Diabetic Nephropathy
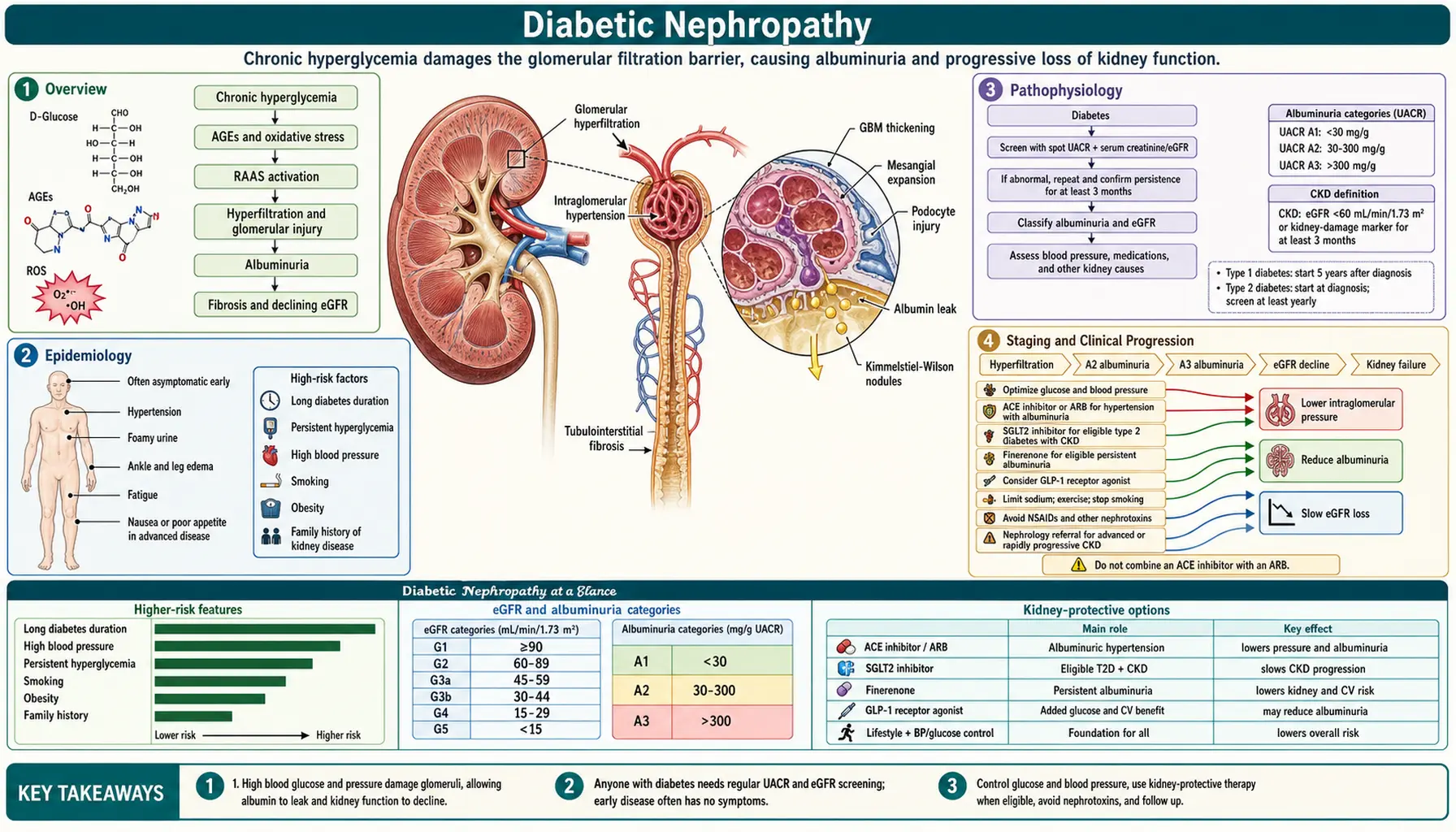
Diabetic nephropathy (DN), also called diabetic kidney disease (DKD), is the most common cause of end-stage renal disease (ESRD) in the United States and worldwide. It affects 30–40% of people with type 1 diabetes and 20–30% with type 2 diabetes over their lifetime. DN results from sustained hyperglycemia activating multiple injurious pathways in the glomerulus, leading to characteristic pathological changes — glomerular hypertrophy, basement membrane thickening, mesangial expansion, and ultimately Kimmelstiel-Wilson nodular glomerulosclerosis. It is defined clinically by progressive albuminuria and declining kidney function in the setting of diabetes, typically without need for kidney biopsy. Modern treatment with RAAS blockade, SGLT2 inhibitors, GLP-1 agonists, and finerenone has transformed the prognosis.
