Whipple's Disease
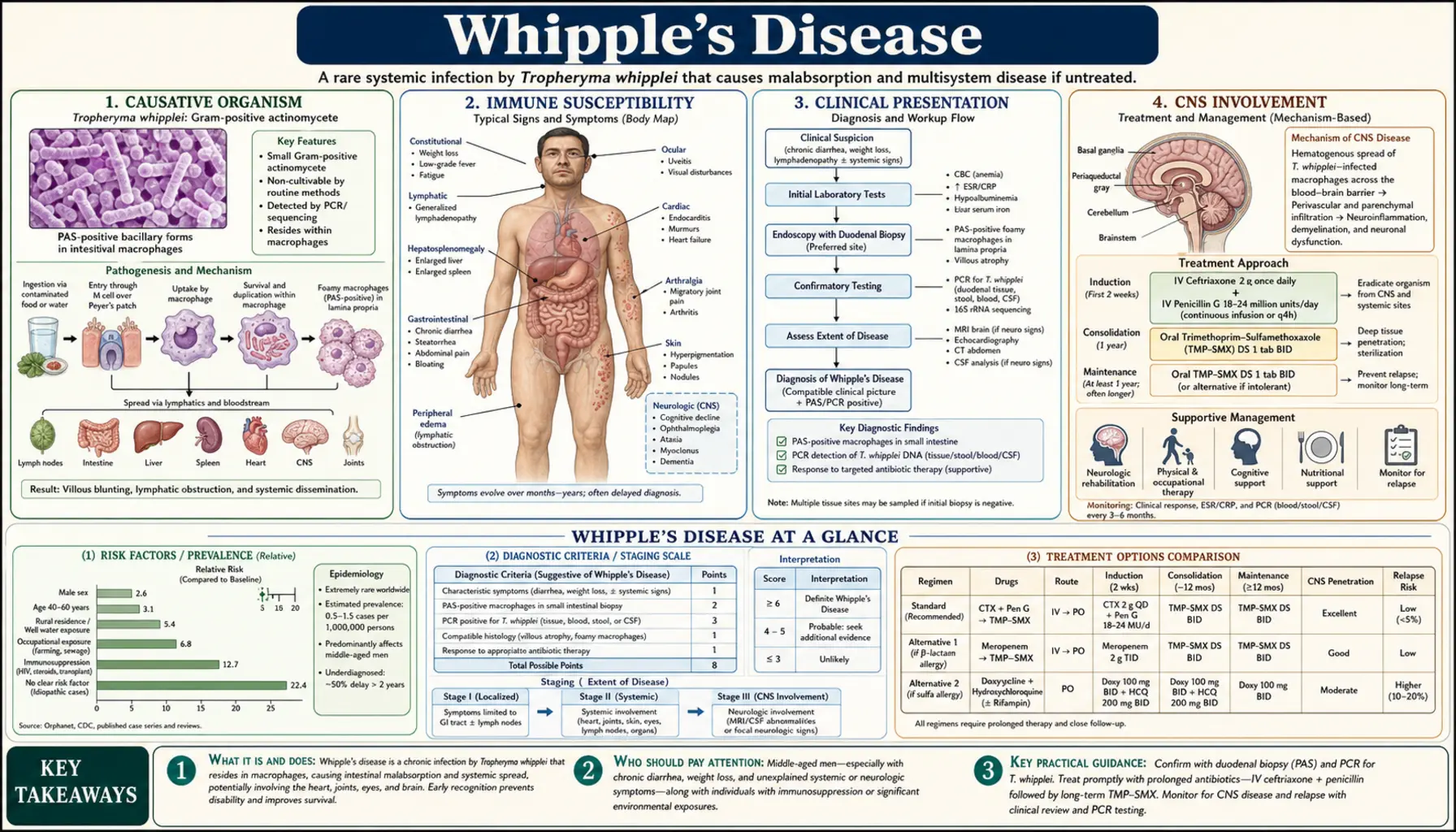
Whipple's disease is a rare, chronic, systemic bacterial infection caused by Tropheryma whipplei — a slow-growing intracellular gram-positive actinomycete that most frequently attacks the small intestine but can invade virtually any organ system. Often called the great imitator, it mimics rheumatoid arthritis for years before gastrointestinal symptoms emerge, and in its most dangerous form it causes progressive neurological destruction that is irreversible without prolonged antibiotic therapy. Worldwide prevalence is estimated at fewer than 1 case per million people per year, yet the true burden may be higher because it is chronically misdiagnosed. Without treatment it is uniformly fatal.
