Autoimmune Hepatitis
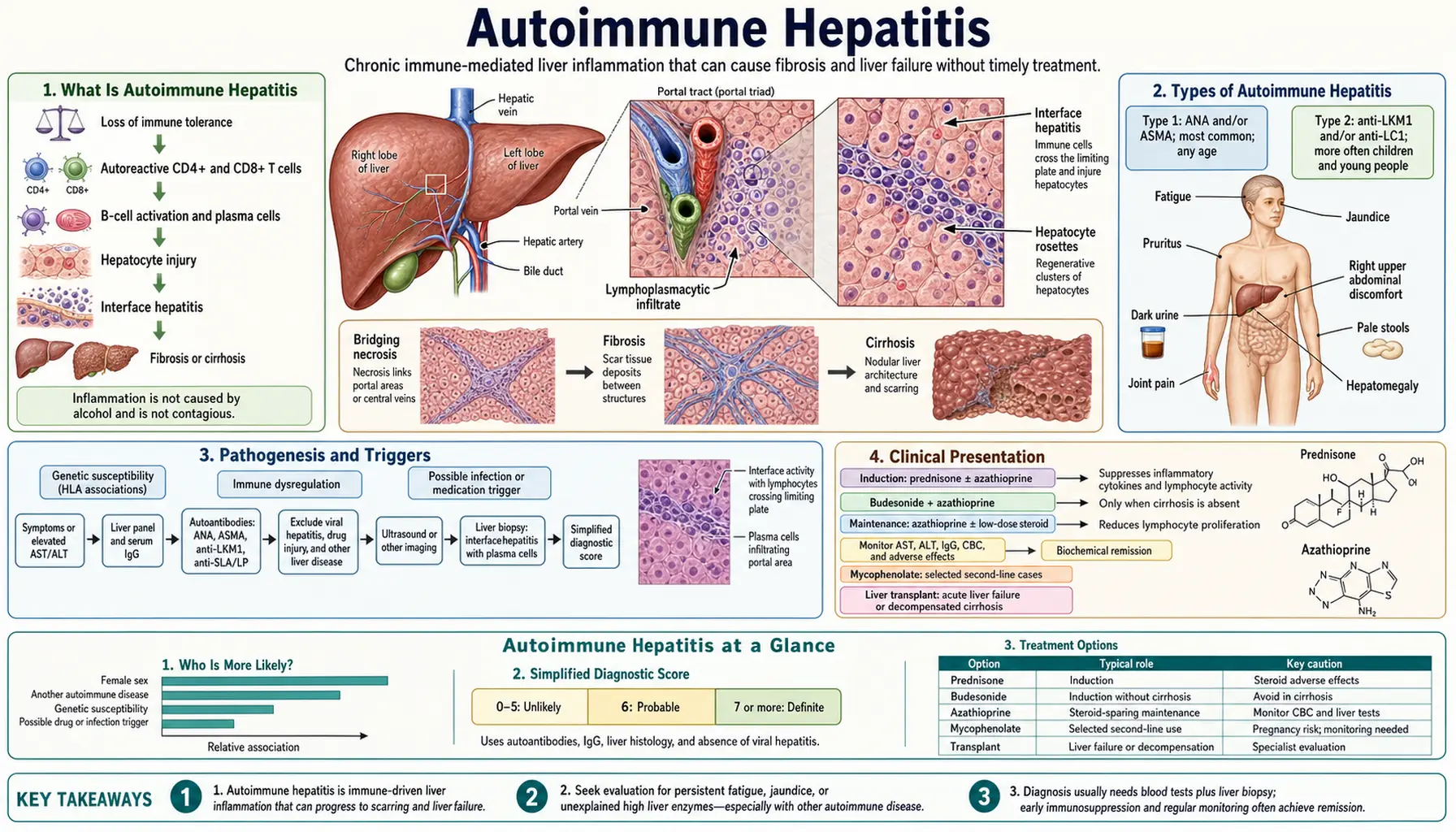
Autoimmune hepatitis (AIH) is a chronic inflammatory liver disease caused by the immune system attacking the body's own hepatocytes. It affects predominantly women (70%) and follows a bimodal age distribution — a first peak in adolescence and young adulthood, and a second peak around perimenopause. AIH can masquerade as virtually every other liver disease: it may present as acute hepatitis indistinguishable from viral infection, as chronic hepatitis discovered incidentally on blood tests, or as cirrhosis presenting with its complications. The treacherous part is that without treatment, AIH progresses silently to cirrhosis in the majority of patients — yet with the right treatment, most patients achieve complete remission and a normal life expectancy.
