apices within a single red blood cell, visually resembling a Maltese cross — is the most specific finding in babesiosis and is considered pathognomonic for B. microti on peripheral blood smear. No other human intraerythrocytic parasite produces this formation, which makes it one of the most diagnostically useful single morphological findings in infectious disease medicine.
Identifying the tetrad on smear requires Giemsa or Wright-Giemsa staining and an experienced microscopist. The four merozoites appear as small, pale ring forms connected by a thin chromatin bridge at their apices. The overall structure fits within a single RBC that is not enlarged (unlike Plasmodium vivax, which enlarges infected cells). The tetrad is not present in every infected cell — in fact, it may be seen in only 1–5% of parasitized cells on a given smear, because many cells contain only single ring forms or two-merozoite (paired piriform) stages.
Distinguishing Babesia ring forms from Plasmodium falciparum ring forms is critically important, since the treatments are entirely different and since both parasites circulate in RBCs as small ring forms in early infection. Key distinguishing features: Babesia has no hemozoin (malaria pigment) — the characteristic dark granular deposits seen in P. falciparum-infected cells are absent; Babesia does not enlarge infected RBCs (falciparum also does not enlarge cells, but vivax and ovale do, and their enlarged cells would not be confused with Babesia); Babesia produces extracellular merozoites — free ring forms floating outside RBCs are visible on smear and are not seen with Plasmodium; and the tetrad formation is unique to Babesia.
The sensitivity of a single blood smear for B. microti in early infection is relatively low — perhaps 60–70% — because parasitemia may be sparse at the time the smear is obtained. Repeat smears over 24–48 hours improve sensitivity. PCR is more sensitive than smear at low parasitemia levels and should be ordered simultaneously when clinical suspicion is high.
4. How Hemolysis Happens: Direct and Immune-Mediated
Babesia-driven hemolysis operates through two simultaneous pathways that compound each other: direct parasitic destruction of RBCs and indirect immune-mediated destruction of both parasitized and unparasitized cells.
The direct pathway is straightforward: when a parasitized RBC completes the intracellular replication cycle, the RBC membrane ruptures to release merozoites. This rupture destroys the host cell. Each destroyed cell releases hemoglobin, cell membrane debris, and parasite antigens into the plasma. At low parasitemia (<1%), this direct cell loss is easily compensated by the bone marrow's increased production of reticulocytes. As parasitemia rises — to 4%, 10%, or beyond — the rate of RBC destruction outpaces the bone marrow's compensatory capacity, and anemia develops and deepens.
The indirect immune-mediated pathway amplifies hemolysis beyond what direct parasitic destruction would produce alone. The host immune system mounts an inflammatory response against parasitized RBCs, involving both cellular immunity (natural killer cells, macrophages) and the complement system. Complement activation leads to deposition of complement proteins on the surface of parasitized RBCs, marking them for destruction by macrophages in the spleen and liver. This immune recognition is imprecise: bystander unparasitized RBCs can be caught up in the same process, particularly during the peak of immune activation, accounting for the fact that the degree of anemia in babesiosis often exceeds what would be predicted from the parasitemia level alone.
The direct Coombs test (direct antiglobulin test) is positive in some patients with babesiosis, confirming that immunoglobulin and/or complement is coating the patient's RBCs — a finding that documents the immune-mediated component of hemolysis. This Coombs positivity can persist even after the parasite is cleared, contributing to prolonged anemia in some patients during recovery.
5. The Flu-Like Prodrome: Fever, Rigors, and Myalgia
The clinical presentation of symptomatic babesiosis begins with a prodrome that is easily mistaken for influenza, particularly in summer and early fall months when both influenza and tick-borne diseases circulate. The onset is gradual, not abrupt — symptoms typically develop over several days, unlike the sudden onset of influenza, which usually strikes within hours. This gradual onset, combined with the summer timing (when influenza is uncommon in most years), provides a clue that the illness is not straightforward influenza.
Fever is the cardinal feature. Temperature typically rises to 38–40°C (100.4–104°F) and may be persistently elevated or, particularly later in the illness, intermittent — spiking in the afternoon or evening and partially resolving overnight. The intermittent pattern reflects the synchrony of parasite replication cycles releasing merozoites in waves, each wave triggering a cytokine spike and fever spike. In severe cases, fever may be continuous rather than intermittent.
