Lewy Body Dementia
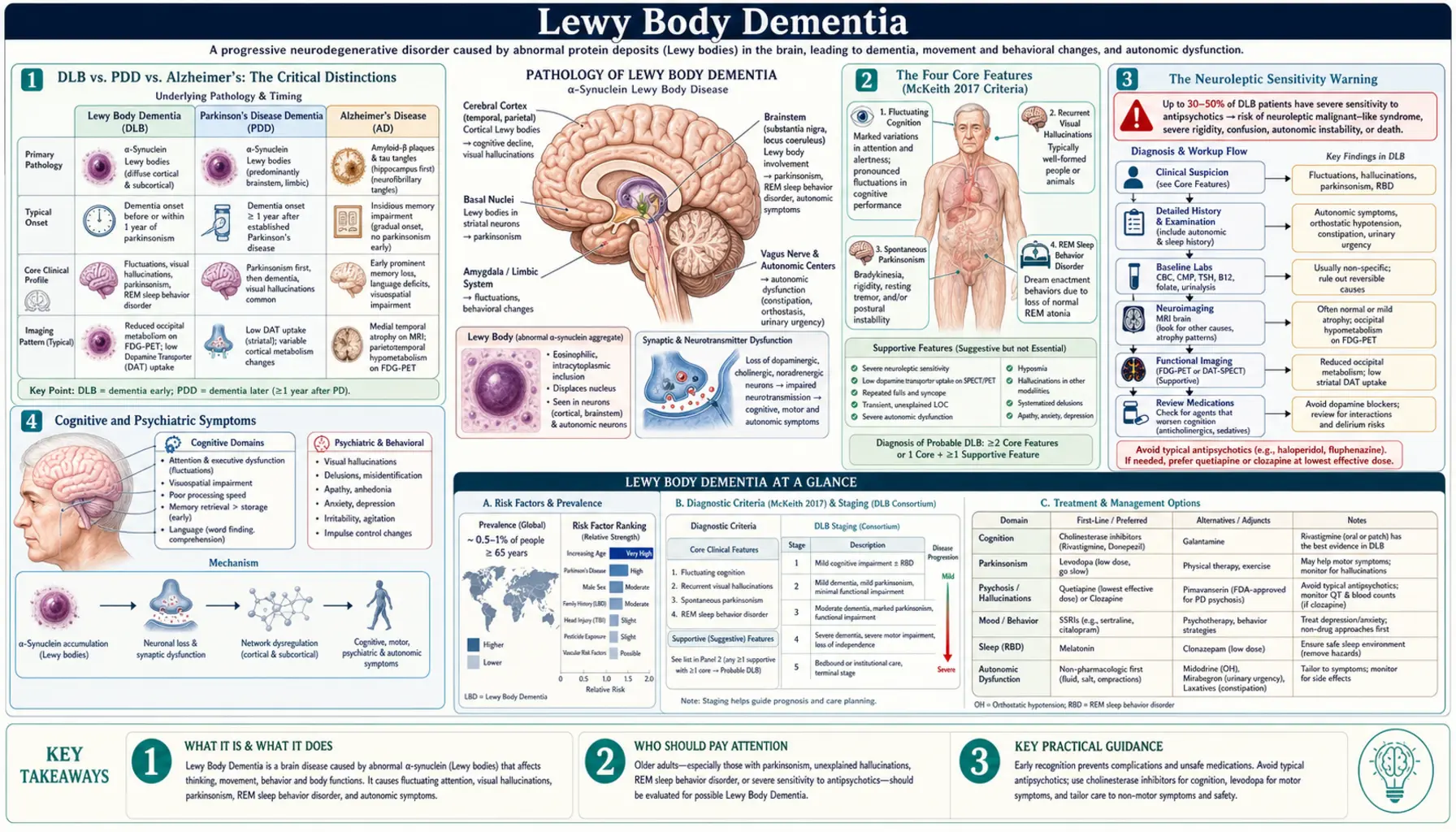
Lewy Body Dementia (LBD) is the second or third most common form of progressive dementia, affecting an estimated 1.4 million Americans and accounting for 10–15% of all dementia diagnoses. It encompasses two closely related diagnoses — Dementia with Lewy Bodies (DLB) and Parkinson's Disease Dementia (PDD) — both caused by the same underlying pathology: abnormal deposits of alpha-synuclein protein (Lewy bodies and Lewy neurites) throughout the cortex, limbic system, and brainstem. LBD is frequently misdiagnosed as Alzheimer's disease or a psychiatric illness, with an average diagnostic delay of two to four years. Early, accurate diagnosis is critical because the disease carries a unique and life-threatening drug sensitivity that every caregiver and emergency physician must know.
