Diagnosing Babesiosis: Blood Smear, PCR, and Serology
Diagnosing babesiosis requires combining the right clinical suspicion with the right tests in the right order. The diagnosis is missed far too often — sometimes because the clinician did not consider it, and sometimes because the test result was misinterpreted. A negative blood smear does not rule out babesiosis in a patient with a convincing clinical picture. PCR is more sensitive than smear at low parasitemia levels. Serology confirms exposure but cannot diagnose acute infection in the first week. And Babesia ring forms on smear are frequently mistaken for malaria by clinicians who have not seen babesiosis before. This page explains each diagnostic tool, its strengths and limitations, how to distinguish Babesia from Plasmodium on smear, and what the supporting laboratory findings mean.
Table of Contents
- Peripheral Blood Smear (Giemsa Stain)
- Distinguishing Babesia from Plasmodium
- PCR: The Gold Standard for Accuracy
- Serology (IFA): Confirming Exposure
- Why Species Identification Matters
- Parasitemia Percentage Calculation
- CBC Findings: The Hemolysis Signature
- Direct Coombs Test in Babesiosis
- Reticulocyte Count: Bone Marrow Response
- Liver and Metabolic Tests in Severe Disease
- Key Research Papers
- Connections
- Featured Videos
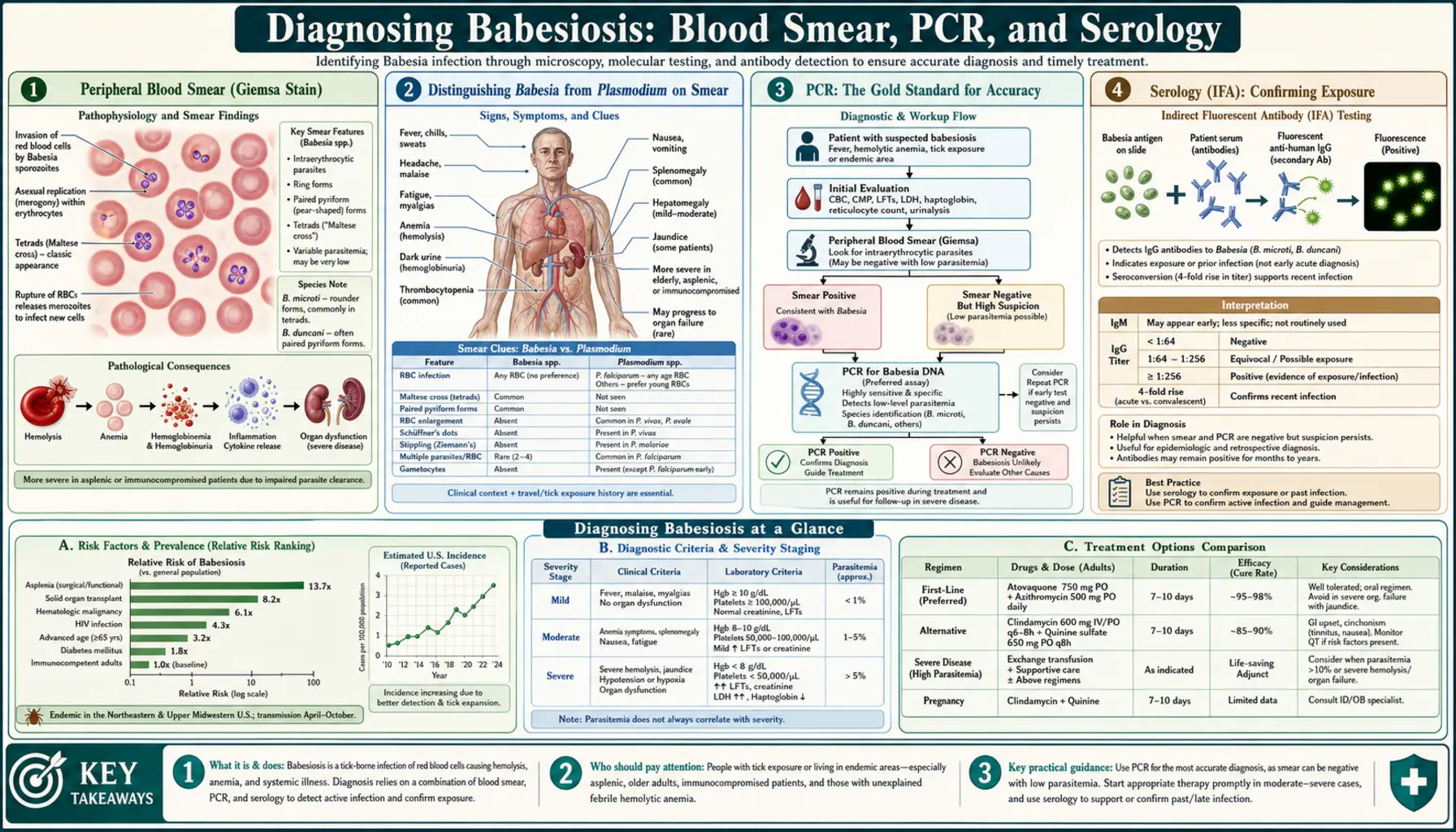
1. Peripheral Blood Smear (Giemsa Stain)
The peripheral blood smear stained with Giemsa (or Wright-Giemsa) stain is the first-line diagnostic test for babesiosis in a symptomatic patient and the fastest way to confirm active parasitemia. A skilled microscopist examining a well-prepared Giemsa smear can identify Babesia ring forms within 15–30 minutes of receiving the specimen, enabling a same-visit diagnosis in urgent cases.
On Giemsa smear, Babesia parasites appear as small blue ring forms inside red blood cells. In early infection when each parasite is still a single ring form, the appearance is similar to early-stage Plasmodium falciparum rings. As the parasite matures and divides, the characteristic morphological features emerge: multiple rings per RBC (two, three, or four parasites within a single cell), extracellular merozoites (free ring forms floating outside RBCs in the plasma — a finding not seen with Plasmodium), and most importantly, the tetrad (Maltese cross) formation — four merozoites arranged in a cross pattern within a single RBC, connected at their apices. The tetrad is pathognomonic for B. microti and distinguishes it definitively from all species of Plasmodium.