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Staging and Clinical Progression
- Diagnosis
- Glycemic Control and Blood Pressure
- RAAS Blockade Therapy
- SGLT2 Inhibitors and GLP-1 Agonists
- Finerenone and Novel Therapies
- Dietary and Lifestyle Management
- Prognosis and ESRD Prevention
- Research Papers (PubMed searches)
- References
- Featured Videos
Overview
Diabetic nephropathy is the leading cause of ESRD in developed countries — 44% of new ESRD cases in the US arise from diabetes, according to the USRDS 2022 Annual Report. It represents a microvascular complication of diabetes affecting the glomerular filtration barrier. Both type 1 and type 2 diabetes cause DN through the same fundamental mechanism: sustained hyperglycemia leads to glomerular hypertension, glomerular hypertrophy, and activation of pathological signaling pathways — PKC, mTOR, TGF-β, RAAS, and NF-κB — culminating in progressive glomerulosclerosis, albuminuria, and CKD.
The landmark Diabetes Control and Complications Trial (DCCT, 1993) for type 1 diabetes and the United Kingdom Prospective Diabetes Study (UKPDS, 1998) for type 2 diabetes proved that tight glycemic control prevents or delays DN development. The treatment revolution of the 2020s — SGLT2 inhibitors, finerenone, and GLP-1 receptor agonists — has dramatically reduced progression to ESRD beyond what RAAS blockade alone achieves, fundamentally changing the long-term outlook for patients with diabetic kidney disease.
Epidemiology
DN affects approximately 30–40% of type 1 diabetes patients and 20–30% of type 2 diabetes patients over 20–25 years of disease duration. In the United States, 37 million people live with diabetes; approximately 28% develop albuminuria or reduced GFR, constituting diabetic kidney disease. DN accounts for 44% of incident ESRD cases, translating to roughly 120,000 new dialysis patients per year attributable to diabetes.
Racial and ethnic disparities are pronounced. Black, Hispanic, Native American, and Pacific Islander populations experience 2–4 times higher ESRD rates compared with White Americans with diabetes. These disparities reflect inequalities in healthcare access, glycemic control, hypertension burden, and genetic susceptibility. Type 2 diabetes drives the overwhelming majority of DN burden worldwide due to its high global prevalence, which now exceeds 500 million people.
Pathophysiology
Hyperglycemia activates multiple parallel injurious pathways that converge on the glomerular filtration barrier:
- Glomerular hemodynamic changes: Hyperglycemia causes afferent arteriolar vasodilation combined with efferent arteriolar vasoconstriction (angiotensin II mediated), producing glomerular hypertension. Mechanical stress on podocytes and mesangium drives glomerular hypertrophy and hyperfiltration — an elevated GFR is characteristic of early DN.
- Advanced glycation end-products (AGEs): Glucose-derived AGEs cross-link proteins in the glomerular basement membrane (GBM), increasing thickness and reducing permeability selectivity. AGE-RAGE signaling drives oxidative stress and NF-κB activation, producing pro-inflammatory cytokines.