- Causative Organism
- Immune Susceptibility
- Clinical Presentation
- CNS Involvement
- Diagnosis
- Differential Diagnosis
- Treatment and Duration
- Relapse and Monitoring
- Prognosis
- Research Papers
- Connections
Causative Organism
Tropheryma whipplei (formerly called Tropheryma whippelii) is a gram-positive actinomycete belonging to the class Actinobacteria. It was first identified histologically in 1907 by George Hoyt Whipple, who described rod-shaped organisms in macrophage-filled intestinal lymph nodes. The organism was not successfully cultured until 2000, and robust culture protocols were not standardized until 2019 — a 90-year gap that profoundly delayed understanding of the disease.
The bacterium has a reduced genome (approximately 925 kb) consistent with an obligate intracellular lifestyle. It lacks genes for several biosynthetic pathways, making it dependent on the host cell for amino acids, nucleotides, and lipids. This intracellular survival strategy is central to pathogenesis: T. whipplei replicates within macrophage phagolysosomes, escaping normal bacterial clearance by blocking phagolysosomal acidification and inhibiting the oxidative burst.
Despite its extreme rarity as a disease-causing agent, the organism is widespread in the environment. Epidemiological studies have detected T. whipplei DNA by PCR in sewage (up to 25% of samples), soil, and the saliva of asymptomatic adults (1–11% prevalence). This wide environmental distribution and the rarity of clinical disease strongly suggest that the vast majority of exposed individuals clear the bacterium without consequence, and only those with a specific host immune defect progress to systemic Whipple's disease.
Immune Susceptibility
Whipple's disease is not a contagious epidemic illness. Community clusters and person-to-person transmission have not been documented. The critical determinant of disease is host immune susceptibility, not infectious dose or exposure frequency. Understanding why certain individuals are at risk while others remain unaffected despite widespread environmental exposure is the central unsolved question in Whipple's disease research.
Several immune defects have been identified in patients with Whipple's disease:
- HLA associations: HLA-B27 (also associated with ankylosing spondylitis and reactive arthritis) is significantly overrepresented in Whipple's disease patients, occurring in approximately 26–30% compared to 8% in the general population. HLA-DRB1*13 is another risk allele. These associations point toward antigen presentation defects in the adaptive immune response to T. whipplei.
- M2 macrophage polarization defect: Macrophages in Whipple's disease patients show abnormal polarization toward the anti-inflammatory M2 phenotype instead of the pro-inflammatory M1 phenotype required for bacterial killing. M2 macrophages express high levels of IL-10 (immunosuppressive) and low levels of IL-12 (needed to activate Th1 responses). This polarization defect appears intrinsic to the host rather than bacterially induced in every patient.
- Impaired CD4+ T cell response: Circulating CD4+ T cells in Whipple's disease patients show reduced antigen-specific responses to T. whipplei antigens. IL-16 (a CD4+ T cell chemoattractant) is markedly reduced in intestinal tissue of affected patients. Regulatory T cells (Tregs) may be overactive, suppressing the Th1 response needed to clear the organism.
- Low IL-12 production: Dendritic cells and macrophages from Whipple's disease patients produce less IL-12 in response to T. whipplei stimulation compared to healthy controls, blunting Th1 activation and IFN-gamma-mediated macrophage killing.
This immune susceptibility profile explains why Whipple's disease occurs predominantly in middle-aged white men (approximately 80% male, mean age 50), who may share environmental and genetic risk factors, and why the disease behaves as a chronic smoldering infection rather than an acute infectious emergency.
Clinical Presentation
Whipple's disease is classically described by the triad of diarrhea, weight loss, and arthritis — but this complete triad is present in only about half of patients at diagnosis. The disease has an insidious onset spanning years to decades, and the sequence of organ involvement creates a diagnostic journey that typically lasts 5–7 years from first symptoms to correct diagnosis.