The sensitivity of a single blood smear for B. microti is imperfect, particularly in early infection when parasitemia is low (<0.5%). Studies suggest sensitivity of 70–75% for a single thin blood smear examined by an experienced microscopist, improving to over 90% when three separate smears are examined. The reason is that parasitemia fluctuates over time as waves of merozoites invade and replicate; sampling at a moment when parasitemia is temporarily low may miss sparse ring forms. If clinical suspicion is high and the first smear is negative, the smear should be repeated in 24–48 hours and PCR should be ordered concurrently.
The smear also serves a quantitative function: parasitemia percentage (the number of parasitized RBCs per 100 RBCs counted) guides clinical severity assessment and treatment decisions. Parasitemia above 4% indicates severe disease; above 10% typically prompts exchange transfusion consideration. The smear should therefore be reported not only as positive or negative, but with a parasitemia percentage.
2. Distinguishing Babesia from Plasmodium on Smear
The diagnostic confusion between Babesia and Plasmodium falciparum is clinically consequential because they require entirely different treatments: Babesia is treated with atovaquone/azithromycin or clindamycin/quinine; malaria is treated with artemisinin-based combination therapy, chloroquine (for non-falciparum species), or other antimalarials. Giving malaria treatment for babesiosis or vice versa is not effective and delays appropriate care. The distinction matters at the bedside.
Hemozoin (malaria pigment): The most reliable distinguishing feature. Plasmodium species digest hemoglobin inside infected RBCs and produce hemozoin — a dark brown-black pigment — as a byproduct. Hemozoin is visible on Giemsa smear as dark granular deposits within parasitized cells and within the cytoplasm of monocytes and macrophages that have phagocytosed infected RBCs. Babesia does not produce hemozoin. An infected RBC with no dark pigment granules strongly suggests Babesia; infected cells with dark pigment granules are Plasmodium.
Tetrad (Maltese cross) formation: Unique to Babesia. No Plasmodium species produces a tetrad. Seeing a Maltese cross on smear is pathognomonic and confirms babesiosis. However, the tetrad is seen in only 1–5% of parasitized cells in most cases, so its absence does not exclude Babesia.
Extracellular merozoites: Free ring forms outside RBCs are visible in babesiosis smears but are not seen in Plasmodium infections. If the microscopist sees ring forms floating free in the plasma without being inside a cell, this is a strong argument for Babesia.