Table of Contents
- DLB vs. PDD vs. Alzheimer's: The Critical Distinctions
- The Four Core Features (McKeith 2017 Criteria)
- The Neuroleptic Sensitivity Warning
- Cognitive and Psychiatric Symptoms
- Diagnosis: Biomarkers and Imaging
- Management: Cholinesterase Inhibitors and Motor Symptoms
- Disease Course and Prognosis
- Practical Guidance for Patients and Caregivers
- Key Research Papers
- Connections
- Featured Videos
DLB vs. PDD vs. Alzheimer's: The Critical Distinctions
Dementia with Lewy Bodies and Parkinson's Disease Dementia sit on the same alpha-synuclein disease spectrum. The practical distinction between them rests on a single clinical rule called the one-year rule: if dementia develops within one year of the onset of parkinsonism — or before parkinsonism appears — the diagnosis is DLB. If parkinsonism has been well-established for more than one year before significant cognitive decline develops, the diagnosis is PDD. Both involve identical brain pathology; the distinction is primarily temporal and reflects the sequence in which symptoms unfold.
The contrast with Alzheimer's disease (AD) is more fundamental:
- Visual hallucinations: In DLB, vivid, well-formed visual hallucinations — typically of people, children, or animals that are "visiting" — occur early, often at diagnosis, and in 60–80% of patients. In Alzheimer's, hallucinations are a late feature appearing only in advanced stages. Families frequently call these figures "the visitors." The hallucinations are often non-threatening, and patients sometimes recognize them as not real.
- Fluctuating cognition: DLB is characterized by pronounced, spontaneous variations in attention and alertness — sometimes hour-to-hour. A patient may be engaged and conversational one moment, then stare blankly, be impossible to rouse, or seem confused for minutes to hours ("the lights-out episodes"). This fluctuation is unpredictable and distressing. Alzheimer's follows a more steady, progressive decline without these sudden waxing-and-waning episodes.
- REM sleep behavior disorder (RBD): Patients with DLB frequently act out their dreams during REM sleep — punching, kicking, shouting, or falling out of bed. RBD can precede the motor and cognitive symptoms of Lewy body disease by decades. Studies show that 80–90% of people with idiopathic RBD eventually develop a synucleinopathy (DLB, PDD, or multiple system atrophy). RBD is rarely seen in early Alzheimer's disease.
- Parkinsonism: Present in 70–80% of DLB patients, parkinsonism in DLB tends to be symmetric. Resting tremor is less prominent than in classic Parkinson's disease. Bradykinesia (slowness), rigidity, and postural instability are the more common motor features.
- Cognitive profile: DLB preferentially impairs visuospatial processing and executive function early — patients struggle with clock drawing, assembling puzzles, navigating familiar routes, and managing complex tasks. Episodic memory is relatively preserved in early DLB, contrasting with Alzheimer's, where anterograde memory failure is the hallmark presenting symptom.
The Four Core Features (McKeith 2017 Criteria)
The Fourth Consensus Report of the DLB Consortium, published in 2017 by McKeith and colleagues, updated the international diagnostic criteria for DLB. The diagnosis rests on four core clinical features and a framework of supportive biomarkers.
Core Clinical Features
- Fluctuating cognition — spontaneous alterations in concentration and alertness that vary in severity and duration.
- Recurrent visual hallucinations — typically well-formed, detailed, and complex; people and animals are most common.