- Overview
- Type 1 vs Type 2 AIH
- Pathophysiology
- Clinical Presentation
- Diagnosis and the Simplified IAIHG Criteria
- Liver Biopsy and Histology
- Treatment
- Overlap Syndromes: AIH-PSC and AIH-PBC
- Research Papers
- Connections
Overview
Autoimmune hepatitis is defined by three features: (1) elevated serum transaminases (AST/ALT), typically 5–50 times the upper limit of normal; (2) characteristic autoantibodies (ANA, ASMA, anti-LKM1); and (3) interface hepatitis on liver biopsy — a histological pattern of lymphocytic and plasma cell infiltration eroding the boundary between the portal tract and the liver parenchyma (the "limiting plate"). A fourth feature, elevated immunoglobulin G (IgG), is present in 85% of patients and is an important diagnostic clue.
AIH is rare — prevalence approximately 10–20 per 100,000 in European and North American populations — but its importance lies in its treatability. Untreated, approximately 40% of patients with severe AIH die within 6 months. With standard immunosuppressive treatment, 80–90% achieve biochemical remission and 5-year survival exceeds 90%. This dramatic treatment benefit makes early recognition critical.
Key clinical associations:
- Other autoimmune diseases occur in 30–50% of AIH patients: autoimmune thyroiditis (Hashimoto's), rheumatoid arthritis, type 1 diabetes, celiac disease, vitiligo, Sjogren's syndrome
- First-degree relatives have increased rates of autoimmune diseases and elevated aminotransferases
- HLA-DR3 (DRB1*0301) and HLA-DR4 (DRB1*0401) are the two major susceptibility alleles in European-descent populations; HLA-DR3 is associated with younger age of onset and more aggressive disease
Type 1 vs Type 2 AIH
AIH is divided into two subtypes based on autoantibody profile:
Type 1 AIH (most common, ~80% of AIH)
Autoantibody markers:
- ANA (antinuclear antibody): positive at titer ≥1:40 in ~70% of Type 1 AIH patients; homogeneous or speckled pattern on immunofluorescence; non-specific (also positive in many healthy individuals, SLE, drug reactions)
- ASMA (anti-smooth muscle antibody): positive in ~70% of Type 1; specificity increases substantially at titers ≥1:80; directed against actin (F-actin specificity is most specific for AIH)
- Anti-SLA/LP (anti-soluble liver antigen/liver-pancreas): present in 10–30% of Type 1; highly specific (>99%) for AIH when positive; associated with more severe disease and higher relapse rate
- Type 1 can occur at any age; accounts for the majority of adult and elderly AIH
Type 2 AIH (less common, ~20%, predominantly children and adolescents)
Autoantibody markers:
- Anti-LKM1 (anti-liver-kidney microsomal antibody type 1): directed against CYP2D6 (cytochrome P450 2D6); positive in ~95% of Type 2; negative in Type 1; can be induced by hepatitis C infection (HCV can trigger anti-LKM1 — always check HCV in anti-LKM1-positive patients)
- Anti-LC1 (anti-liver cytosol antibody type 1): directed against formiminotransferase cyclodeaminase; often co-positive with anti-LKM1; can be the sole marker in Type 2
- Type 2 AIH tends to present more acutely, at younger ages (2–14 years most typical), with higher severity at presentation
- Type 2 has higher rate of progression to cirrhosis if untreated
Practical note: Type 1 and Type 2 are not distinguished by treatment — both receive the same prednisolone ± azathioprine protocol. The distinction matters for diagnostic workup and for understanding disease behavior.