RBC size: Babesia-infected RBCs are not enlarged — they are normal size. Plasmodium vivax and P. ovale enlarge infected RBCs. This distinction is most useful for ruling in babesiosis when cells are clearly not enlarged; falciparum also does not enlarge cells, so the absence of RBC enlargement does not distinguish Babesia from falciparum.
Banana-shaped gametocytes: Plasmodium falciparum produces distinctive crescent (banana)-shaped gametocytes visible on smear. Babesia does not produce gametocytes in human blood. Seeing banana-shaped gametocytes confirms malaria.
Multiple infections per cell: While multiple ring forms per cell can be seen in both P. falciparum and Babesia, having four forms arranged in a tetrad is unique to Babesia.
In practice, the combination of no hemozoin, presence of extracellular merozoites, and (if present) tetrad formation in a patient from a US endemic area with no malaria travel history is diagnostic for babesiosis, even before PCR confirmation.
3. PCR: The Gold Standard for Accuracy
Polymerase chain reaction (PCR) testing on whole blood is the most sensitive diagnostic test for babesiosis and is now the preferred test for both initial diagnosis (especially in early infection with low parasitemia) and for follow-up monitoring of treatment response in immunocompromised patients. PCR detects and amplifies Babesia DNA directly, enabling detection of parasitemia levels far below the threshold visible on blood smear.
Real-time quantitative PCR (qPCR) offers additional advantages: it quantifies the copy number of Babesia DNA, providing an estimate of parasitemia that complements the smear-based parasitemia percentage. In early infection, PCR can be positive 3–7 days before the first positive smear, because a single PCR test can detect as few as 1–10 parasites per microliter of blood. For comparison, the lower detection threshold of light microscopy by an experienced microscopist is approximately 50–100 parasites per microliter.
PCR also enables species identification, which is clinically important. Primers targeting the 18S ribosomal RNA gene can distinguish B. microti, B. duncani, B. divergens, and rarer species. B. divergens requires more aggressive initial management in patients with any degree of immunocompromise; B. duncani is associated with more severe hemolysis than B. microti even in healthy patients. Knowing the species guides treatment duration in immunocompromised patients and provides prognostic information.
PCR remains positive for several weeks after treatment is initiated and parasitemia clears on smear. In immunocompromised patients who require treatment until two consecutive negative PCR results, this persistence is clinically important — a positive PCR 4–6 weeks after starting treatment in a B-cell-depleted patient signals persistent infection, not just residual DNA, and warrants continued treatment. The test should be ordered as Babesia PCR (whole blood) at a reference laboratory experienced with tick-borne disease testing. Many commercial labs now offer this test.
4. Serology (IFA): Confirming Exposure
Immunofluorescence antibody (IFA) testing measures the patient's IgM and IgG antibody responses to Babesia antigens. A titer of IgG ≥1:64 against B. microti antigens is considered diagnostic of past or current infection in the appropriate clinical context. Paired acute and convalescent sera showing a fourfold rise in IgG titer (drawn 2–4 weeks apart) is the classical serological confirmation of active infection.
The critical limitation of IFA serology for babesiosis diagnosis is timing. The adaptive immune response requires time to generate detectable antibody levels: IgM appears first, typically 1–2 weeks after infection; IgG appears 2–4 weeks after infection and rises over 4–8 weeks before gradually declining. During the first 1–2 weeks of symptomatic babesiosis — the acute phase when diagnosis is most urgently needed — serology is often negative because antibodies have not yet formed. A negative IFA in a patient presenting acutely with 3–5 days of febrile illness does not rule out babesiosis.
IFA serology is most useful in three situations: confirming the diagnosis retrospectively when parasitemia has already cleared by the time the patient seeks care (PCR and smear may be negative, but IgG will be positive if infection occurred within the past 6–12 months); epidemiological studies of seroprevalence in endemic populations; and confirming the diagnosis in a patient whose PCR result was negative but clinical suspicion remains high (paired acute and convalescent IFA may show seroconversion).
Antibody titers can remain elevated (IgG ≥1:64) for 6–12 months after treated infection, declining gradually. A positive IFA does not distinguish active current infection from treated past infection — this is why PCR is preferred for monitoring treatment response. Cross-reactivity with other Apicomplexa parasites (e.g., Plasmodium) is rare at the titers used for diagnosis, but clinicians should be aware that mild cross-reactivity exists and that confirmatory PCR is advisable in ambiguous cases.