- REM sleep behavior disorder (RBD) — physically acting out dreams, confirmed by history or polysomnography.
- One or more cardinal features of parkinsonism — bradykinesia, resting tremor, or rigidity.
Probable DLB requires two or more core features, or one core feature plus one or more indicative biomarkers. Possible DLB requires one core feature, or one or more indicative biomarkers alone.
Indicative Biomarkers
- Reduced dopamine transporter uptake on SPECT or PET imaging (DaTscan) in basal ganglia — present in DLB and Parkinson's disease, preserved in Alzheimer's disease and essential tremor. This is the single most useful test to distinguish DLB from AD when diagnosis is uncertain.
- Reduced MIBG uptake on myocardial scintigraphy — reflecting cardiac sympathetic denervation, highly specific for Lewy body disease.
- Polysomnographic confirmation of RBD — REM sleep without muscle atonia, with limb or body movements during REM sleep.
Supportive Biomarkers
- Positive amyloid PET or CSF amyloid pattern — concurrent Alzheimer's copathology is present in approximately 40% of DLB cases (Lewy-AD overlap), making amyloid positivity alone insufficient to exclude DLB.
Supporting Clinical Features (Not Core)
- Severe neuroleptic sensitivity — a potentially life-threatening reaction to antipsychotic medications (see the dedicated section below).
- Postural instability, repeated falls, syncope.
- Autonomic dysfunction: orthostatic hypotension, constipation, urinary symptoms.
- Hypersomnia, anosmia.
- Depression and anxiety.
The Neuroleptic Sensitivity Warning
This is the most critical safety point for anyone caring for a person with DLB or suspected LBD.
Standard antipsychotic medications — including haloperidol (Haldol), risperidone, and olanzapine — can cause severe, potentially irreversible, and sometimes fatal reactions in 30–50% of DLB patients. This is known as neuroleptic sensitivity. Symptoms include profound sedation, acute confusion, severe rigidity, immobility, autonomic instability (fever, blood pressure swings), and accelerated cognitive decline. Some patients do not recover to their pre-treatment baseline. Death has been reported.
The danger is greatest in emergency room settings, where a DLB patient brought in for acute confusion or behavioral symptoms may be given antipsychotics by a clinician unaware of the diagnosis. The same risk applies to prochlorperazine (used for nausea), metoclopramide (used for gastroparesis or nausea), and promethazine — all dopamine blockers that carry the same mechanism of toxicity.
When Hallucinations Must Be Treated
- Quetiapine (Seroquel) — the best-tolerated option in DLB due to low D2 receptor affinity; used off-label at low doses. Evidence is limited but clinical experience supports its relative safety compared to other antipsychotics.
- Clozapine — effective but requires regular blood monitoring for agranulocytosis; reserved for cases where quetiapine fails.
- Pimavanserin (Nuplazid) — a 5-HT2A inverse agonist with no dopamine receptor activity; FDA-approved for psychosis in Parkinson's disease, used off-label in DLB. It does not worsen motor symptoms. Increasingly used when hallucinations cause distress.
- Cholinesterase inhibitors (rivastigmine, donepezil) — can reduce hallucination frequency and severity in DLB and should be considered as a first-line intervention before any antipsychotic is started.
Documentation and Emergency Preparedness
Every person with a DLB diagnosis should carry a medication safety card in their wallet listing the diagnosis and the specific antipsychotics to avoid. A medical alert bracelet or necklace is strongly recommended. Family members and caregivers should rehearse communicating this warning to emergency personnel before any hospital visit. The Lewy Body Dementia Association (LBDA.org) provides a downloadable "Medical Alert Wallet Card" specifically for this purpose.
Cognitive and Psychiatric Symptoms
The cognitive and psychiatric profile of DLB is distinctive and differs meaningfully from Alzheimer's disease, especially in the early and middle stages.
Cognitive Domains Affected
- Visuospatial processing — impaired early and prominently. Patients struggle with clock drawing, jigsaw puzzles, copying geometric figures, recognizing faces, and navigating familiar environments. This reflects early involvement of posterior cortical regions (parieto-occipital cortex).
