Chronic Pain: History and Discovery
For most of recorded history, pain was a riddle. Philosophers debated whether it was an emotion of the soul or a message from the body, and physicians could do little more than dull it. This page traces two intertwined stories: the slow scientific effort to understand how pain works — from Aristotle and Galen, through Descartes' famous "bell-rope" image of 1664, to the revolutionary Gate Control Theory of Pain published by Ronald Melzack and Patrick Wall in 1965 — and the much more recent recognition that chronic pain is not merely a long-lasting symptom but a condition in its own right, a shift now formalized in the World Health Organization's ICD-11 (adopted 2019). Names, dates, and "firsts" below have been checked against multiple sources; where the history is a hypothesis rather than settled fact, it is marked as such.
Table of Contents
- Ancient Ideas: Pain of the Heart, Pain of the Nerves
- Descartes and the Bell-Rope (1664)
- The Nineteenth Century: Specificity, Intensity, and the Search for Pain Nerves
- The Gate Control Theory (Melzack & Wall, 1965)
- John Bonica and the Birth of Pain Medicine
- Measuring Pain and the Neuromatrix
- The Opioid Story: Relief and Crisis
- Chronic Pain Becomes a Disease: ICD-11 (2019)
- Research Papers and References
- Connections
- Featured Videos
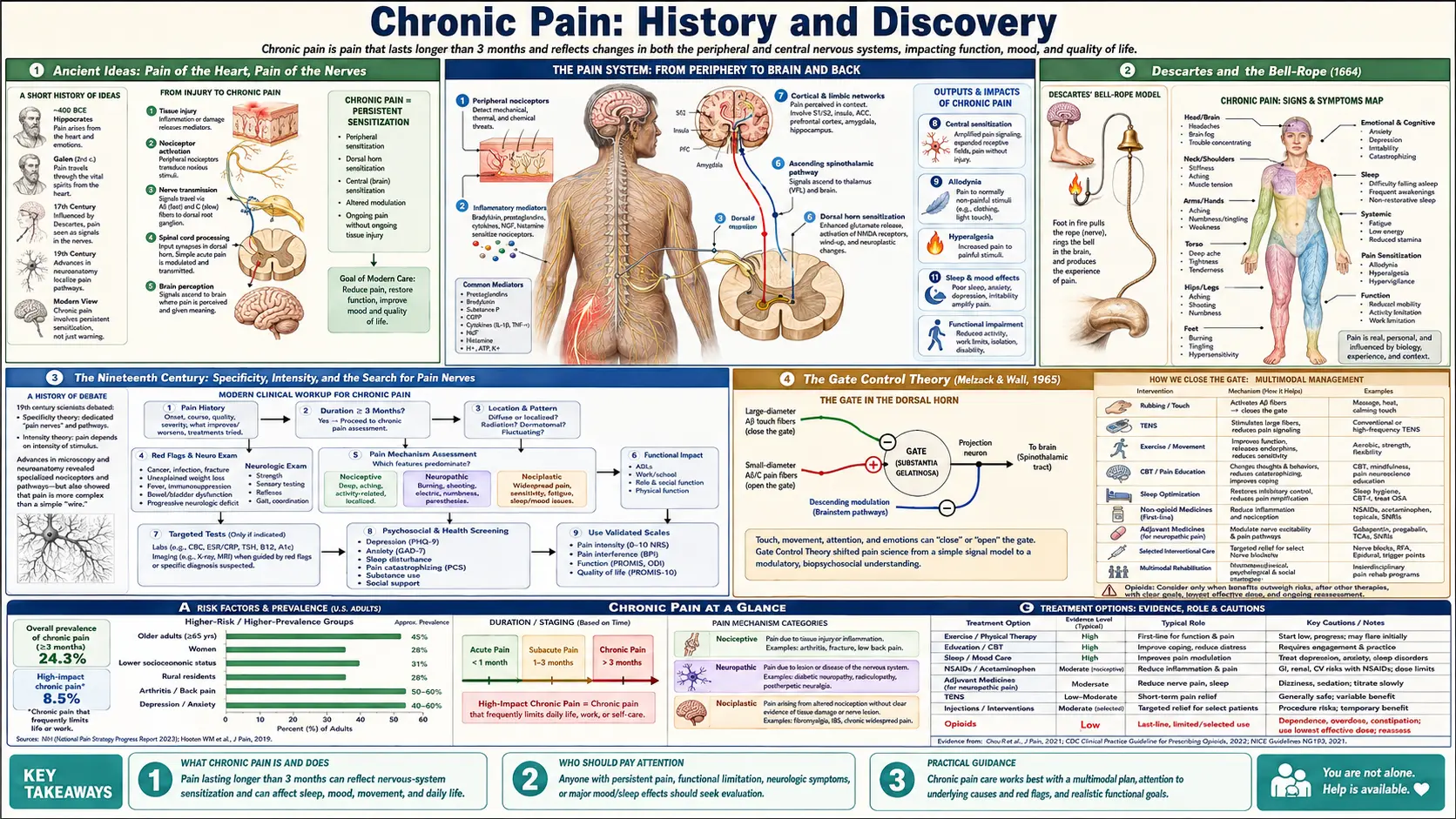
Ancient Ideas: Pain of the Heart, Pain of the Nerves
The question of what pain is — and where in the body it happens — has been argued for well over two thousand years. In ancient Greece, Aristotle (384–322 BCE) did not count pain among the five senses at all. Following Plato, he treated pain and pleasure as emotions, "passions of the soul," rather than as a distinct sensory channel. Just as importantly, Aristotle held the cardiocentric view that the heart, not the brain, was the seat of sensation; for him pain arose from disturbances of the heart and blood. This was an influential idea, not a proven one, and it shaped Western thinking for centuries.
The counter-tradition placed sensation firmly in the nervous system. Writing roughly 450 years after Aristotle, the Greco-Roman physician Galen of Pergamon (c. 129–c. 216 CE) argued that sensory impressions — including those that become pain — are carried by nerves to the brain. Galen reportedly demonstrated the role of the spinal cord experimentally, severing it in animals to show that the conduction of feeling to the brain could be interrupted. Galen's anatomy dominated European medicine for more than a thousand years, and his brain-and-nerves account of sensation is, in broad outline, the one that eventually won.