5. Why Species Identification Matters
Not all Babesia species behave the same way clinically, and species identification has direct implications for prognosis and treatment decisions.
Babesia microti (US Northeast and upper Midwest): The mildest human species, though still capable of causing severe and fatal disease in vulnerable patients. Standard treatment duration is 7–10 days with atovaquone/azithromycin for mild-to-moderate disease. Species confirmation is particularly important in immunocompromised patients receiving extended treatment regimens.
Babesia duncani (US West Coast): Causes more severe hemolysis than B. microti and has been associated with fatal outcomes in immunocompetent patients. Treatment is the same regimen but clinicians should have a lower threshold for hospitalization and closer monitoring in documented B. duncani infection.
Babesia divergens (Europe): Requires immediate, aggressive treatment in any patient, but especially in asplenic patients where case fatality exceeds 40% in untreated cases. Some experts recommend exchange transfusion as initial management in all asplenic patients with B. divergens regardless of parasitemia level, given the rapidity of deterioration. Standard antiparasitic therapy is the same, but treatment duration may need to be extended.
PCR with species-level identification is available at specialized reference laboratories including the CDC and several academic medical centers. For routine community-based babesiosis in a patient without risk factors in a B. microti-endemic state, species identification is often assumed rather than confirmed explicitly. But in any patient with unusual severity, no clear epidemiological exposure, or treatment failure, explicit species identification by PCR is warranted.
6. Parasitemia Percentage Calculation
Parasitemia percentage is calculated from the peripheral blood smear by counting the number of parasitized RBCs out of a total of 500–1000 RBCs examined under oil-immersion microscopy. The formula is: (number of parasitized RBCs / total RBCs counted) × 100 = parasitemia %.
For example, if a microscopist counts 500 RBCs and finds 20 with parasites visible inside them, the parasitemia is 4%. This deceptively simple calculation has important clinical weight: parasitemia <4% is generally classified as mild-to-moderate disease manageable without exchange transfusion in most patients; 4–10% is classified as severe disease warranting hospitalization and possible exchange transfusion; >10% in a deteriorating patient or asplenic patient is a strong indication for exchange transfusion.
Parasitemia measurement is imprecise at low levels (<1%), where counting variability between microscopic fields can significantly affect the result. It is also imprecise at very high levels where counting becomes technically difficult. In practice, repeat smears every 24–48 hours during the acute treatment phase track the trend in parasitemia — a falling parasitemia confirms treatment response; a rising parasitemia despite treatment in an immunocompetent patient may indicate drug resistance or inadequate drug levels, while in an immunocompromised patient it more commonly reflects inability to clear the parasite immunologically.
In clinical practice, the parasitemia percentage from the blood smear is used as an adjunct to clinical assessment, not as the sole decision-making tool. A patient with 3% parasitemia who is hemodynamically unstable, anuric, and hypoxic warrants the same urgency as a patient with 12% parasitemia who is clinically stable. Clinical status and rate of deterioration are as important as the parasitemia number.
7. CBC Findings: The Hemolysis Signature
The complete blood count (CBC) in symptomatic babesiosis produces a characteristic pattern that, while not diagnostic by itself, strongly supports the diagnosis in the right clinical context and guides assessment of severity.
Hemoglobin and hematocrit: Falling progressively as hemolysis continues. The rate of decline correlates with parasitemia level and disease severity. Hemoglobin of 8–10 g/dL is common in moderate disease; below 7 g/dL indicates severe hemolysis. The anemia is normocytic (normal MCV) and normochromic (normal MCHC), reflecting the fact that the problem is destruction of normal-sized, normal-colored cells rather than impaired synthesis or iron deficiency.
Thrombocytopenia: Present in 50–70% of symptomatic babesiosis patients and is one of the most consistent laboratory findings. The mechanism involves splenic sequestration of platelets (the enlarged, hyperactive spleen traps platelets), immune-mediated platelet destruction, and in severe cases DIC-related consumption. Platelet counts of 50,000–100,000/μL are common in moderate disease. Platelet counts below 20,000/μL indicate severe disease and potential DIC.