- Executive function — impaired planning, sequencing, multitasking, abstract reasoning, and problem-solving. Managing finances, cooking complex meals, or following multi-step instructions becomes difficult.
- Attention and fluctuating alertness — the hallmark "fluctuation." A patient may be engaged and answer questions clearly, then within minutes appear glazed, unresponsive, or asleep. These episodes can last seconds to hours and may be mistaken for absence seizures, transient ischemic attacks, or medication side effects. The Mayo Fluctuation Scale and the Clinician Assessment of Fluctuation (CAF) are validated rating tools.
- Episodic memory — relatively preserved in early DLB compared to Alzheimer's, though not normal. As the disease progresses, memory impairment becomes more prominent. The early memory-sparing pattern is one reason DLB is initially mistaken for something other than dementia.
Psychiatric Symptoms
- Visual hallucinations — described above; well-formed, detailed, often of people or animals. Patients may describe them as "visitors," "little people," or "the children." In early stages, insight may be partially preserved.
- Depression and anxiety — extremely common in DLB, often predating the dementia diagnosis by months to years. Depression in DLB may reflect both the underlying neurodegeneration and the distress of cognitive and motor symptoms.
- Delusions — paranoid thinking is common. A particularly characteristic delusion is the Capgras syndrome — the belief that a familiar person (spouse, caregiver) has been replaced by an impostor. Misidentification delusions are more common in DLB than in Alzheimer's.
- Hallucinations in other modalities — auditory, tactile (feeling of being touched), and olfactory hallucinations occur but are less common than visual hallucinations.
- Apathy — loss of motivation and initiative, distinct from depression; common in all dementias but prominent in LBD.
Diagnosis: Biomarkers and Imaging
No single test confirms DLB. Diagnosis rests on a combination of clinical features, history, and targeted investigations. The following tools are the most useful in current clinical practice.
DaTscan (FP-CIT SPECT)
DaTscan images the density of dopamine transporters in the striatum using a radiotracer injected intravenously. In DLB and Parkinson's disease, dopaminergic neurons are lost, producing a characteristic reduced or absent uptake pattern. In Alzheimer's disease and essential tremor, dopamine transporters are preserved. When the clinical picture is ambiguous — especially when distinguishing DLB from AD — DaTscan is the single most useful objective test. It does not differentiate DLB from PD or MSA, but it reliably separates Lewy body diseases from non-Lewy body dementias.
MIBG Myocardial Scintigraphy
Meta-iodobenzylguanidine (MIBG) scintigraphy measures cardiac sympathetic innervation. In DLB and PD, autonomic neurons supplying the heart degenerate early, producing markedly reduced cardiac MIBG uptake. This test is highly specific for Lewy body disease and is included as an indicative biomarker in the McKeith 2017 criteria. It is less widely available than DaTscan in the United States.
Polysomnography (PSG)
An overnight sleep study can confirm REM sleep behavior disorder by demonstrating REM sleep without the normal muscle atonia, along with electromyographic evidence of limb movements during REM. PSG confirmation of RBD is an indicative biomarker for DLB and is especially useful in patients who present primarily with sleep symptoms before clear cognitive or motor features develop.
MRI Brain
MRI is used primarily to exclude other causes (strokes, tumors, hydrocephalus). In DLB, hippocampal atrophy is relatively preserved compared to Alzheimer's — an important distinguishing feature. Posterior cortical atrophy (parieto-occipital) is more prominent in DLB than in typical Alzheimer's. White matter changes may be present but are non-specific.
FDG-PET
Fluorodeoxyglucose PET measures brain glucose metabolism. In DLB, hypometabolism in the occipital lobes (posterior) is characteristic and helps distinguish DLB from Alzheimer's (where temporal-parietal hypometabolism predominates). The "occipital island sign" — relative preservation of occipital metabolism — actually can paradoxically appear in DLB when compared to overall posterior hypometabolism pattern. Expert nuclear medicine interpretation is essential.
