Creutzfeldt-Jakob Disease (CJD)
Creutzfeldt-Jakob Disease (CJD) is a rare, rapidly progressive, and invariably fatal neurodegenerative disorder caused by abnormal prion proteins. First described independently by Hans Gerhard Creutzfeldt in 1920 and Alfons Jakob in 1921, it belongs to a family of transmissible spongiform encephalopathies (TSEs) that affect both humans and animals. CJD causes sponge-like holes in brain tissue, leading to swiftly worsening dementia and death, typically within months of symptom onset. Its unique biology — an infectious agent composed entirely of misfolded protein with no nucleic acid — overturned centuries of dogma in infectious disease and earned Stanley Prusiner the 1997 Nobel Prize in Physiology or Medicine.
- Prion Biology and the "Protein-Only" Hypothesis
- Types of CJD
- Sporadic CJD: Clinical Presentation
- Variant CJD: BSE Link and Features
- Familial and Iatrogenic CJD
- Diagnosis: EEG, CSF, MRI, and RT-QuIC
- Neuropathology
- Prion Transmission and Biosafety
- Treatment and Prognosis
- Public Health and Surveillance
- Key Research Papers
- Connections
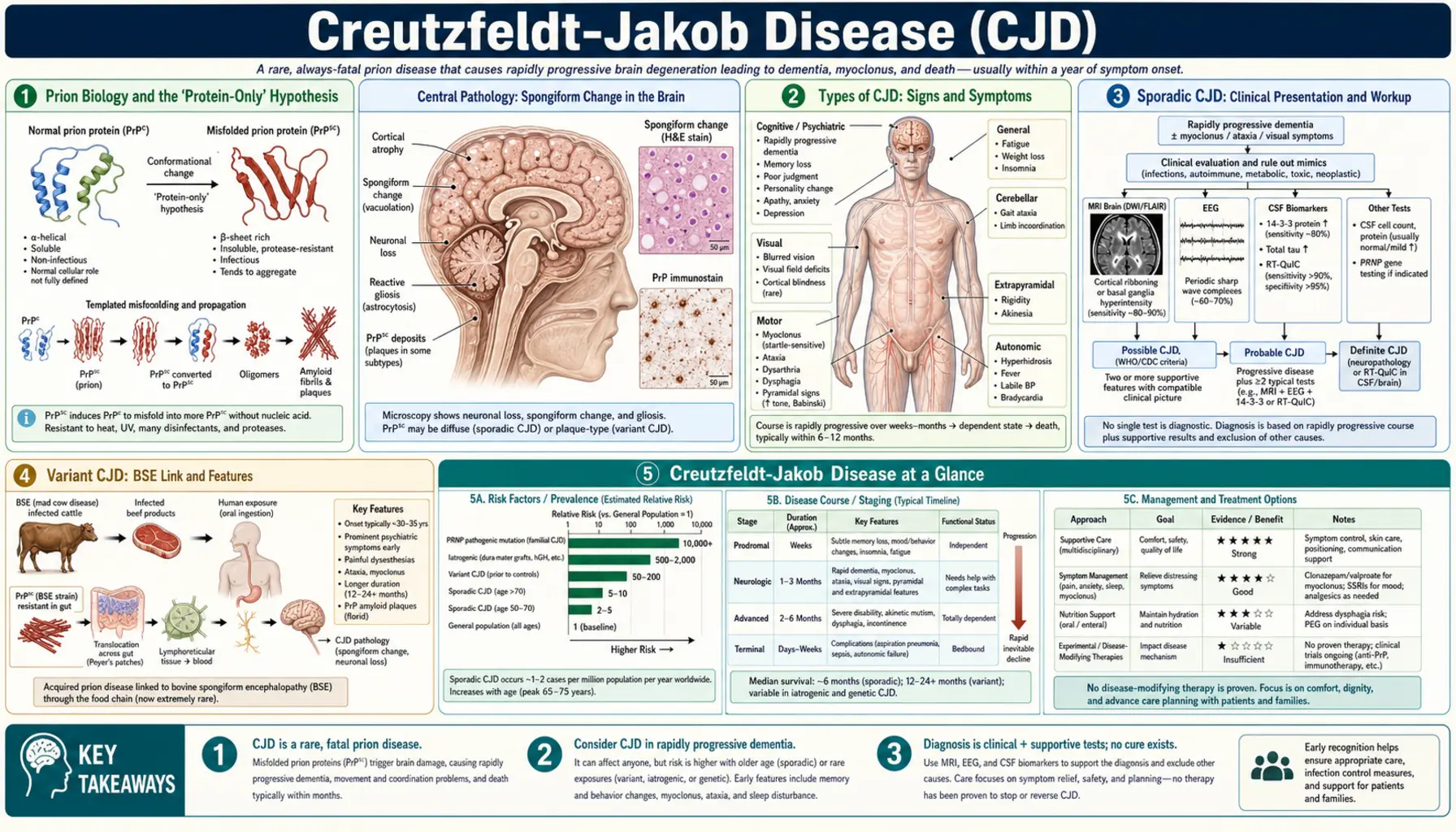
Prion Biology and the "Protein-Only" Hypothesis
Prions are infectious agents unlike any other known pathogen. They contain no DNA or RNA — they are composed entirely of a misfolded version of the cellular prion protein (PrPC). The normal prion protein, encoded by the PRNP gene on chromosome 20, is expressed throughout the body but is especially abundant in neurons. Under physiological conditions PrPC adopts a predominantly alpha-helical structure and is thought to play roles in neuroprotection, cell signaling, and copper metabolism, though its precise function remains debated.