Arthritis — The Presenting Feature in Most Patients
Joint involvement occurs in 50–90% of patients and typically precedes gastrointestinal symptoms by years to decades — an average of 6–8 years in case series. The arthritis is:
- Seronegative (negative rheumatoid factor and anti-CCP antibodies)
- Oligoarticular or migratory polyarticular, affecting large joints (knees, ankles, wrists, elbows, shoulders) more than small joints
- Episodic — attacks lasting days to weeks, often separated by long asymptomatic periods
- Non-destructive — does not erode cartilage or bone, which helps distinguish it from rheumatoid arthritis
- Often accompanied by sacroiliitis (common in HLA-B27-positive patients)
Clinical pearl: Whipple's disease should be considered in any patient with seronegative arthritis that fails to respond to conventional treatment, especially if GI symptoms or weight loss develop later.
Malabsorption Syndrome — The Central GI Feature
When gastrointestinal symptoms emerge, they dominate the clinical picture:
- Diarrhea — typically steatorrhea (pale, bulky, fatty, foul-smelling stools from fat malabsorption), 3–10 bowel movements per day
- Weight loss — often profound (10–20 kg or more), due to malabsorption of fat, protein, fat-soluble vitamins, and carbohydrates
- Abdominal pain and distension — diffuse, crampy; bloating from bacterial overgrowth and lymphatic obstruction
- Peripheral edema — from hypoalbuminemia due to protein malabsorption and lymphatic obstruction
- Anemia — from iron, folate, and B12 malabsorption; fatigue and pallor
- Hyperpigmentation — a distinctive finding in approximately 50% of patients; diffuse tan/brown skin darkening resembling Addison's disease, caused by melanin deposition (mechanism unclear)
Lymphadenopathy and Fever
Generalized or mesenteric lymphadenopathy is present in the majority of patients. Fever is common (approximately 50%) and may be the presenting complaint. The combination of fever, lymphadenopathy, and weight loss frequently triggers a lymphoma workup before Whipple's disease is considered.
Cardiac Involvement
T. whipplei is an increasingly recognized cause of culture-negative endocarditis. In large culture-negative endocarditis series, T. whipplei accounts for 3–7% of cases. Unlike classic Whipple's disease, isolated T. whipplei endocarditis may occur without any intestinal symptoms — the heart valve is the primary site of infection. It typically involves the aortic and mitral valves and can lead to valvular destruction requiring surgical replacement. Diagnosis requires PCR of excised valve tissue or serology.
CNS Involvement
Central nervous system involvement occurs in approximately 10–40% of patients and represents the most feared complication of Whipple's disease. CNS disease carries the highest risk of irreversible neurological damage and death. It can occur as part of classic systemic disease or — rarely — as isolated CNS Whipple's without intestinal manifestations.
Oculomasticatory Myorhythmia — The Pathognomonic Sign
Oculomasticatory myorhythmia (OMM) is one of the most specific clinical signs in all of neurology — its presence is virtually diagnostic of CNS Whipple's disease. OMM consists of:
- Pendular vergence oscillations of the eyes — rhythmic, slow (approximately 1 Hz), synchronous convergent-divergent movements of both eyes
- Synchronous jaw myoclonus — rhythmic contractions of the masseter and pterygoid muscles at exactly the same 1 Hz frequency as the eye movements
- Limb myoclonus — sometimes accompanies the ocular and jaw movements
This combination of pendular vergence oscillations synchronous with jaw and limb myoclonus at 1 Hz is pathognomonic — it has not been described in any other disease. When OMM is observed, immediate workup for CNS Whipple's is warranted. However, OMM is present in only about 20% of CNS Whipple's cases; its absence does not exclude CNS involvement.
Other CNS Manifestations
- Cognitive decline and dementia — insidious onset; memory impairment, personality change, executive dysfunction; can progress to severe dementia
- Hypothalamic dysfunction — hypersomnia (excessive daytime sleepiness), hyperphagia (increased appetite), polydipsia, and temperature dysregulation from hypothalamic infiltration
- Ophthalmoplegia — paralysis of eye movements from cranial nerve or supranuclear involvement; may be isolated
- Ataxia — cerebellar involvement; gait unsteadiness, dysmetria
- Seizures — partial or generalized; in some cases the presenting CNS manifestation
- Myoclonus — action or spontaneous, involving face, limbs, or trunk (separate from OMM)
- Psychiatric symptoms — depression, anxiety, psychosis; can antedate neurological signs by months to years
MRI brain imaging in CNS Whipple's may show T2/FLAIR hyperintensities in the hypothalamus, periaqueductal gray, cortex, or white matter — but can also be normal, particularly early in the disease course. CSF analysis typically shows a mild lymphocytic pleocytosis and elevated protein. CSF PCR for T. whipplei is highly specific and should be performed when CNS disease is suspected.