Alpha-Synuclein Skin Biopsy
An emerging diagnostic approach involves biopsying skin from the thigh or neck and staining for phosphorylated alpha-synuclein in dermal nerves. Studies show high sensitivity and specificity for synucleinopathies (DLB, PD, MSA). This test is increasingly used in research settings and is moving toward clinical availability, potentially offering a minimally invasive tissue-based diagnosis.
CSF Biomarkers
Approximately 30–40% of DLB patients show an Alzheimer's CSF pattern (low amyloid-beta 42, elevated tau), reflecting the common Lewy-AD copathology. A normal AD CSF panel does not exclude DLB. CSF alpha-synuclein measurements have not yet achieved the specificity needed for clinical diagnosis.
Management: Cholinesterase Inhibitors and Motor Symptoms
DLB has no disease-modifying treatment as of 2026. Management is symptomatic and requires careful coordination because of the overlapping cognitive, motor, psychiatric, and autonomic features — and the dangerous drug interactions unique to this disease.
Cholinesterase Inhibitors (Cognitive Symptoms and Hallucinations)
Rivastigmine is the only FDA-approved medication for Parkinson's Disease Dementia (PMID: 15590953) and is widely used off-label for DLB. Donepezil and galantamine are also used. Cholinesterase inhibitors work particularly well in DLB — possibly better than in Alzheimer's — because cholinergic deficits are more severe. They can improve attention, cognitive fluctuations, and hallucinations, making them a first-line intervention for both cognitive and psychiatric symptoms. Side effects include nausea, bradycardia (important in autonomic dysfunction), and potential marginal worsening of motor symptoms in some patients. The patch formulation of rivastigmine is better tolerated gastrointestinally than oral forms.
Levodopa (Motor Symptoms)
If parkinsonism is functionally limiting, levodopa (combined with carbidopa) can be tried. The motor response in DLB is less robust and less sustained than in idiopathic Parkinson's disease. Use the lowest effective dose, monitor carefully for increased hallucinations (levodopa can worsen psychosis), and never abruptly discontinue — abrupt withdrawal can precipitate a neuroleptic malignant syndrome-like state with fever, rigidity, and autonomic instability.
Memantine
Some evidence supports memantine (an NMDA receptor antagonist) for moderate-to-severe cognitive symptoms in DLB, though the evidence base is smaller than in Alzheimer's. It can be used alone or in combination with a cholinesterase inhibitor. It is generally well tolerated.
REM Sleep Behavior Disorder
- Melatonin 3–12 mg at bedtime — first-line treatment for RBD; safe, well-tolerated in elderly patients, no cognitive side effects. Reduces dream enactment behavior in most patients.
- Clonazepam 0.25–1 mg at bedtime — effective for RBD, but carries risks of sedation, falls, and cognitive impairment in elderly patients with dementia. Use with caution; reserve for cases where melatonin is insufficient.
Autonomic Dysfunction
- Orthostatic hypotension: increased fluid and salt intake, compression stockings, elevating the head of the bed, fludrocortisone, or midodrine. Avoid diuretics and other antihypertensives where possible.
- Urinary symptoms: avoid anticholinergic bladder medications (oxybutynin, tolterodine) — they worsen cognition significantly. Mirabegron (a beta-3 agonist) is the preferred choice for overactive bladder in LBD patients.
- Constipation: adequate hydration, dietary fiber, osmotic laxatives (polyethylene glycol). Avoid anticholinergic constipation treatments.
Caregiver Support and Multidisciplinary Care
DLB places a heavier burden on caregivers than Alzheimer's disease due to the combination of behavioral symptoms (hallucinations, delusions), motor disability (falls, immobility), rapid disease progression, and medication complexity. Physical therapy and occupational therapy address fall risk, home safety, and adaptive strategies. Speech therapy manages swallowing difficulties as disease advances. Caregiver respite, support groups, and connection to the Lewy Body Dementia Association (LBDA.org) are essential components of a complete care plan.