In prion disease, a pathologically misfolded conformer called PrPSc (for scrapie, the sheep prion disease) accumulates. PrPSc has an increased proportion of beta-sheet secondary structure and is largely resistant to protease digestion, heat, ultraviolet radiation, and conventional sterilization. The critical insight of the prion hypothesis — first articulated by Prusiner in 1982 and vindicated by years of experimental evidence — is that PrPSc propagates by inducing normal PrPC molecules to adopt the misfolded conformation in a chain reaction. No nucleic acid is required for this templated conformational change, a concept that was initially met with deep skepticism from the scientific community.
Different arrangements of the misfolded protein define distinct prion "strains," which differ in their incubation periods, brain regions affected, and clinical phenotypes. Strains are stable upon passage through new hosts and are encoded not by sequence but by conformation — a remarkable biological phenomenon. Understanding prion strains is essential for explaining why CJD in humans can result from exposure to bovine spongiform encephalopathy (BSE), the cattle prion disease, when the two species have different PrP sequences. The species barrier is real but not absolute, and the variant CJD epidemic in the UK demonstrated tragically that it can be crossed.
Back to Table of ContentsTypes of CJD
CJD is classified into four major subtypes based on etiology: sporadic, familial (genetic), iatrogenic (acquired through medical procedures), and variant CJD (linked to BSE). Each has distinct epidemiological, clinical, and pathological features, though all share the common endpoint of fatal spongiform neurodegeneration. Understanding the subtype is critical for counseling, infection control, and public health investigation.
Sporadic CJD (sCJD) accounts for approximately 85–90% of all cases worldwide and has an annual incidence of roughly 1–2 cases per million population. The cause is unknown in most cases; the leading hypothesis is that a spontaneous somatic mutation in PRNP or a rare stochastic misfolding event in a single neuron initiates a cascade that spreads throughout the brain. Familial CJD (fCJD) accounts for about 10–15% of cases and is caused by autosomal dominant mutations in the PRNP gene. Dozens of pathogenic mutations have been identified, with E200K being the most common worldwide.
Iatrogenic CJD (iCJD) is now rare but historically arose from medical procedures that inadvertently transferred prion-contaminated material between individuals. The most notorious route was the use of human growth hormone extracted from cadaveric pituitary glands, which caused hundreds of cases worldwide before recombinant growth hormone replaced it in the mid-1980s. Other documented routes include dural grafts from cadaveric tissue and contaminated neurosurgical instruments. Variant CJD (vCJD) emerged in 1996 as a novel human prion disease strongly linked to the consumption of beef products contaminated with the BSE prion. It has distinct clinical and pathological features that set it apart from all other forms of CJD.
Back to Table of ContentsSporadic CJD: Clinical Presentation
Sporadic CJD typically presents in adults between 60 and 70 years of age, with a median onset around 65 years. The disease is characterized by a classic pentad of clinical features: rapidly progressive dementia, myoclonus, cerebellar ataxia, visual disturbances, and pyramidal or extrapyramidal signs. Not all features are present in every case, and the relative prominence of each depends partly on the underlying molecular subtype of sCJD, which is classified by the methionine/valine polymorphism at codon 129 of PRNP and the PrPSc fragment size on Western blot (MM1, MV1, VV2, MV2, MM2C, MM2T subtypes).