Diagnosis
The diagnosis of Whipple's disease requires a high index of clinical suspicion — it is missed primarily because physicians do not think of it. The gold standard is histological examination of duodenal biopsy combined with PCR confirmation.
Upper Endoscopy and Duodenal Biopsy
Upper endoscopy with multiple duodenal biopsies is the cornerstone of diagnosis for intestinal Whipple's disease:
- Endoscopic appearance: the duodenal mucosa often has a characteristic pale-yellow shaggy or granular appearance with yellow-white plaques — caused by lymphatic dilation and macrophage accumulation in the lamina propria. This appearance is highly suggestive but not pathognomonic.
- Histology — PAS-positive macrophages: the definitive histological finding is infiltration of the small bowel lamina propria by large foamy macrophages that stain intensely with periodic acid–Schiff (PAS) stain. These macrophages are stuffed with PAS-staining glycoprotein remnants of T. whipplei — incompletely digested bacterial cell wall material. This finding is pathognomonic when present.
- Electron microscopy: ultrastructural examination reveals the characteristic trilamellar cell wall structure of T. whipplei — so-called "bacilliform bodies" — within macrophage phagosomes. No longer required for routine diagnosis but remains the historical gold standard.
- Villous atrophy: partial or complete villous flattening is frequently present, contributing to malabsorption; this can mimic celiac disease on routine hematoxylin-eosin staining.
PCR — Confirmatory and Essential
PCR amplification of the T. whipplei 16S rRNA gene from biopsy tissue, CSF, blood, or other clinical specimens confirms the diagnosis and is increasingly the primary diagnostic tool:
- PCR from duodenal biopsy has high sensitivity and specificity for intestinal disease
- CSF PCR is essential when CNS Whipple's disease is suspected — it detects CNS involvement in the absence of classic OMM and guides the choice of induction antibiotic regimen
- Blood PCR and stool PCR have lower sensitivity for systemic disease but can be useful screening tools
- Serology (IgG against T. whipplei antigens) is being developed but is not yet widely available or validated for clinical use
Workup Summary
- Upper endoscopy with multiple duodenal biopsies (≥4 samples from D2-D3) — PAS stain required, not just H&E
- PCR of biopsy material for T. whipplei 16S rRNA
- Lumbar puncture with CSF PCR for T. whipplei if any neurological or psychiatric symptoms are present
- Brain MRI if CNS disease is suspected
- Echocardiogram if culture-negative endocarditis is suspected or cardiac murmur is present
- Labs: CBC, CMP, albumin, iron studies, B12, folate, fat-soluble vitamins (A, D, E, K), stool fat quantification
Differential Diagnosis
The broad, multisystem nature of Whipple's disease creates an extensive differential diagnosis. The diagnostic odyssey is long precisely because each organ system's involvement generates its own set of alternative diagnoses.
- Rheumatoid arthritis / seronegative arthritis — most common initial misdiagnosis (6–8 years average before Whipple's is considered); Whipple's arthritis is non-destructive and seronegative, but can be treated with DMARDs that merely mask symptoms
- Celiac disease — both cause villous atrophy and malabsorption; Whipple's has PAS-positive macrophages and positive TTG-IgA is absent; biopsy is key
- Crohn's disease — transmural granulomatous inflammation; skip lesions; perianal disease; granulomas but not PAS-positive macrophages
- Tropical sprue — similar malabsorption with villous atrophy; geographic exposure history; responds to tetracycline and folic acid
- Lymphoma — fever + weight loss + lymphadenopathy; lymphoma workup is commonly initiated before Whipple's is considered
- Sarcoidosis — multisystem granulomatous disease; elevated ACE; hilar lymphadenopathy; non-caseating granulomas on biopsy
- Dementia/Alzheimer's disease — when CNS Whipple's presents with cognitive decline; treatable vs. degenerative — critical distinction
- Culture-negative endocarditis from other causes — HACEK organisms, Bartonella, Brucella, Coxiella burnetii (Q fever); PCR of valve material distinguishes
- MAC (Mycobacterium avium complex) in HIV — PAS-positive macrophages in small bowel can mimic Whipple's; acid-fast stain and PCR distinguish; common in advanced AIDS
Treatment and Duration
Treatment of Whipple's disease is prolonged — a minimum of 1–2 years — because short courses lead to relapse, particularly in CNS disease. The treatment strategy consists of induction to clear the acute bacterial burden followed by extended maintenance to prevent relapse.