White blood cell count: Generally normal or mildly elevated in babesiosis. This distinguishes babesiosis from anaplasmosis (which typically causes significant leukopenia), and from bacterial sepsis (which usually causes a marked leukocytosis). A white cell count that is significantly elevated (>15,000/μL) in a patient with presumed babesiosis should prompt consideration of concurrent bacterial infection or a different diagnosis.
LDH (lactate dehydrogenase): Markedly elevated, often 2–5 times the upper limit of normal. LDH is released from the cytoplasm of all lysed cells and is a sensitive marker of ongoing hemolysis. Serial LDH measurements track treatment response: falling LDH confirms that hemolysis is slowing.
Haptoglobin: Low or undetectable. Haptoglobin is consumed as it binds free hemoglobin from lysed RBCs; when hemolysis is rapid and large-scale, haptoglobin is depleted. Undetectable haptoglobin is a sensitive but not specific marker of significant hemolysis (it is also low in liver failure, where synthesis is reduced).
Indirect bilirubin: Elevated from heme catabolism as the liver processes the free hemoglobin and heme from lysed RBCs. Clinical jaundice (yellowing of the sclera and skin) becomes apparent when total bilirubin exceeds approximately 3 mg/dL.
8. Direct Coombs Test in Babesiosis
The direct antiglobulin test (DAT), also called the direct Coombs test, detects immunoglobulin (IgG) and/or complement (C3d) coating the surface of the patient's red blood cells. A positive DAT indicates that the patient's own immune system is recognizing surface proteins on their RBCs — a finding that, in the context of hemolytic anemia, confirms an immune-mediated component to the hemolysis.
In babesiosis, the direct Coombs test is positive in a subset of patients. The mechanism involves both direct antibody coating of parasitized RBCs (targeting Babesia antigens on the cell surface) and bystander damage to non-parasitized RBCs that become coated with antibody as a result of the broad immune activation. This immune-mediated hemolysis occurs alongside and in addition to the direct parasitic destruction of RBCs, and it explains why the degree of anemia sometimes exceeds what would be predicted from the parasitemia level alone.
The Coombs test can remain positive for weeks after the parasite has been cleared, because the immune activation persists for some time after parasitemia resolves. This means a recovering patient may continue to have mild anemia from ongoing immune-mediated hemolysis even after successful antiparasitic treatment, and may require a longer period before their hemoglobin normalizes. Follow-up CBC at 4–6 weeks after treatment confirms recovery of hemoglobin to normal levels.
9. Reticulocyte Count: Bone Marrow Response
Reticulocytes are immature red blood cells released early from the bone marrow in response to hemolysis or hemorrhage. Under normal circumstances, the bone marrow releases mature RBCs into the circulation, and the reticulocyte count (normally <2% of circulating RBCs) reflects this steady-state production. When hemolysis accelerates RBC destruction, the bone marrow responds by releasing reticulocytes early and in increased numbers — the reticulocyte count rises.
In symptomatic babesiosis, reticulocytosis is expected and is a marker of the bone marrow's appropriate response to hemolytic anemia. A reticulocyte count of 3–8% (sometimes higher in brisk hemolysis) is typical during active infection. This elevated reticulocyte count distinguishes hemolytic anemia from aplastic anemia or other hypoproliferative anemias (where the bone marrow fails to respond), and from nutritional anemias (iron, B12, folate deficiency) where reticulocytosis is absent despite falling hemoglobin.
In severe babesiosis, very high reticulocyte counts may cause a misleadingly elevated MCV (mean corpuscular volume) on the CBC, because reticulocytes are slightly larger than mature RBCs. This can make the anemia appear mildly macrocytic rather than normocytic. Awareness of this artifact prevents unnecessary workup for macrocytic anemia (B12/folate deficiency) in a patient whose elevated MCV is explained entirely by reticulocytosis from hemolysis.
Following the reticulocyte count during recovery provides a measure of bone marrow response: a rising reticulocyte count as treatment begins (reflecting marrow stimulation by the anemia) followed by a gradual fall as hemoglobin recovers toward normal confirms appropriate hematological response to therapy.
10. Liver and Metabolic Tests in Severe Disease
Liver function tests (LFTs) and metabolic panels provide additional diagnostic and severity information in babesiosis, particularly in moderate-to-severe disease where organ involvement extends beyond the blood compartment.