The cognitive decline in sCJD is characteristically rapid and relentless, often progressing from subtle memory complaints to severe global dementia within weeks to a few months. This tempo — far faster than Alzheimer's disease or other common dementias — is one of the most important clinical clues. Myoclonus, particularly startle myoclonus triggered by sudden sound or touch, is present in about 90% of patients at some point in the illness. Cerebellar involvement causes prominent gait ataxia and limb incoordination. Visual disturbances range from blurred vision to cortical blindness (Heidenhain variant), reflecting occipital cortex involvement.
As the disease advances, patients typically develop akinetic mutism — a state of profound unresponsiveness with preserved wakefulness — which represents end-stage cortical and subcortical devastation. Death usually follows within four to six months of symptom onset in the most common MM1 subtype. Some molecular subtypes, particularly VV2, run a longer course approaching 12 months or more. The profound rapidity of decline, the combination of cortical and cerebellar signs, and the absence of fever or systemic illness help distinguish sCJD from infectious or autoimmune encephalitides, which are critical alternative diagnoses to consider because some are treatable.
Back to Table of ContentsVariant CJD: BSE Link and Features
Variant CJD (vCJD) was first described by Will and colleagues in 1996 in a cluster of young patients in the United Kingdom with an unusual prion disease phenotype. The epidemiological, experimental, and molecular evidence that followed established beyond reasonable doubt that vCJD results from human exposure to the bovine spongiform encephalopathy (BSE) prion, likely through consumption of beef products contaminated with central nervous system tissue from infected cattle. The BSE epidemic in UK cattle peaked in the early 1990s, and the vCJD epidemic followed with an incubation lag consistent with prion biology.
The clinical features of vCJD are strikingly different from sCJD. Patients are dramatically younger — mean age at onset is approximately 28 years, compared to 65 years for sCJD — and no upper age limit has been clearly defined. The disease begins insidiously with prominent psychiatric symptoms: depression, anxiety, social withdrawal, and behavioral change, often leading to initial referral to psychiatrists rather than neurologists. Painful sensory dysesthesias are another early feature not seen in sCJD. Neurological signs, including cerebellar ataxia and involuntary movements, emerge weeks to months later. The overall disease duration is longer than sCJD, with a median survival of approximately 13 months.
A characteristic MRI finding in vCJD is bilateral symmetrical high signal in the pulvinar nucleus of the thalamus on T2 and FLAIR sequences — the "pulvinar sign" — which is present in over 75% of cases and is not seen in sCJD. All genetically confirmed cases of vCJD have been homozygous methionine (MM) at PRNP codon 129, suggesting a strong genetic susceptibility, though modeling suggests that MV and VV individuals with long incubation periods may yet develop disease. The UK has documented over 170 definite and probable vCJD cases; globally the total exceeds 230, with small numbers in France, Ireland, Italy, the United States, and Canada, mostly in individuals with UK exposure history.
Back to Table of ContentsFamilial and Iatrogenic CJD
Familial CJD is caused by autosomal dominant mutations in the PRNP gene and accounts for roughly 10–15% of all CJD cases. More than 50 pathogenic PRNP mutations have been identified worldwide. The E200K mutation is the most prevalent globally, found at particularly high frequencies in Libyan Jews and in clusters in Slovakia and Chile, reflecting founder effects. Other mutations include V180I (common in Japan), D178N (which causes fatal familial insomnia when combined with methionine at codon 129, or familial CJD when combined with valine at codon 129), and numerous insertions of octapeptide repeats in the N-terminal domain of PrP.
The clinical presentation of familial CJD can resemble sCJD, though certain mutations produce distinctive phenotypes. The age of onset is often younger than sCJD, and family history of a similar rapidly progressive dementing illness is a key diagnostic clue. Genetic counseling is important for affected families because each child of an affected individual has a 50% chance of inheriting the mutation. Penetrance is high but not always complete, and the age of onset can vary considerably even within families. Genetic testing by PRNP sequencing is available and, when positive, confirms the diagnosis without need for brain biopsy.