It is worth being clear that these were theories of sensation, often entangled with philosophy and religion, not the modern, testable neuroscience of pain. For most of antiquity and the Middle Ages, pain was also understood through frameworks such as the four humours, and was frequently given moral or spiritual meaning. What the ancients bequeathed to later science was a framing question that is still alive today: is pain a thing the body simply detects, or an experience the mind constructs?
Descartes and the Bell-Rope (1664)
The single most famous image in the early science of pain comes from the French philosopher and mathematician René Descartes (1596–1650). In his Treatise of Man (L'Homme) — a manuscript he left unpublished in his lifetime, printed posthumously in Latin in 1662 and in French in 1664 — Descartes described the body as a kind of machine and pain as a signal travelling along a fixed pathway from the site of injury to the brain. The historical date attached to this model, 1664, refers to that French edition.
Descartes illustrated the idea with an analogy that has echoed ever since: a foot near a fire sets off a chain of events "just as, pulling on one end of a rope, one makes a bell ring at the other end." In this bell-rope picture, particles of fire tug a delicate thread running up to the brain, much as a rope rung in a church tower sounds the bell above. The model implied a direct, one-to-one relationship between the amount of tissue damage and the amount of pain felt — the seed of what would later be called the specificity theory of pain.
Two points are often missed. First, Descartes' mechanistic pathway is essentially a description of what we now call nociception — the detection and signalling of damaging stimuli — and within the same work he distinguished that signalling from the conscious experience of pain, which he located in the mind/brain. Second, although the rigid "injury in, pain out" reading of Descartes turned out to be incomplete, his linear pathway was enormously productive: it gave anatomists and physiologists a concrete picture to test, and the next three centuries of pain science can be read as a long argument with, and eventual revision of, the bell-rope.