Rigors (shaking chills) accompany fever spikes, sometimes severely. Patients often describe uncontrollable shaking that lasts 10–30 minutes, then transitions to drenching sweats as the fever breaks temporarily. This fever-rigor-sweat cycle is characteristic of parasitic hemolytic diseases (it is also seen in malaria) and differs from the milder chills typical of bacterial infections.
Myalgias — diffuse muscle aches — are prominent and often described as the most disabling symptom after the fever itself. Unlike the focused joint pains of Lyme disease, babesiosis myalgias tend to be generalized and poorly localized. Arthralgias (joint aches without actual joint swelling) also occur. Headache is common, typically frontal or generalized. Fatigue can be profound and may persist for weeks after the parasite is cleared.
Anorexia and nausea are reported in many patients. Some patients report abdominal pain, particularly left upper quadrant discomfort from splenomegaly as the spleen enlarges to filter increasing numbers of parasitized RBCs. Vomiting is less common in mild disease but occurs in more severe presentations.
6. Hemoglobinuria: The Coca-Cola Urine Sign
When RBC hemolysis exceeds the binding capacity of haptoglobin (a plasma protein that captures free hemoglobin released from lysed cells), free hemoglobin spills into the urine, producing hemoglobinuria. Patients notice that their urine turns dark — dark brown, tea-colored, or what clinicians and patients often describe as "coca-cola colored." This is an alarming and important symptom that signals significant ongoing hemolysis and often prompts patients who had been tolerating their illness at home to seek immediate medical care.
Hemoglobinuria in babesiosis is a marker of significant disease severity. It indicates that haptoglobin has been consumed (haptoglobin levels will be undetectable on laboratory testing), that free hemoglobin is now circulating in the plasma (hemoglobinemia), and that the kidneys are filtering it. This matters because free hemoglobin in high concentrations is directly toxic to renal tubular cells, and hemoglobinuria is a precursor to acute kidney injury in babesiosis — a complication more common in severe disease.
Hemoglobinuria must be distinguished from hematuria (blood in the urine from RBC breakdown within the urinary tract) and myoglobinuria (from muscle breakdown). A urine dipstick tests positive for "blood" in all three conditions (because the dipstick detects heme, not intact cells), but urine microscopy clarifies: hemoglobinuria shows no intact red cells on microscopy, while hematuria shows abundant RBCs. Myoglobinuria is distinguished by marked elevation of serum creatine kinase (CK), which is not elevated in pure hemoglobinuria from babesiosis.
7. Laboratory Findings: What the Blood Work Shows
The laboratory pattern in babesiosis is characteristic and, when recognized in a patient from an endemic area with fever and flu-like symptoms, should prompt immediate blood smear and PCR testing.
Complete Blood Count (CBC): Normocytic, normochromic anemia — hemoglobin falling progressively as the infection continues. The red cells are normal in size and color (unlike iron deficiency anemia which produces small, pale cells), reflecting the fact that the problem is destruction, not impaired production. Thrombocytopenia is present in 50–70% of symptomatic patients and can be moderate to severe (platelet counts <100,000/μL are common; <50,000/μL in severe cases). White cell count is typically normal or only mildly elevated — markedly elevated WBC should prompt consideration of a concurrent bacterial infection or anaplasmosis (which does cause leukopenia in many cases).
Reticulocyte count: Elevated, reflecting the bone marrow's attempt to compensate for RBC destruction by accelerating new RBC production. A reticulocyte count of 3–8% (normal <2%) is typical in active hemolysis. This is an important marker: a patient presenting with anemia and a high reticulocyte count has a hemolytic or hemorrhagic process, not a hypoproliferative one.
Lactate dehydrogenase (LDH): Markedly elevated. LDH is released from the cytoplasm of lysed cells — not just RBCs, but any cell that is damaged. In babesiosis, the primary source of elevated LDH is the destruction of parasitized RBCs. LDH levels correlate roughly with the degree of hemolysis and are useful for monitoring response to treatment: falling LDH confirms that hemolysis is slowing.
Haptoglobin: Low or undetectable. Haptoglobin is a plasma protein that scavenges free hemoglobin, binding it and delivering it for recycling in the liver. During active hemolysis, haptoglobin is consumed faster than it is produced, and serum levels fall. An undetectable haptoglobin is a sensitive marker of significant hemolysis. In severe babesiosis, haptoglobin is typically undetectable and may remain so for days after treatment begins.