Iatrogenic CJD (iCJD) arose from medical procedures that inadvertently transferred prion-contaminated tissue. The largest cluster worldwide involved human growth hormone (hGH) extracted from cadaveric pituitary glands administered to children with growth hormone deficiency. More than 200 cases have been attributed to hGH treatment in the United Kingdom, France, and the United States. The use of cadaveric pituitary-derived hGH was banned in the UK and France in 1985, and the United States followed. Additional iCJD cases resulted from dural grafts (lyophilized cadaveric dura mater, particularly the Lyodura brand), corneal transplants, and contaminated neurosurgical instruments and electroencephalogram depth electrodes — the latter demonstrating that even brief contact between brain tissue and metal instruments can transmit prions that survive standard hospital sterilization. These cases drove the development of dedicated neurosurgical instrument protocols for suspected prion disease patients.
Back to Table of ContentsDiagnosis: EEG, CSF, MRI, and RT-QuIC
CJD presents a significant diagnostic challenge because no single test is definitive in life for all cases, and the combination of clinical, electrophysiological, imaging, and biomarker findings is required for probable diagnosis. Definitive diagnosis requires histopathological confirmation (immunohistochemistry or Western blot for PrPSc) from brain biopsy or autopsy. The World Health Organization (WHO) and European diagnostic criteria, most recently updated by Zerr and colleagues, stratify cases into definite, probable, and possible categories based on specific combinations of clinical features and ancillary test results.
Electroencephalography (EEG) in sCJD characteristically shows periodic sharp-wave complexes (PSWCs) occurring at roughly 1-second intervals on a background of diffuse slowing. These periodic discharges have a sensitivity of approximately 67% and specificity of around 86% for sCJD, but they are typically absent in vCJD and some other CJD subtypes. CSF analysis reveals elevated 14-3-3 protein in about 91% of sCJD patients — this protein is released from rapidly dying neurons and is a marker of acute neuronal destruction, not CJD-specific but highly sensitive in the right clinical context. CSF total tau is also markedly elevated and has been incorporated into revised diagnostic criteria as a quantitative biomarker.
Brain MRI using diffusion-weighted imaging (DWI) has become the most sensitive ante-mortem investigation, with abnormalities detectable earlier in the disease course than EEG or CSF changes. The characteristic DWI pattern in sCJD is cortical ribboning — a gyriform or ribbon-like restricted diffusion tracing the cortical surface — combined with hyperintensity in the striatum (caudate and putamen), producing the so-called "hockey stick" sign when caudate and putamen are both involved. RT-QuIC (real-time quaking-induced conversion) represents a transformative advance: this cell-free amplification assay detects minute quantities of prion seeds in CSF with reported sensitivity exceeding 97% and specificity greater than 99% in sporadic CJD, essentially making ante-mortem prion detection practical for the first time. More recently, RT-QuIC applied to nasal brushings or skin biopsies has achieved comparable performance non-invasively.
Back to Table of ContentsNeuropathology
The neuropathological hallmarks of CJD — as in all human prion diseases — are a triad of spongiform change (vacuolation of the neuropil), neuronal loss, and astrogliosis in the grey matter of the cerebral cortex, basal ganglia, thalamus, and cerebellum. The vacuoles are intracytoplasmic and appear as small, round, sharply demarcated holes in routine hematoxylin and eosin staining, giving the brain a sponge-like appearance at the microscopic level. This pattern of neurodegeneration differs fundamentally from the amyloid plaques and neurofibrillary tangles of Alzheimer's disease, the alpha-synuclein Lewy bodies of Parkinson's disease, or the TDP-43 inclusions of ALS.
Different subtypes of CJD show distinct neuropathological distributions and PrP deposition patterns. In MM1 sCJD, spongiform change is most prominent in the cerebral cortex and basal ganglia. In VV2 sCJD, thalamic involvement is severe and cerebellar ataxia dominates clinically. Variant CJD is unique in showing large, florid plaques consisting of a central core of amyloid PrP surrounded by a corona of vacuoles, resembling the kuru plaques described in the New Guinea epidemic of kuru (another human prion disease transmitted by ritual cannibalism). These florid plaques are found throughout the cerebrum and cerebellum and are essentially pathognomonic of vCJD.