- Polyol pathway: Aldose reductase converts excess intracellular glucose to sorbitol, causing osmotic injury and oxidative stress. Sorbitol is subsequently converted to fructose, generating dicarbonyl stress and further AGE production.
- Protein kinase C (PKC) activation: Diacylglycerol (DAG) accumulates under hyperglycemic conditions, activating PKC isoforms. This drives TGF-β overproduction, mesangial matrix expansion, GBM thickening, podocyte apoptosis, and VEGF overproduction causing abnormal glomerular neovascularization.
- TGF-β and fibrosis pathway: TGF-β is the central driver of mesangial expansion and GBM thickening. It promotes podocyte-to-mesenchymal transition, with connective tissue growth factor (CTGF) acting as a downstream effector of progressive glomerulosclerosis.
- RAAS activation: Local intra-renal RAAS activation occurs independently of systemic RAAS status. Angiotensin II drives glomerular hypertension, TGF-β production, and inflammation. Aldosterone drives podocyte injury, interstitial fibrosis, and tubulointerstitial inflammation.
- Oxidative stress: Reactive oxygen species generated by AGE-RAGE signaling, mitochondrial dysfunction, and NAD(P)H oxidase activation cause endothelial dysfunction and podocyte injury, amplifying all other pathological processes.
- Inflammation: Macrophage infiltration, NF-κB activation, and elevated IL-6 and TNF-α levels drive tubulointerstitial inflammation and progressive fibrosis independent of glomerular injury.
- Podocyte loss: Podocytes are post-mitotic cells incapable of regeneration. Their progressive loss leads to focal segmental sclerosis. Low podocyte density on biopsy predicts rate of GFR decline and progression to ESRD.
- Kimmelstiel-Wilson (KW) nodules: Pathognomonic on kidney biopsy — hyaline material deposits in a nodular pattern in the periphery of the glomerulus (mesangial nodules of laminated matrix). Present in approximately 30% of DN biopsies; highly specific but not sensitive for DN.
Staging and Clinical Progression
DN follows a characteristic clinical trajectory described by Mogensen's 5 stages, modified for modern clinical use:
- Stage 1 — Hyperfiltration: eGFR elevated above 120–130 mL/min; glomerular hypertrophy; normal albumin excretion. This stage is present at or near diabetes onset and is partially reversible with strict glucose control.
- Stage 2 — Silent phase: Normal albuminuria (ACR <30 mg/g); early structural changes including GBM thickening and mesangial expansion visible on biopsy; eGFR normal or elevated. This phase may last 10–15 years with no clinical manifestations.
- Stage 3 — Microalbuminuria (Incipient nephropathy): Albumin-to-creatinine ratio (ACR) 30–300 mg/g. eGFR still normal; blood pressure begins to rise; this is the critical therapeutic window — RAAS blockade initiated at this stage halts progression to macroalbuminuria in 30–40% of patients and reverses albuminuria to normal in approximately 20%.
- Stage 4 — Macroalbuminuria (Overt nephropathy): ACR >300 mg/g (>300 mg/day); eGFR declining at an average of 10–15 mL/min/year without treatment; hypertension is prominent; edema develops; cardiovascular risk is markedly elevated. In type 1 DM, diabetic retinopathy is present in virtually all patients at this stage — its absence should prompt re-evaluation of the DN diagnosis.
- Stage 5 — ESRD: eGFR <15 mL/min/1.73 m²; dialysis or transplantation required. Most patients reach ESRD within 5–10 years of onset of macroalbuminuria without modern multimodal therapy.
Screening recommendations: All diabetic patients should have annual urine ACR and serum creatinine/eGFR testing. For type 2 DM, screening begins at diagnosis. For type 1 DM, screening begins 5 years after diagnosis. Confirm any abnormal ACR on 2 of 3 measurements obtained 3 months apart, excluding urinary tract infection as a confounding cause.