Pathophysiology
AIH results from breakdown of immune tolerance to hepatocyte antigens, mediated by both defective regulatory T cells (Tregs) and aberrant effector immune responses.
Molecular Mimicry Hypothesis
Environmental triggers (viruses, drugs, environmental antigens) present peptide sequences that share structural similarity with hepatocyte proteins. CYP2D6 in Type 2 AIH is a clear example: a peptide from the hepatitis C virus (HCV) mimics the CYP2D6 epitope targeted by anti-LKM1, potentially explaining how HCV infection can trigger Type 2 AIH. Measles virus and herpes simplex virus have also been proposed as molecular mimics for other AIH autoantigens.
Defective Regulatory T Cell (Treg) Suppression
Tregs normally suppress autoreactive effector T cells. In AIH, Tregs are quantitatively reduced in peripheral blood and liver, and functionally impaired — they fail to suppress CD4+ and CD8+ T cells that recognize hepatocyte antigens. Mutations in FoxP3 (the master transcription factor of Tregs) and IL-2 signaling pathways (shared with Type 1 diabetes) account for part of this defect.
Th1/Th17 Effector Response
Autoreactive CD4+ T helper cells in AIH are skewed toward Th1 (producing IFN-γ and TNF-α) and Th17 (producing IL-17) phenotypes. These cytokines activate:
- Macrophage and Kupffer cell cytotoxicity against hepatocytes
- CD8+ cytotoxic T lymphocyte killing of hepatocytes expressing the autoantigens on MHC class I
- B cell production of autoantibodies (ANA, ASMA, anti-LKM1) — the antibodies themselves are largely epiphenomenal (markers, not primary drivers) but serve as diagnostic surrogates
Plasma Cell Infiltration
A distinctive feature of AIH histology is hepatic plasma cell infiltration. Activated B cells mature into plasma cells within the liver, producing local IgG that is reflected in the elevated serum IgG. This polyclonal IgG elevation (IgG typically 1.5–3× ULN in active AIH) is a key diagnostic feature and a biomarker of treatment response (IgG normalizes with effective immunosuppression).
Genetic Architecture
HLA-DR3 and HLA-DR4 present autoantigenic peptides on CD4+ T cells in the context of hepatic injury. HLA-DR3 (DRB1*0301) is associated with more severe disease, younger onset, and higher relapse rates; HLA-DR4 (DRB1*0401) is associated with milder disease, older onset, and better response to azathioprine. Non-HLA loci include PTPN22 (lymphocyte phosphatase, shared with RA and Type 1 DM) and SH2B3.
Clinical Presentation
AIH has three main presentations:
1. Acute Hepatitis Presentation (30–40% of Cases)
- Sudden onset jaundice, fatigue, right upper quadrant pain, sometimes nausea/vomiting
- Transaminases strikingly elevated: AST/ALT typically 10–100× ULN
- May be mistaken for acute viral hepatitis (HAV, HBV, EBV) without careful antibody workup
- "Acute severe" AIH: subset presenting with INR >1.5 and encephalopathy — liver failure risk is high; biopsy urgently needed to confirm diagnosis before initiating high-dose steroids (or determine whether transplant is needed)
- ~5–10% of patients develop acute liver failure requiring emergency transplantation
2. Chronic Asymptomatic Presentation (30–50% of Cases)
- Discovered incidentally during routine blood tests or workup for fatigue
- ALT/AST elevated 3–10× ULN
- No jaundice, no abdominal symptoms
- Many of these patients are found to have advanced fibrosis or cirrhosis on biopsy — the disease was silently progressing for years
3. Presentation with Established Cirrhosis
- First presentation as cirrhosis complications: ascites, variceal hemorrhage, hepatic encephalopathy
- Transaminases may be normal or only mildly elevated if hepatocyte mass is significantly reduced
- AIH must be considered in any patient with "cryptogenic" cirrhosis — unrecognized burned-out AIH is a common finding in transplant explants
Physical Examination
- Jaundice and scleral icterus (in acute or decompensated presentations)
- Hepatomegaly (tender in acute presentations)
- Spider angiomata, palmar erythema (chronic disease / cirrhosis)
- Other autoimmune disease findings: thyroid enlargement, joint swelling/tenderness, skin depigmentation (vitiligo)
Laboratory Pattern
- ALT > AST (hepatocellular pattern, not cholestatic)
- ALP and GGT: normal or mildly elevated unless overlap with PSC or PBC
- Elevated IgG: often 1.5–3× ULN; can be dramatically elevated (>30 g/L) in acute severe disease
- Low platelets and albumin if cirrhosis present
- Normal or mildly elevated bilirubin unless acute or decompensated
Diagnosis and the Simplified IAIHG Criteria
AIH diagnosis requires integrating clinical, serological, and histological data. The International Autoimmune Hepatitis Group (IAIHG) has published two scoring systems: the original complex scoring system and the simplified 2008 criteria.