PrPSc immunohistochemistry and Western blot analysis of brain tissue provide definitive confirmation of CJD at autopsy and can classify the molecular subtype. The PrPSc fragment pattern after proteinase K digestion — specifically the molecular weight of the protease-resistant core (type 1 vs. type 2) combined with the codon 129 genotype — forms the basis of the six-subtype neuropathological classification system developed by Parchi and colleagues, which correlates with clinical phenotype and prognosis. This classification has been invaluable for understanding the phenotypic diversity of sCJD and for defining the boundaries between CJD subtypes and other prion diseases such as Gerstmann-Straussler-Scheinker syndrome and fatal familial insomnia.
Back to Table of ContentsPrion Transmission and Biosafety
Prions are uniquely resistant to standard decontamination and sterilization procedures. They withstand boiling, ultraviolet irradiation, formalin fixation, alcohol, and even autoclaving at the standard 121°C cycle used in hospital settings. This extraordinary durability reflects the fact that conventional sterilization targets nucleic acids or protein tertiary structure, neither of which is the active component of prion infectivity; PrPSc can retain infectivity even after extensive denaturing. This creates serious challenges for healthcare settings, particularly for neurosurgical and ophthalmic procedures, because prions can adhere firmly to metal instruments and remain infectious after routine reprocessing.
Recommended decontamination for prion-contaminated instruments involves one of two validated approaches: either autoclaving at 134°C for 18 minutes in a prevacuum cycle (significantly more aggressive than routine sterilization), or immersion in 1 N sodium hydroxide (NaOH) or 20,000 parts per million sodium hypochlorite for at least one hour followed by thorough rinsing. Many institutions handling suspected CJD cases use single-use instruments for high-risk procedures or disposable sheath systems for stereotactic procedures. Tissues and waste from CJD patients are handled as BSL-3 materials in many jurisdictions, with specific guidelines for biopsy handling, autopsy conduct, and disposal.
Person-to-person transmission of CJD does not occur through casual contact, respiratory secretions, or fomites under ordinary circumstances. The primary routes of natural transmission are ingestion of prion-contaminated food (vCJD), iatrogenic medical exposures described above, and theoretically blood transfusion — which has been documented in at least four cases of vCJD transmission through non-leucodepleted red cell transfusions in the UK. This prompted universal leucodepletion of blood products in the UK and exclusion of donors with significant UK residence history from blood banks in many countries. No evidence currently supports airborne or contact transmission in healthcare workers, and the occupational risk appears extremely low.
Back to Table of ContentsTreatment and Prognosis
There is currently no effective disease-modifying treatment for any form of CJD. Numerous agents have been investigated in small trials and case series, including quinacrine, pentosan polysulfate, flupirtine, and doxycycline, but none has demonstrated meaningful clinical benefit in adequately powered studies. The challenge is formidable: by the time CJD is diagnosed, massive neuronal loss has already occurred, and the prion propagation cascade is well advanced. Experimental approaches including anti-PrP antibodies, PrP-lowering gene therapies, and small molecules that stabilize the native PrP conformation are under investigation, but none has yet reached clinical trial in CJD patients.
The prognosis of sCJD is uniformly fatal, with median survival of approximately four to six months from symptom onset for the most common MM1 subtype. Approximately 90% of patients die within one year. The VV2 subtype has a somewhat longer median survival, approaching 7–8 months. Familial CJD survival varies by mutation. Variant CJD has a median survival of about 13 months. There are rare documented cases of sCJD survivors exceeding two years, but these remain exceptional and the biological determinants are not well understood.
The focus of clinical management is high-quality palliative and supportive care. Myoclonus and pain may respond to clonazepam, valproate, or opiates. Seizures, when present, are treated with anticonvulsants. Psychiatric symptoms in early vCJD may be managed pharmacologically. Multidisciplinary palliative care teams are essential, and advance care planning discussions should occur early, while the patient retains decision-making capacity. Families need intensive psychological support and practical guidance on caregiving, as the rapid trajectory of the disease is devastating. Genetic counseling is indicated for families of patients with familial CJD.
Back to Table of ContentsPublic Health and Surveillance
CJD is a notifiable disease in most developed countries. In the United States, surveillance is coordinated through the National Prion Disease Pathology Surveillance Center (NPDPSC) at Case Western Reserve University, which conducts free confirmatory testing on autopsy brain tissue from suspected prion disease cases submitted from across the country. Similar national reference centers operate in the UK (National CJD Research and Surveillance Unit, Edinburgh), France, Germany, Italy, and numerous other European nations. International surveillance coordination occurs through the European Creutzfeldt-Jakob Disease Surveillance Network (EuroCJD).