Diagnosis
DN is usually diagnosed clinically without kidney biopsy when the presentation is classic. Clinical diagnostic criteria include: diabetes of greater than 5–10 years duration, albuminuria (ACR >30 mg/g confirmed on 2 of 3 tests 3 months apart, excluding UTI), presence of diabetic retinopathy, and no hematuria or other features suggesting an alternative diagnosis.
Kidney biopsy is indicated when atypical features are present: active urine sediment with red blood cell casts suggesting glomerulonephritis, sudden-onset proteinuria, unusually rapid GFR decline, absence of retinopathy in type 1 DM with presumed DN, or clinical suspicion of a concurrent primary glomerular disease.
Laboratory workup:
- HbA1c and fasting glucose — assess glycemic control
- Urine albumin-to-creatinine ratio (ACR) — preferred over 24-hour urine for screening; spot ACR is well-validated
- Serum creatinine and eGFR (CKD-EPI equation) — stage CKD severity
- Electrolytes — monitor potassium, especially with RAAS blockade and eGFR <45
- CBC, lipid panel — cardiovascular risk assessment
- Urine microscopy — exclude active sediment suggesting alternative glomerular disease
Pathology on biopsy: Glomerular hypertrophy, GBM thickening, diffuse mesangial expansion (early stages), Kimmelstiel-Wilson nodules (late; pathognomonic), hyalinosis of both afferent and efferent arterioles (hyaline arteriolosclerosis — efferent involvement is specific to DN, distinguishing it from hypertensive nephrosclerosis), progressive glomerulosclerosis, and tubulointerstitial fibrosis in advanced disease.
Glycemic Control and Blood Pressure
Glycemic control is foundational in DN prevention and management. The target HbA1c is <7.0% for most patients (ADA 2024 guidelines). The DCCT trial demonstrated a 60% reduction in DN incidence with intensive glucose control in type 1 DM. The UKPDS showed a 30–35% risk reduction in type 2 DM with intensive control. Caution is required in elderly patients prone to frequent hypoglycemia, for whom less aggressive targets of HbA1c 7.5–8.0% are appropriate. Hypoglycemia itself is associated with worse cardiovascular and renal outcomes and should be actively avoided.
Blood pressure control targets <130/80 mmHg for patients with diabetes and CKD (endorsed by ADA, KDIGO, and ACC/AHA 2024 guidelines). This target reduces GFR decline rate and cardiovascular event risk. Systolic blood pressure control is more important than diastolic for renal protection. Antihypertensive therapy should be initiated promptly when blood pressure exceeds this threshold, with RAAS-based regimens as the preferred backbone.
RAAS Blockade Therapy
ACE inhibitors (captopril, lisinopril, enalapril) and angiotensin receptor blockers (losartan, irbesartan, olmesartan) are the cornerstone of DN therapy for all patients with ACR >30 mg/g, with or without hypertension. Their renoprotective effects operate through two mechanisms: reducing intraglomerular pressure by dilating the efferent arteriole, and reducing proteinuria by 30–40% through a direct antiproteinuric effect independent of blood pressure reduction.
- The IDNT trial (Lewis 2001, NEJM): irbesartan 300 mg/day reduced the risk of doubling serum creatinine by 33% versus amlodipine and by 20% versus placebo in patients with type 2 DN and macroalbuminuria.
- The RENAAL trial (Brenner 2001, NEJM): losartan 100 mg/day reduced ESRD risk by 28% versus placebo in type 2 DN over 3.4 years.
- The MICRO-HOPE substudy (2000): ramipril reduced the composite of ESRD and dialysis by 22% in high-cardiovascular-risk diabetic patients.
Dual RAAS blockade (combining ACEi with ARB) must not be used. The VA-NEPHRON-D trial showed increased AKI and hyperkalemia without additional renal benefit from the combination. Hyperkalemia is the most common complication of RAAS blockade in DN patients; monitor serum potassium closely, particularly when eGFR falls below 45 mL/min. Potassium binders such as patiromer or sodium zirconium cyclosilicate can enable continuation of RAAS blockade in patients who develop hyperkalemia.