Induction Therapy
Ceftriaxone 2 g IV daily for 14 days is the preferred induction regimen for all patients with confirmed or suspected CNS involvement, and for severely ill patients with systemic disease. Ceftriaxone penetrates the blood–brain barrier reliably, achieving therapeutic CSF concentrations. Some centers use meropenem or cefotaxime as alternatives.
For mild systemic disease without CNS involvement, some protocols proceed directly to oral maintenance therapy after a brief induction, but parenteral induction is increasingly favored given the difficulty in ruling out subclinical CNS disease.
Maintenance Therapy
Trimethoprim-sulfamethoxazole (TMP-SMX, co-trimoxazole) for 1–2 years is the standard maintenance regimen:
- Dose: TMP-SMX DS (160/800 mg) twice daily for at least 12 months; most experts recommend 24 months for CNS disease
- Excellent oral bioavailability and good CNS penetration
- Monitoring: CBC monthly (risk of leukopenia and megaloblastic anemia from folate antagonism), LFTs, renal function
- Folinic acid supplementation may be added to reduce TMP-SMX hematological toxicity, though this is not universally practiced
Important caution regarding TMP-SMX alone: Do not use TMP-SMX as monotherapy (without parenteral induction) in patients with CNS disease. Historically, some patients treated with TMP-SMX monotherapy for intestinal Whipple's experienced CNS relapse — likely because the drug suppressed but did not fully eradicate CNS organisms. The combination of IV ceftriaxone induction followed by extended TMP-SMX maintenance significantly reduces this risk.
Alternative Regimens
- Doxycycline + hydroxychloroquine: an emerging evidence-based alternative, particularly for T. whipplei endocarditis. Doxycycline is bacteriostatic against T. whipplei; hydroxychloroquine raises phagolysosomal pH, restoring antibiotic efficacy within macrophages (similar to its use in Coxiella Q-fever endocarditis). Used for ≥18 months.
- Penicillin G + streptomycin: the historical standard before TMP-SMX; still used in some European protocols.
- Rifampicin: may be added for refractory or relapsing CNS disease.
Response to treatment is typically dramatic: constitutional symptoms, fever, and diarrhea often improve within days to weeks of starting antibiotics. Arthritis and neurological symptoms may take months to resolve, and some neurological deficits are permanent if treatment is delayed.
Relapse and Monitoring
Relapse is one of the defining challenges of Whipple's disease management. The relapse rate after apparently successful treatment is approximately 30–40% over long-term follow-up, with most relapses occurring within 2 years of stopping antibiotics but late relapses at 5–10 years also reported.
CNS relapse is the most dangerous form of relapse. It may occur as isolated neurological deterioration without gastrointestinal recurrence, and neurological damage from relapse can be permanent. A patient who had only intestinal disease initially can relapse with CNS involvement — this is why the adequacy of CNS treatment is paramount from the outset.
Monitoring During and After Treatment
- During treatment: repeat duodenal biopsy (PAS stain + PCR) at 6 and 12 months of treatment; histological clearance of PAS-positive macrophages and PCR negativity are the treatment endpoints. Normalization of serum albumin, hemoglobin, and nutritional markers confirms functional recovery of intestinal absorption.
- After treatment completion: annual clinical assessment and duodenal biopsy for at least 5 years; CSF PCR reassessment if any neurological symptoms emerge; indefinite vigilance in patients with prior CNS disease.
- Symptomatic relapse workup: any new fever, diarrhea, weight loss, joint symptoms, or neurological changes in a patient with prior Whipple's disease should prompt immediate endoscopy + biopsy + PCR + lumbar puncture with CSF PCR.