Active surveillance is essential because CJD is thought to be significantly underdiagnosed and underreported globally, particularly in resource-limited settings and in cases where post-mortem examination is not performed. Accurate incidence data depend on consistent autopsy rates and awareness among clinicians. Studies from countries with comprehensive surveillance suggest the true incidence may be 1.5–2 times higher than reported rates. The incidence of sCJD has remained stable worldwide at approximately 1–2 per million per year, with no evidence of an epidemic. The vCJD epidemic in the UK has diminished substantially since its peak in 2000, with only isolated cases in recent years.
Public health concern about residual vCJD risk centers on the unknown number of individuals who may be incubating infection with very long incubation periods, possibly in genetic backgrounds other than MM at codon 129 — the only genotype seen among symptomatic vCJD cases so far. Appendix and tonsil surveys in the UK have detected PrPSc in lymphoid tissue at rates suggesting a larger pool of infected individuals than the number who developed clinical disease. Blood safety measures, deferral of donors with UK exposure history, and ongoing RT-QuIC-based screening research are components of the continuing public health response to this prion threat.
Back to Table of ContentsKey Research Papers
- Prusiner SB. Prion diseases and the BSE crisis. Science. 1997;278(5336):245–251 — Search PubMed
- Zerr I, Kallenberg K, Summers DM, et al. Updated clinical diagnostic criteria for sporadic Creutzfeldt-Jakob disease. Brain. 2009;132(10):2659–2668. PMID: 19773352
- Parchi P, Giese A, Capellari S, et al. Classification of sporadic Creutzfeldt-Jakob disease based on molecular and phenotypic analysis of 300 subjects. Ann Neurol. 1999;46(2):224–233. PMID: 10443888
- Atarashi R, Satoh K, Sano K, et al. Ultrasensitive human prion detection in cerebrospinal fluid by real-time quaking-induced conversion. Nat Med. 2011;17(2):175–178. PMID: 21278748
- Will RG, Ironside JW, Zeidler M, et al. A new variant of Creutzfeldt-Jakob disease in the UK. Lancet. 1996;347(9006):921–925. PMID: 8598754
- Sanchez-Juan P, Green A, Ladogana A, et al. CSF tests in the differential diagnosis of Creutzfeldt-Jakob disease. Neurology. 2006;67(4):637–643. PMID: 16924018
- Bizzi A, Pascuzzo R, Blevins J, et al. Evaluation of a new criterion for detecting prion disease with diffusion-weighted MRI. AJNR Am J Neuroradiol. 2020;41(7):1201–1208 — Search PubMed
- Bruce ME, Will RG, Ironside JW, et al. Transmissions to mice indicate that 'new variant' CJD is caused by the BSE agent. Nature. 1997;389(6650):498–501. PMID: 9333239
- Collinge J, Clarke AR. A general model of prion strains and their pathogenicity. Science. 2007;318(5852):930–936. PMID: 17991853
- Hermann P, Appleby B, Brandel JP, et al. Cerebrospinal fluid in Creutzfeldt-Jakob disease: from traditional to newly established biomarkers. J Alzheimers Dis. 2021;82(3):843–860 — Search PubMed
- Zerr I, Pocchiari M, Collins S, et al. Analysis of EEG and CSF 14-3-3 proteins as aids to the diagnosis of Creutzfeldt-Jakob disease. Neurology. 2000;55(6):811–815 — Search PubMed
- Foutz A, Appleby BS, Hamlin C, et al. Diagnostic and prognostic value of human prion detection in cerebrospinal fluid. Ann Neurol. 2017;81(1):79–92. PMID: 27893164
Additional literature can be found via PubMed: Creutzfeldt-Jakob disease prion sporadic CJD diagnosis variant CJD BSE RT-QuIC prion detection
Back to Table of Contents Back to Table of ContentsConnections
- Neurology
- Prion Disease
- Alzheimer's Disease
- Frontotemporal Dementia
- Huntington's Disease
- Multiple Sclerosis
- Vascular Dementia
- ALS (Amyotrophic Lateral Sclerosis)
- Normal Pressure Hydrocephalus
- Cerebellar Ataxia
- Parkinson's Disease
- Multiple System Atrophy