The Nineteenth Century: Specificity, Intensity, and the Search for Pain Nerves
Descartes' intuition hardened into formal theory in the nineteenth century, as physiologists tried to map sensation onto real nerves. The German physiologist Johannes Müller proposed (in the 1830s–1840s) the law of specific nerve energies — the idea that each nerve carries one specific kind of sensation. Building on this, the anatomist Maximilian von Frey, around 1894–1895, advanced a detailed specificity theory of pain, proposing dedicated pain receptors and pain-specific pathways, an account that fit neatly with the discovery of distinct "sensory spots" on the skin.
A rival camp argued that pain was not a separate sense at all but a matter of degree. The intensity (or summation) theory — associated in the nineteenth century with figures such as Wilhelm Erb and developed by others into pattern and summation models — held that any sensation, if intense enough, becomes pain, and that pain reflects the pattern and summation of nerve impulses rather than a private pain line. The debate between specificity and pattern/intensity views ran, unresolved, into the twentieth century.
By the mid-twentieth century neither camp could explain the everyday facts clinicians saw: soldiers with terrible wounds who reported little pain, patients whose pain persisted long after an injury had healed, the agony of phantom limbs in people who had no limb at all, and the way rubbing or distraction could ease hurt. Pure specificity could not account for pain without injury; pure intensity could not account for the obvious specialization of the nervous system. The stage was set for a theory that could hold both ideas at once.
The Gate Control Theory (Melzack & Wall, 1965)
The landmark modern theory of pain arrived in 1965. The Canadian psychologist Ronald Melzack (1929–2019) and the British physiologist Patrick Wall (1925–2001) published "Pain mechanisms: a new theory" in the journal Science (1965, volume 150, pages 971–979). Their Gate Control Theory of Pain proposed that, before pain signals reach the brain, they pass through a kind of neural "gate" in the dorsal horn of the spinal cord that can turn the volume of those signals up or down.
The mechanism, in plain terms: large-diameter nerve fibres that carry touch and pressure tend to close the gate, while small-diameter fibres that carry injury signals tend to open it — and, crucially, signals descending from the brain can also push the gate one way or the other. This single idea elegantly explained the puzzles the older theories could not: why rubbing a banged shin helps (touch fibres closing the gate), why a frightened or focused person may not feel a wound, and why mood, attention, and past experience change how much something hurts. Pain, in this view, is not a simple one-to-one readout of injury; it is modulated, contextual, and shaped by the nervous system itself.
The impact was immense, and it reframed the entire field. Some of the specific wiring details proposed in 1965 were later debated and revised — the gate metaphor is a model, not a literal switch — but its central claim, that pain transmission is actively gated and top-down modulated, has been repeatedly supported and remains foundational. It also opened the door to new, non-drug treatments built on the principle of "closing the gate" with competing sensory input. Within two years, in 1967, Patrick Wall and the neurosurgeon William Sweet reported relieving pain in patients with electrical stimulation of nerves — an approach that helped give rise to transcutaneous electrical nerve stimulation (TENS) and, in the same period (work by Norman Shealy and colleagues), to spinal cord stimulation. Modern pain medicine is, in large part, the offspring of the gate.
John Bonica and the Birth of Pain Medicine
Understanding pain is one thing; building a medical specialty to treat it is another. That second achievement belongs above all to John J. Bonica (1917–1994), an Italian-American anesthesiologist widely called the "father of pain medicine." Caring for grievously wounded soldiers as an army physician during the Second World War, Bonica saw that no single doctor could manage complex, persistent pain, and he established what is generally recognized as the first multidisciplinary pain clinic — in Tacoma/Seattle, Washington, in the late 1940s (around 1947) — bringing anesthesiologists, surgeons, neurologists, psychiatrists, and others around one patient.
In 1953 Bonica published his monumental textbook The Management of Pain, which for the first time gathered the scattered knowledge of pain diagnosis and treatment into a single comprehensive reference and effectively defined the new field. He argued persistently that chronic pain deserved its own clinical attention and a team-based, biopsychosocial approach — ideas decades ahead of their time.