SGLT2 Inhibitors and GLP-1 Agonists
SGLT2 inhibitors (dapagliflozin, empagliflozin, canagliflozin) represent a landmark advance in DN treatment, recommended by KDIGO 2022 for all patients with type 2 DM and CKD with eGFR ≥20 mL/min, regardless of glycemic control status.
Their renoprotective mechanism involves blockade of sodium-glucose cotransporter 2 in the proximal tubule, causing glucosuria. This reduces tubuloglomerular feedback, lowering afferent arteriolar tone and intraglomerular pressure — directly counteracting the glomerular hemodynamic abnormality central to DN. Additional benefits include weight loss, blood pressure reduction, and anti-inflammatory and anti-fibrotic effects.
- CREDENCE trial (Perkovic 2019, NEJM): canagliflozin in type 2 DM with DN and ACR 300–5,000 mg/g reduced the composite of ESRD, sustained 40% eGFR decline, and renal or cardiovascular death by 30%. The trial was stopped early for overwhelming efficacy.
- DAPA-CKD trial (Heerspink 2020, NEJM): dapagliflozin in CKD patients with eGFR 25–75 and ACR 200–5,000 mg/g — including both diabetic and non-diabetic CKD — reduced sustained GFR decline ≥50%, ESRD, or death by 44%. Dapagliflozin is now approved for non-diabetic CKD based on this result.
- EMPA-KIDNEY trial (2023, NEJM): empagliflozin across a broad CKD population reduced kidney disease progression or cardiovascular death by 28%.
GLP-1 receptor agonists (semaglutide, liraglutide, dulaglutide) provide both cardiovascular and emerging kidney protection in diabetic patients:
- LEADER trial (Marso 2016, NEJM): liraglutide reduced the composite renal outcome — new macroalbuminuria, doubling of creatinine, ESRD, or renal death — by 22% versus placebo.
- SUSTAIN-6 trial (Marso 2016, NEJM): semaglutide reduced new or worsening nephropathy by 46%.
- FLOW trial (Perkovic 2024, NEJM): semaglutide 1 mg subcutaneously weekly in patients with type 2 DM and DN (eGFR 50–75, ACR ≥300 mg/g) reduced the composite of kidney failure, sustained 50% eGFR decline, or renal and cardiovascular death by 24%. This was the first trial establishing direct kidney protection by a GLP-1 receptor agonist, independent of glucose or weight effects alone.
The mechanism of GLP-1 renoprotection involves reduced glomerular hyperfiltration, anti-inflammatory effects, weight loss reducing glomerular hypertension, and possible direct GLP-1 receptor signaling on podocytes.
Finerenone and Novel Therapies
Finerenone is a non-steroidal, selective mineralocorticoid receptor antagonist (MRA) approved by the FDA in 2021 for reducing progression of DN in adults with type 2 DM. Unlike steroidal MRAs (spironolactone, eplerenone), finerenone has higher receptor selectivity for kidney and cardiac tissue and causes significantly less hyperkalemia due to rapid tissue distribution and a non-steroidal scaffold.
Its mechanism blocks mineralocorticoid receptor (MR) overactivation in the kidney and heart — the pathway through which aldosterone drives glomerular inflammation, podocyte injury, and progressive interstitial fibrosis.
- FIDELIO-DKD trial (Bakris 2020, NEJM): finerenone versus placebo in type 2 DM with DN (ACR 30–5,000 mg/g and eGFR ≥25) reduced the composite kidney outcome — sustained ≥40% eGFR decline, ESRD, or renal death — by 18%, and reduced cardiovascular events by 14%.
- FIGARO-DKD trial (Pitt 2021, NEJM): in a similar population with greater emphasis on cardiovascular outcomes, finerenone reduced the composite of cardiovascular death, non-fatal MI, non-fatal stroke, or hospitalization for heart failure by 13%.