Some experts advocate lifelong low-dose TMP-SMX after completing the standard treatment course for patients with CNS involvement, given the severity and irreversibility of CNS relapse. Evidence is largely observational.
Prognosis
Without treatment, Whipple's disease is uniformly fatal, typically within 1–2 years of GI symptom onset from malnutrition, cachexia, and progressive organ failure. With appropriate antibiotic therapy, the prognosis is dramatically improved — the majority of patients achieve long-term remission.
Intestinal manifestations carry an excellent prognosis with treatment. GI symptoms, diarrhea, and weight loss typically resolve within weeks to months. Villous architecture gradually normalizes on serial biopsies over months to years.
Arthritis responds well to antibiotics in most patients, with joint symptoms resolving over months. Long-term joint damage is uncommon because the arthritis is non-destructive.
Neurological prognosis depends critically on timing. Neurological deficits that have been present for less than 6 months are more likely to partially or fully resolve with treatment. Deficits present for more than 1–2 years — particularly cognitive decline and oculomasticatory myorhythmia — are more likely to be permanent. Oculomasticatory myorhythmia may persist even after bacterial clearance. CNS involvement is the single most important predictor of poor long-term outcome.
Cardiac Whipple's (endocarditis) carries variable prognosis depending on extent of valve destruction. Surgical valve replacement may be required and is not contraindicated — antibiotic treatment should continue perioperatively and postoperatively for the full duration.
Research Papers
The following PubMed-indexed studies and reviews underpin current understanding of Whipple's disease pathogenesis, diagnosis, and management.
- Schneider T, et al. Whipple's disease: new aspects of pathogenesis and treatment. Lancet Infect Dis. 2008;8(3):179-190. PMID: 18291339
- Fenollar F, Puéchal X, Raoult D. Whipple's disease. N Engl J Med. 2007;356(1):55-66 — Search PubMed
- Marth T, Moos V, Müller C, Feurle GE, Schneider T. Tropheryma whipplei infection and Whipple's disease. Lancet Infect Dis. 2016;16(3):e13-22. PMID: 26856775
- Moos V, et al. Impaired immune functions of monocytes and macrophages in Whipple's disease. Gastroenterology. 2010;138(1):210-220 — Search PubMed
- Fenollar F, et al. PCR assessment of Tropheryma whipplei in 1 year of intestinal biopsy specimens from patients with Whipple disease. J Clin Microbiol. 2007;45(9):2803-2808 — Search PubMed
- Lagier JC, et al. Culture of Tropheryma whipplei from the stool of a patient with Whipple's disease. J Clin Microbiol. 2010;48(5):1892-1893 — Search PubMed
- Anderson M. Oculomasticatory myorhythmia: a unique movement disorder occurring in Whipple's disease. Ann Neurol. 1984;15(6):582-587 — Search PubMed
- Louis ED, et al. Diagnostic guidelines in central nervous system Whipple's disease. Ann Neurol. 1996;40(4):561-568 — Search PubMed
- Baisden BL, Lepidi H, Raoult D, Argani P, Yardley JH, Dumler JS. Diagnosis of Whipple disease by immunohistochemical analysis. Am J Clin Pathol. 2002;118(5):742-748 — Search PubMed
- Feurle GE, et al. Efficacy of ceftriaxone or meropenem as initial therapies in Whipple's disease. Gastroenterology. 2010;138(2):478-486 — Search PubMed
- Boulos A, et al. Doxycycline/hydroxychloroquine versus trimethoprim/sulfamethoxazole in the treatment of Whipple disease. Antimicrob Agents Chemother. 2004;48(3):747-752 — Search PubMed
- Malnick S, et al. Whipple's disease presenting as culture-negative endocarditis. Eur J Clin Microbiol Infect Dis. 2000;19(3):216-219 — Search PubMed
Connections
- Gastroenterology
- Celiac Disease
- Crohn's Disease
- Small Intestinal Bacterial Overgrowth (SIBO)
- Microscopic Colitis
- Tropical Sprue
- Autoimmune Hepatitis
- Rheumatoid Arthritis
- Dementia
- Lab Tests
- Arthritis Overview — joint inflammation is the presenting feature in most patients, often years before gut symptoms.