Bonica also built the institutions. In May 1973 he convened roughly 350 researchers and clinicians from many disciplines and countries at a meeting in Issaquah, near Seattle, that led directly to the founding of the International Association for the Study of Pain (IASP) (the organization was formally incorporated in 1974). IASP went on to launch the influential journal PAIN and, in 1979, to publish the first widely adopted formal definition of pain — the framework that, decades later, would carry the classification of chronic pain into the WHO's disease catalogue.
Measuring Pain and the Neuromatrix
If pain is shaped by mind as well as body, then measuring it cannot be a matter of injury size alone — it must capture what the sufferer actually feels. In 1975, Ronald Melzack published the McGill Pain Questionnaire in the journal PAIN, a tool that asks patients to choose from carefully grouped descriptive words (sensory words like "burning" or "stabbing," affective words like "exhausting" or "sickening") to characterize their pain. It was a milestone: one of the first instruments to treat pain as a multidimensional experience and to put a number on its quality as well as its intensity. The McGill Pain Questionnaire has since been translated into many languages and remains among the most widely used pain-measurement tools in research and clinics worldwide.
Melzack's later work pushed the gate idea further into the brain. Struggling to explain phantom limb pain — severe pain felt in a limb that no longer exists, and which therefore cannot be sending any injury signals — he proposed the neuromatrix theory of pain, developed across the late 1980s and 1990s (notably in publications around 1989, 1999, and 2001). The theory holds that pain is ultimately produced by the brain: a widely distributed network (the "body-self neuromatrix") generates a characteristic pattern, or "neurosignature," that we experience as pain, with sensory input being one influence among many rather than the sole cause.
The neuromatrix theory deliberately moves away from the strict Cartesian picture: pain need not begin with tissue damage, and the brain can generate or amplify pain on its own. This idea is central to modern accounts of chronic pain, including central sensitization and so-called nociplastic pain, where the pain-processing system itself becomes the problem. It remains a guiding theoretical framework rather than a complete map of the brain, but it gives a coherent way to understand pain that long outlasts — or never had — an injury.
The Opioid Story: Relief and Crisis
No history of pain treatment is complete without opioids, humanity's oldest and most powerful painkillers. Opium from the poppy Papaver somniferum has eased pain for millennia, but the modern era began in the laboratory. Around 1804 the young German pharmacist Friedrich Sertürner isolated the active principle of opium — the first alkaloid ever extracted from any plant — and by 1817 he had published his human observations and named it morphine, after Morpheus, the god of dreams. The spread of injectable morphine after the invention of the hypodermic syringe in the 1850s transformed surgery and battlefield medicine.
The promise repeatedly came tangled with addiction. In 1898 the Bayer company marketed heroin (diacetylmorphine), at first promoting it as a cough remedy and, notoriously, as a supposedly less-addictive substitute for morphine — a claim that proved disastrously wrong. Across the twentieth century, semi-synthetic and synthetic opioids (oxycodone, hydrocodone, fentanyl, and others) gave clinicians precise, life-changing tools for surgical, cancer, and acute pain.
The most consequential recent chapter is the opioid crisis. Beginning in the late 1990s — a period often dated from the 1996 launch of the extended-release oxycodone product OxyContin and an accompanying push to treat pain more aggressively, under the slogan of pain as "the fifth vital sign" — prescribing of opioids for chronic non-cancer pain rose sharply in the United States. Aggressive and at times misleading marketing, combined with genuine gaps in chronic-pain care, contributed to widespread dependence, addiction, and a wave of overdose deaths that became one of the defining public-health emergencies of the early twenty-first century. The crisis reshaped pain medicine again, driving caution about long-term opioids, renewed interest in non-opioid and multidisciplinary care, and the very "chronic pain as a disease" reckoning described next. (For current treatment guidance, see the companion deep-dive articles on opioids and non-opioid medications linked in the Connections.)