Indirect bilirubin: Elevated. When haptoglobin is saturated and free hemoglobin reaches the liver, heme is metabolized to bilirubin. Indirect (unconjugated) bilirubin rises, sometimes causing clinical jaundice (scleral icterus, skin yellowing). Direct bilirubin may also rise slightly if there is some degree of hepatic involvement.
Liver function tests: Mildly elevated AST and ALT are common and do not indicate primary liver disease in most cases. They reflect hemolysis and the liver's processing of excess heme. Markedly elevated transaminases should prompt consideration of a co-existing liver pathology or severe systemic inflammatory response.
Peripheral blood smear (Giemsa stain): The direct visualization of parasitized RBCs with ring forms and, in some cells, the pathognomonic Maltese cross tetrad formation. Parasitemia percentage is calculated by counting the percentage of RBCs containing visible parasites.
8. Splenomegaly: The Spleen's Losing Battle
The spleen is the primary battleground in babesiosis. It performs two critical functions that are both protective and ultimately limiting: physical filtration of parasitized RBCs, and coordination of the adaptive immune response against Babesia.
Red blood cells infected with Babesia undergo structural changes — they become stiffer, less deformable, and display altered surface proteins that mark them as abnormal. The spleen's sinusoidal architecture exploits these changes: the narrow sinusoids require RBCs to deform extensively to squeeze through, and cells that cannot deform adequately (parasitized cells, old cells, damaged cells) are trapped and phagocytosed by resident macrophages. In this way, the spleen continuously removes parasitized cells from the circulation, slowing the expansion of parasitemia.
But as parasitemia rises and the rate of parasitized RBC delivery to the spleen exceeds its filtration capacity, the spleen enlarges (splenomegaly) to accommodate the increased workload. Splenic enlargement can be detected on physical examination as left upper quadrant dullness on percussion and a palpable edge below the left costal margin. Patients sometimes notice left-sided abdominal heaviness or fullness.
Splenomegaly in babesiosis carries a risk: an enlarged, engorged spleen with friable parenchyma can rupture, either spontaneously or with minimal trauma. Splenic rupture is a rare but life-threatening complication of babesiosis, manifesting as sudden, severe left-sided abdominal pain, hemodynamic instability, and a rapidly falling hemoglobin. It requires emergency surgical management.
For patients who lack a spleen entirely (asplenic patients), this protective filtering mechanism is completely absent. Parasitized RBCs circulate freely, parasitemia climbs unchecked, and the entire burden of immune defense shifts to circulating antibodies and macrophages — a burden they cannot manage alone without the spleen's architectural and immunological contributions. This is why asplenic patients develop the highest parasitemia levels and the most severe, rapidly fatal disease.
9. Concurrent Lyme Disease: Amplified Symptoms
Babesia microti and Borrelia burgdorferi — the agent of Lyme disease — share the same tick vector, Ixodes scapularis, and both circulate in the same reservoir hosts. Co-infection from a single tick bite is well documented, with studies in high-endemic regions finding that 20–40% of patients with symptomatic B. microti infection are simultaneously infected with Borrelia burgdorferi. Anaplasma phagocytophilum (anaplasmosis) is a third co-circulating tick-borne pathogen, adding a possible third simultaneous infection.
Co-infection with Lyme disease amplifies the systemic symptoms of babesiosis. Studies have shown that patients with both B. microti and B. burgdorferi experience more severe fatigue, more pronounced fever, and a longer duration of illness than patients with either infection alone. The immunological basis for this synergy is not fully elucidated, but there is evidence that Borrelia may modulate immune responses in ways that reduce clearance of Babesia, potentially allowing higher parasitemia to develop.
The treatment implications are important: doxycycline, the first-line treatment for Lyme disease, has no efficacy against Babesia. A patient prescribed doxycycline for presumed Lyme disease who fails to improve within a few days — or whose blood tests reveal hemolytic anemia and thrombocytopenia — should be evaluated immediately for concurrent babesiosis. Adding atovaquone and azithromycin to the treatment regimen is the appropriate response. Conversely, babesiosis treatment (atovaquone plus azithromycin) does not adequately treat Lyme disease, so both infections must be diagnosed and treated simultaneously in co-infected patients.