Disease Course and Prognosis
LBD follows a more rapid and variable course than Alzheimer's disease. Median survival from symptom onset is 5–8 years, compared to approximately 8–10 years for Alzheimer's. However, some patients survive more than a decade, while others decline rapidly within 3–4 years. Population-based incidence data from the Mayo Clinic Olmsted County Study confirmed the progressive natural history and noted a slightly higher age-adjusted incidence in men (PMID: 24100359).
Disease Trajectory
- Early stage: Cognitive fluctuations, visual hallucinations, mild parkinsonism or RBD may be present for years before diagnosis. Functional independence is largely maintained with adaptations.
- Middle stage: Increasing motor disability, falls, more pronounced cognitive impairment, behavioral symptoms requiring management. Driving cessation is typically required. Caregiver involvement intensifies.
- Late stage: Severe dementia, immobility, dysphagia, complete dependence for activities of daily living. The fluctuating quality may persist even in late stages, making prognosis difficult to predict at individual visits.
Leading Causes of Death
- Aspiration pneumonia (most common — related to dysphagia and immobility).
- Falls and fractures (hip fracture with subsequent complications).
- Cardiovascular complications (autonomic dysfunction, orthostatic events).
- General debility and sepsis from infections.
Lewy-AD Overlap
Autopsy studies reveal that Lewy body pathology and Alzheimer's pathology co-occur in a large proportion of elderly patients — possibly the most common combined dementia pathology pattern in people over 80 (PMID: 15184608). This Lewy-AD overlap may explain why some patients respond to treatments for both conditions, and why amyloid positivity does not exclude a DLB diagnosis.
Advance Planning
Because DLB can progress more rapidly than Alzheimer's and capacity may fluctuate unpredictably, advance directive conversations — including durable power of attorney for healthcare, living will, and discussion of artificial nutrition and resuscitation preferences — should be initiated as early as possible, while the patient can fully participate. Hospice eligibility follows standard dementia criteria (inability to ambulate, limited verbal communication, recurrent infections, significant weight loss). The palliative care team should be engaged well before the terminal stage.
Practical Guidance for Patients and Caregivers
The Diagnostic Journey
Getting a DLB diagnosis typically takes two to four years from the first symptoms. The disease is frequently misdiagnosed as Alzheimer's disease (because dementia is present), psychiatric illness (because hallucinations are present), or depression (because apathy and withdrawal are early features). Advocating for a DaTscan when the diagnosis is uncertain — especially if visual hallucinations, RBD, or early parkinsonism are present — can dramatically accelerate accurate diagnosis. Referral to a memory disorders center or a behavioral neurologist experienced with Lewy body disease is strongly recommended.
Medication Safety Card
Every person with LBD should carry a wallet card listing:
- Diagnosis: Lewy Body Dementia (DLB or PDD)
- DANGEROUS — AVOID: haloperidol, risperidone, olanzapine, quetiapine in high doses, prochlorperazine, metoclopramide, promethazine, droperidol
- Emergency contact name and phone number
The Lewy Body Dementia Association provides a free downloadable version at LBDA.org.
Managing Hallucinations Without Medication
Not every hallucination requires pharmacological treatment. In early DLB, many patients experience friendly or neutral "visitors" — familiar figures who sit quietly and are not threatening. Strategies that help:
- Do not argue with or try to disprove the hallucination — this increases agitation without helping.
- Calmly acknowledge what the patient is experiencing: "I can see you are seeing someone. How does that feel?"
- Improve lighting — hallucinations are more frequent in dim or shadowy environments.
- Remove or cover mirrors — reflections frequently trigger misidentification and distressing visual experiences.
- Only consider medication when hallucinations are frightening, cause dangerous behavior, or significantly impair quality of life.
RBD Safety at Home
- Pad or move furniture away from the bed to reduce injury risk during episodes.
- Consider bed rails with padding.
- If a partner is being struck or kicked during sleep, sleeping in a separate bed is a reasonable, practical solution — not abandonment.