Finerenone is indicated as add-on therapy to RAAS blockade and SGLT2 inhibitors for patients with type 2 DM and DN, eGFR ≥25, and ACR ≥30 mg/g. The combination of an ACEi or ARB, SGLT2 inhibitor, and finerenone represents the current gold standard of DN pharmacotherapy.
Emerging therapies:
- Endothelin receptor antagonists: Sparsentan (dual endothelin/angiotensin receptor antagonist) is approved for IgA nephropathy and under study in DN. Atrasentan in the SONAR trial (de Zeeuw 2019, The Lancet) reduced the composite kidney endpoint by 35% in patients with DN selected for an acute antiproteinuric response.
- Bardoxolone methyl: An Nrf2 activator that raises eGFR by reducing filtration restriction. Phase 2 data were promising; the CARDINAL phase 3 trial in Alport syndrome informed the DN program; ongoing evaluation in DN at risk of progression.
Dietary and Lifestyle Management
Dietary and lifestyle interventions are integral to slowing DN progression and should accompany pharmacotherapy:
- Protein restriction: 0.8 g/kg/day is the standard recommended intake for patients with CKD (KDIGO 2024). Protein restriction reduces glomerular hyperfiltration. High-protein diets accelerate GFR decline and should be actively avoided. Protein intake below 0.6 g/kg/day provides no additional benefit and risks malnutrition.
- Sodium restriction: Less than 2 g of sodium per day reduces blood pressure and potentiates the antiproteinuric effect of RAAS blockade. Most processed and restaurant foods substantially exceed this target.
- Weight management: Obesity is a direct driver of glomerular hyperfiltration through adipokine-mediated and hemodynamic mechanisms. Each 10% reduction in body weight reduces proteinuria by approximately 30%. Bariatric surgery improves DN — studies show reduced albuminuria and stabilized eGFR in morbidly obese patients with type 2 DM following Roux-en-Y gastric bypass.
- Physical activity: 150 minutes per week of moderate-intensity aerobic exercise improves insulin sensitivity, reduces blood pressure, and lowers cardiovascular risk — the dominant competing cause of death in diabetic CKD.
- Smoking cessation: Smoking doubles the rate of DN progression through endothelial injury, oxidative stress, and worsening glomerular hemodynamics. Cessation measurably slows GFR decline.
- Dietary patterns: The DASH diet and Mediterranean diet both reduce CKD progression. Limit processed meats, added sugars, and excess phosphorus. Restrict dietary potassium when eGFR falls below 30 mL/min, particularly in patients on RAAS blockade and/or finerenone.
- Nephrotoxin avoidance: NSAIDs worsen DN through combined hemodynamic and direct tubulotoxic effects and should be avoided or used only briefly. Iodinated contrast media carry AKI risk — use iso-osmolar agents, ensure adequate hydration, and hold SGLT2 inhibitors for 48 hours before elective contrast procedures.
Prognosis and ESRD Prevention
Without treatment: type 1 DM patients with overt DN face approximately 50% ESRD risk over 25 years. Type 2 DM patients with DN have variable outcomes — many die of cardiovascular disease before reaching ESRD (the "competing risk" phenomenon), making cardiovascular risk reduction as important as kidney protection in this population.
With modern multimodal therapy — HbA1c <7%, ACEi or ARB, SGLT2 inhibitor, finerenone, GLP-1 receptor agonist, blood pressure <130/80, statin therapy, and lifestyle modification — ESRD rates have declined 30–40% in the US over the past 20 years. The combination of all four pillars (RAAS + SGLT2i + finerenone + GLP-1RA) is now achievable for most patients and represents the standard of care.
Cardiovascular mortality is the leading cause of death in diabetic CKD — 10–20 times higher than matched non-diabetic CKD patients. Aggressive cardiovascular risk reduction (statins, antiplatelet therapy where indicated, blood pressure control, smoking cessation) is essential and often achieves greater life-year gains than renal protection alone.