Aminotransferases (AST, ALT): Mildly elevated in most symptomatic babesiosis cases, reflecting hepatic involvement from hemolysis (the liver processes massive amounts of heme from lysed RBCs) and from cytokine-mediated hepatic inflammation. Transaminase elevations of 1–3 times the upper limit of normal are common and typically resolve with treatment. Markedly elevated transaminases (>5 times normal) suggest more severe hepatic injury from microvascular obstruction (parasitized RBCs lodging in hepatic sinusoids) or concurrent hepatitis from another tick-borne co-infection.
Bilirubin (total, direct, indirect): Elevated total and indirect bilirubin reflects heme catabolism from hemolysis. Elevated direct bilirubin suggests hepatic involvement impairing bilirubin conjugation and excretion. Severely elevated bilirubin (>10 mg/dL) is a marker of severe disease.
Alkaline phosphatase (ALP) and GGT: May be mildly elevated, particularly in patients with concurrent biliary inflammation. Large elevations should prompt investigation for an alternative hepatobiliary diagnosis.
Creatinine and BUN: Rising in renal failure from pigment nephropathy or glomerular injury. Creatinine above 2 mg/dL indicates significant AKI and warrants close monitoring and aggressive hydration. The BUN/creatinine ratio may be elevated due to increased urea production from catabolism of hemoglobin in addition to intrinsic renal impairment.
LDH: As noted in the CBC section, LDH is the most sensitive correlate of ongoing hemolysis and is often the first laboratory value to improve as treatment takes effect. A falling LDH within 48–72 hours of initiating antiparasitic therapy is one of the earliest signs of treatment response.
Prothrombin time (PT) and activated partial thromboplastin time (aPTT): Prolonged in DIC, reflecting depletion of clotting factors. A rising PT/PTT combined with falling fibrinogen and elevated D-dimer confirms DIC and warrants FFP replacement.
Key Research Papers
Primary literature on babesiosis diagnosis, smear interpretation, PCR methods, and laboratory findings.
- Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366(25):2397–2407 — Search PubMed
- Linden JV, Wong SJ, Chu FK, et al. Transfusion-associated transmission of babesiosis in New York state. Transfusion. 2000;40(3):285–289 — Search PubMed
- Leiby DA. Transfusion-transmitted Babesia spp.: bull's-eye on Babesia microti. Clin Microbiol Rev. 2011;24(1):14–28 — Search PubMed
- Krause PJ, Spielman A, Telford SR 3rd, et al. Persistent parasitemia after acute babesiosis. N Engl J Med. 1998;339(3):160–165. PMID: 9664092
- Vannier EG, Diuk-Wasser MA, Ben Mamoun C, Krause PJ. Babesiosis. Infect Dis Clin North Am. 2015;29(2):357–370 — Search PubMed
- Lobo CA, Rodriguez M, Cursino-Santos JR. Babesia and red cell invasion. Curr Opin Hematol. 2012;19(3):170–177 — Search PubMed
- Hatcher JC, Greenberg PD, Antique J, Jimenez-Lucho VE. Severe babesiosis in Long Island: review of 34 cases and their complications. Clin Infect Dis. 2001;32(8):1117–1125. PMID: 11283800
- Krause PJ, McKay K, Thompson CA, et al. Disease-specific diagnosis of coinfecting tickborne zoonoses. Clin Infect Dis. 2002;34(9):1184–1191. PMID: 11941544
- Herwaldt BL, Linden JV, Bosserman E, et al. Transfusion-associated babesiosis in the United States: a description of cases. Ann Intern Med. 2011;155(8):509–519 — Search PubMed
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis. Clin Infect Dis. 2006;43(9):1089–1134 — Search PubMed
Live PubMed Searches
- Babesia diagnosis PCR blood smear
- Babesia Giemsa stain morphology
- Babesia versus Plasmodium differentiation
- Babesiosis laboratory findings CBC
- Babesia serology IFA antibody
- Babesia species identification PCR
Connections
- All Parasites
- Babesia Overview
- Babesia Symptoms Hub
- Hemolytic Anemia & Flu Symptoms
- Severe Babesiosis & Immunocompromised
- Babesia Treatments Hub
- Atovaquone & Azithromycin Treatment
- Exchange Transfusion & Severe Disease
- Tick Prevention & Environmental Control
- Hematology
- Malaria
- Lyme Disease
- Babesiosis — the full disease overview: transmission, clinical course, severity, and treatment.