- Start melatonin (3–12 mg at bedtime) under physician guidance — it is the safest first-line option.
- Remove weapons or dangerous objects from the bedroom.
Driving
Visuospatial impairment combined with cognitive fluctuations makes driving dangerous earlier in DLB than in Alzheimer's disease. A formal driving evaluation by an occupational therapist certified in driver rehabilitation is the gold standard. Do not wait for a crash to raise the issue — the conversation should happen at diagnosis.
Key Resources
- Lewy Body Dementia Association (LBDA.org) — the leading patient and caregiver resource; caregiver helpline, research updates, local support groups.
- National Institute on Aging — Lewy Body Dementia — evidence-based patient information.
- Mayo Clinic — Lewy Body Dementia — clinical overview for patients.
Key Research Papers
- McKeith IG, et al. "Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium." Neurology. 2017 Jul 4;89(1):88–100. PMID: 28592453
- McKeith IG, et al. "Dementia with Lewy bodies." Lancet Neurol. 2004 Jan;3(1):19–28. PMID: 14693108
- Donaghy PC, McKeith IG. "The clinical characteristics of dementia with Lewy bodies and a consideration of prodromal diagnosis." Alzheimers Res Ther. 2014 Aug 21;6(4):46. — Search PubMed
- Walker Z, et al. "Dementia with Lewy bodies: a comparison of clinical diagnosis, FP-CIT single photon emission computed tomography imaging and autopsy." J Neurol Neurosurg Psychiatry. 2007 Nov;78(11):1176–81. PMID: 17220289
- Emre M, et al. "Rivastigmine for dementia associated with Parkinson's disease." N Engl J Med. 2004 Dec 9;351(24):2509–18. PMID: 15590953
- Ferman TJ, et al. "Dementia with Lewy bodies may present as dementia and REM sleep behavior disorder without parkinsonism or hallucinations." J Neurol Neurosurg Psychiatry. 2011;82(2):203–8. — Search PubMed
- Stinton C, et al. "Pharmacological Management of Lewy Body Dementia: A Systematic Review and Meta-Analysis." Am J Psychiatry. 2015 Aug;172(8):731–42. PMID: 26085043
- Tiraboschi P, et al. "The importance of neuritic plaques and tangles to the development and evolution of AD in human brain." Neurology. 2004 Jun 8;62(11):1984–9. — Search PubMed
- Molano J, et al. "Mild cognitive impairment associated with limbic and neocortical Lewy body disease: a clinicopathological study." Brain. 2010;133(Pt 2):540–56. — Search PubMed
- Bonanni L, et al. "EEG comparisons in early Alzheimer's disease, dementia with Lewy bodies and Parkinson's disease with dementia." Brain. 2008 Mar;131(Pt 3):690–705. PMID: 18202105
- Boot BP. "Comprehensive treatment of dementia with Lewy bodies." Alzheimers Res Ther. 2015 Oct 12;7(1):45. — Search PubMed
- Savica R, et al. "Time trends in the incidence and natural history of Lewy body dementia." JAMA Neurol. 2013 Dec;70(12):1495–501. — Search PubMed
PubMed Topic Searches
- Dementia with Lewy bodies — diagnosis
- Lewy body dementia — neuroleptic sensitivity
- DLB — alpha-synuclein biomarkers
- REM sleep behavior disorder and Lewy body disease
- Rivastigmine — Lewy body dementia treatment
Connections
- Neurology
- Alzheimer's Disease — differential diagnosis and Lewy-AD overlap
- Parkinson's Disease — PDD overlap and shared synuclein pathology
- Frontotemporal Dementia — dementia differential
- Vascular Dementia — second most common dementia
- Normal Pressure Hydrocephalus — treatable dementia differential
- Multiple System Atrophy — synucleinopathy overlap
- Restless Legs Syndrome — synucleinopathy association
- Magnesium — sleep and motor support in neurodegeneration
- Thiamine (Vitamin B1) — metabolic support in neurodegeneration
- Dementia — the umbrella syndrome LBD belongs to, and the baseline for comparing subtypes.