Renal replacement therapy for ESRD:
- Hemodialysis — most common modality in the US; requires vascular access (arteriovenous fistula preferred)
- Peritoneal dialysis — home-based option; suitable for motivated patients with adequate abdominal clearance
- Kidney transplant — best outcomes in eligible patients; pre-emptive transplant (before dialysis initiation) is strongly preferred over transplant after a period of dialysis, with substantially better graft and patient survival
- Simultaneous pancreas-kidney (SPK) transplant — the optimal treatment for eligible patients with type 1 DM and ESRD, restoring both glucose homeostasis and kidney function
Research Papers (PubMed searches)
- Diabetic nephropathy SGLT2 inhibitors canagliflozin empagliflozin
- Diabetic kidney disease finerenone FIDELIO FIGARO
- Diabetic nephropathy ACE inhibitor ARB RAAS
- Diabetic nephropathy GLP-1 receptor agonist semaglutide FLOW
- Diabetic nephropathy pathophysiology TGF-beta AGE RAGE
- Diabetic nephropathy HbA1c glycemic control DCCT UKPDS
- Diabetic nephropathy ESRD outcomes dialysis transplant
References
- Perkovic V, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy (CREDENCE). N Engl J Med. 2019;380(24):2295–2306. PMID: 30990260. https://doi.org/10.1056/NEJMoa1811744
- Bakris GL, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes (FIDELIO-DKD). N Engl J Med. 2020;383(23):2219–2229. PMID: 33264825. https://doi.org/10.1056/NEJMoa2025845
- Pitt B, et al. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes (FIGARO-DKD). N Engl J Med. 2021;385(24):2252–2263. PMID: 34449181. https://doi.org/10.1056/NEJMoa2110956
- Heerspink HJL, et al. Dapagliflozin in Patients with Chronic Kidney Disease (DAPA-CKD). N Engl J Med. 2020;383(15):1436–1446. PMID: 32970396. https://doi.org/10.1056/NEJMoa2024816
- Perkovic V, et al. Semaglutide and Kidney Outcomes in Type 2 Diabetes and Chronic Kidney Disease (FLOW). N Engl J Med. 2024;391(2):109–121. PMID: 38785209. https://doi.org/10.1056/NEJMoa2402285
- Lewis EJ, et al. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy Due to Type 2 Diabetes (IDNT). N Engl J Med. 2001;345(12):851–860. PMID: 11565517. https://doi.org/10.1056/NEJMoa011303
- Brenner BM, et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy (RENAAL). N Engl J Med. 2001;345(12):861–869. PMID: 11565518. https://doi.org/10.1056/NEJMoa011161
- EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023;388(2):117–127. PMID: 36331190. https://doi.org/10.1056/NEJMoa2204233
- Marso SP, et al. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes (LEADER). N Engl J Med. 2016;375(4):311–322. PMID: 27295427. https://doi.org/10.1056/NEJMoa1603827
- DCCT Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N Engl J Med. 1993;329(14):977–986. PMID: 8366922. https://doi.org/10.1056/NEJM199309303291401
- Thomas MC, et al. Diabetic kidney disease. Nat Rev Dis Primers. 2015;1:15018. PMID: 27188854. https://doi.org/10.1038/nrdp.2015.18
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022;102(5S):S1–S127. PMID: 36272764. https://doi.org/10.1016/j.kint.2022.06.008
Connections
- Nephrology & Hepatology
- Chronic Kidney Disease
- Acute Kidney Injury
- Nephrotic Syndrome
- Glomerulonephritis
- Membranous Nephropathy
- FSGS
- Lupus Nephritis
- Kidney Stones
- Kidney Function Tests
- Urinalysis
- Astragalus for Kidney & Diabetic Nephropathy
- Type 2 Diabetes — drives the overwhelming majority of diabetic nephropathy worldwide, and 20–30% of these patients develop kidney disease.