Chronic Pain Becomes a Disease: ICD-11 (2019)
For most of medical history, pain — even pain lasting years — was treated as a symptom of something else: a sign pointing to a tumour, an injury, an inflamed joint. The decisive modern shift has been the recognition that when pain persists, it can become a health condition in its own right, with its own mechanisms (such as central sensitization), its own burden, and its own need for treatment, even when the original cause has healed or cannot be found. "Chronic" pain is conventionally defined as pain that lasts or recurs for more than three months.
This recognition was formalized when the World Health Organization built a dedicated chronic-pain classification into the eleventh revision of the International Classification of Diseases (ICD-11). A task force led by the IASP — with Rolf-Detlef Treede, Winfried Rief and many colleagues — created a new top-level category, MG30 "Chronic Pain," that for the first time gathers chronic-pain diagnoses in one place rather than scattering them across the manual. ICD-11 was adopted by the World Health Assembly in 2019 and came into effect on 1 January 2022.
The classification distinguishes chronic primary pain — where the pain itself is the disease, with conditions such as fibromyalgia, chronic primary low back pain, and chronic primary headache among its members — from chronic secondary pain linked to another diagnosis (for example cancer-related, post-surgical, neuropathic, or musculoskeletal pain). This is more than bookkeeping: by giving chronic pain its own codes, ICD-11 makes the condition visible to health systems, research, and insurers, validates patients whose pain has no obvious lesion, and embeds a biopsychosocial understanding of pain into official medicine. It is the institutional capstone of a long arc — from Descartes' bell-rope, through Melzack and Wall's gate, to Bonica's clinics — in which pain came to be understood not as a simple alarm bell but as a complex experience that can itself become the illness.
Research Papers and References
The list below combines landmark peer-reviewed papers in the science and classification of pain with curated PubMed topic-search links into the historical literature. Where a confident DOI or PMID exists it is given; otherwise the entry links to a PubMed topic search. Historical primary texts (Aristotle's and Galen's writings; Descartes' Treatise of Man) are named in the article as historical sources rather than as modern citations. Each link opens in a new tab.
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science. 1965;150(3699):971-979. — doi:10.1126/science.150.3699.971
- Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain. 1975;1(3):277-299. — doi:10.1016/0304-3959(75)90044-5
- Melzack R. Pain and the neuromatrix in the brain. Journal of Dental Education. 2001;65(12):1378-1382. — PMID: 11780656
- Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003-1007. — doi:10.1097/j.pain.0000000000000160
- Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the ICD-11. Pain. 2019;160(1):19-27. — doi:10.1097/j.pain.0000000000001384
- Moayedi M, Davis KD. Theories of pain: from specificity to gate control. Journal of Neurophysiology. 2013;109(1):5-12. — doi:10.1152/jn.00457.2012
- Mendell LM. Constructing and deconstructing the gate theory of pain. Pain. 2014;155(2):210-216. — doi:10.1016/j.pain.2013.12.010
- Descartes and the bell-rope: history of the specificity (Cartesian) model of pain — PubMed: Descartes and the history of pain theory
- John J. Bonica and the founding of multidisciplinary pain medicine — PubMed: Bonica and the history of pain medicine
- International Association for the Study of Pain (IASP) and the definition of pain — PubMed: IASP and the definition of pain
- Gate control theory at 50: historical reappraisal and legacy — PubMed: gate control theory at fifty years
- Friedrich Sertürner and the isolation of morphine; history of opioid analgesia — PubMed: Sertürner, morphine, and opioid history
- Origins of the United States opioid crisis: OxyContin, prescribing, and chronic pain — PubMed: history of the opioid crisis
- Central sensitization and nociplastic pain: the modern understanding of chronic pain mechanisms — PubMed: central sensitization and nociplastic pain
External Authoritative Resources
- International Association for the Study of Pain (IASP)
- WHO ICD-11 — MG30 Chronic Pain
- NINDS (NIH) — Chronic Pain Information
Connections
- Pain & Allergy
- Chronic Pain (Overview)
- Complex Regional Pain Syndrome
- Opioids for Chronic Non-Cancer Pain
- Central Sensitization & Nociplastic Pain
- Migraine
- Fibromyalgia
- Chronic Fatigue Syndrome
- All Conditions