10. Incubation Period and Timing of Symptom Onset
The incubation period for tick-transmitted Babesia microti infection is typically 1–4 weeks after the tick bite. Most symptomatic patients develop illness within 2–3 weeks. The peak risk season in the northeastern United States is late spring through early summer (May–July), when nymphal Ixodes ticks are most active. Many patients presenting with babesiosis in July or August had their tick bite in late May or June and have been asymptomatically incubating the infection for weeks.
A critical and often overlooked incubation period applies to transfusion-transmitted babesiosis: 1–9 weeks after receiving a blood transfusion. This extended window — up to more than two months — means that a hospitalized patient developing unexplained fever and anemia in September may have acquired Babesia from a transfusion received in July. Without an explicit question about recent transfusions and a clinician who is aware of transfusion-transmitted babesiosis, this diagnosis is easily missed.
Patients sometimes dismiss the tick bite history because the bite was small and painless — nymphal ticks are the size of a poppy seed and can feed for 24–48 hours undetected, particularly on the scalp, behind the ears, in the axillae, and in the groin. A careful history asking about outdoor activities (hiking, camping, gardening, yard work, golf) in endemic areas during the prior 1–4 weeks is essential. When a patient in an endemic state presents in summer with unexplained fever, hemolytic anemia, and thrombocytopenia, babesiosis should be in the differential regardless of whether they recall a specific tick bite.
Key Research Papers
Foundational and current literature on Babesia hemolytic anemia, pathophysiology, and clinical presentation.
- Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366(25):2397–2407 — Search PubMed
- Krause PJ, McKay K, Thompson CA, et al. Disease-specific diagnosis of coinfecting tickborne zoonoses. Clin Infect Dis. 2002;34(9):1184–1191. PMID: 11941544
- Leiby DA. Transfusion-transmitted Babesia spp.: bull's-eye on Babesia microti. Clin Microbiol Rev. 2011;24(1):14–28 — Search PubMed
- Lobo CA, Rodriguez M, Cursino-Santos JR. Babesia and red cell invasion. Curr Opin Hematol. 2012;19(3):170–177 — Search PubMed
- Hatcher JC, Greenberg PD, Antique J, Jimenez-Lucho VE. Severe babesiosis in Long Island: review of 34 cases and their complications. Clin Infect Dis. 2001;32(8):1117–1125. PMID: 11283800
- Moniuszko A, Dunaj J, Swiecicka I, et al. Co-infections with Borrelia species, Anaplasma phagocytophilum and Babesia spp. in patients with tick-borne encephalitis. Eur J Clin Microbiol Infect Dis. 2014;33(10):1835–1841 — Search PubMed
- Vannier EG, Diuk-Wasser MA, Ben Mamoun C, Krause PJ. Babesiosis. Infect Dis Clin North Am. 2015;29(2):357–370 — Search PubMed
- Herwaldt BL, Linden JV, Bosserman E, Young C, Olkowska D, Wilson M. Transfusion-associated babesiosis in the United States: a description of cases. Ann Intern Med. 2011;155(8):509–519 — Search PubMed
- Krause PJ, Spielman A, Telford SR 3rd, et al. Persistent parasitemia after acute babesiosis. N Engl J Med. 1998;339(3):160–165. PMID: 9664092
- Krause PJ, Gewurz BE, Hill D, et al. Persistent and relapsing babesiosis in immunocompromised patients. Clin Infect Dis. 2008;46(3):370–376 — Search PubMed
Live PubMed Searches
- Babesia hemolytic anemia pathophysiology
- Babesia microti blood smear diagnosis
- Babesiosis fever chills clinical presentation
- Babesia duncani West Coast
- Babesia divergens Europe asplenic
- Babesiosis Lyme co-infection symptoms
Connections
- All Parasites
- Babesia Overview
- Babesia Symptoms Hub
- Severe Babesiosis & Immunocompromised
- Diagnosis: Blood Smear & PCR
- Babesia Treatments Hub
- Atovaquone & Azithromycin Treatment
- Exchange Transfusion & Severe Disease
- Tick Prevention & Environmental Control
- Malaria
- Hematology
- Lyme Disease
- Babesiosis — the general infectious-disease overview of the illness these hemolytic and flu-like symptoms belong to.