IAIHG Simplified Criteria (2008)
| Variable | Finding | Points |
|---|---|---|
| ANA or ASMA | ≥1:40 | +1 |
| ANA or ASMA | ≥1:80 | +2 |
| Anti-LKM1 | ≥1:40 | +2 |
| Anti-SLA/LP | Positive | +2 |
| IgG | >ULN | +1 |
| IgG | >1.10 × ULN | +2 |
| Liver histology | Compatible with AIH | +1 |
| Liver histology | Typical of AIH | +2 |
| Absence of viral hepatitis | Yes | +2 |
Score Interpretation
- ≥7 points: definite AIH (sensitivity 85%, specificity 97%)
- 6 points: probable AIH (sensitivity 90%, specificity 90%)
- <6 points: AIH unlikely
Practical Workup Sequence
- Exclude viral hepatitis: HAV IgM, HBsAg, HBcAb IgM, HCV Ab (with reflex RNA if positive), HEV IgM
- Check ANA (IF on Hep-2 cells), ASMA (IF), anti-LKM1 (IF), anti-SLA/LP (ELISA)
- Measure IgG (and IgA, IgM to assess pattern)
- Liver biopsy (virtually always required for definitive diagnosis and fibrosis staging)
- Abdominal ultrasound (baseline; assess liver echogenicity, portal flow)
- If cholestatic features (elevated ALP/GGT): MRCP to evaluate for overlap with PSC
Drug-Induced AIH
Many drugs cause AIH-like reactions with identical serological and histological findings: minocycline, nitrofurantoin, statins, methyldopa, hydralazine, isoniazid, alpha-methyldopa. Drug-induced AIH may resolve with drug withdrawal alone. A detailed drug history (including herbal supplements — kava, comfrey, germander have caused AIH-like drug reactions) is mandatory.
Liver Biopsy and Histology
Liver biopsy is essential in AIH for three reasons: (1) to confirm the diagnosis, (2) to stage fibrosis, and (3) to establish a histological baseline for monitoring treatment response.
Characteristic Histological Features
Interface Hepatitis (the Cardinal Lesion)
Lymphocytes and plasma cells spill from portal tracts across the limiting plate into the periportal hepatocyte parenchyma, destroying periportal hepatocytes in clusters. This periportal hepatitis eroding the limiting plate is the defining histological feature and is responsible for the "rosette" formation described below.
Plasma Cell Infiltrate
Dense plasma cell infiltration — often described as the "most striking" feature by experienced pathologists — is highly characteristic of AIH. Plasma cells are rare or absent in viral hepatitis and MASLD, making their presence a strong diagnostic pointer. In acute severe AIH, plasma cells may be sparse ("plasma-cell-poor AIH"), which can mislead the pathologist.
Hepatocyte Rosette Formation
Remaining periportal hepatocytes, hemmed in by the inflammatory infiltrate, arrange themselves in a gland-like ring (rosette) around a dilated bile canaliculus or central hepatocyte. Rosettes are not specific to AIH but are characteristic.
Emperipolesis
Lymphocytes penetrating into hepatocyte cytoplasm (lymphocyte emperipolesis) — a more specific feature of AIH when prominent; distinct from hepatocyte apoptosis which produces Councilman bodies.
Fibrosis Staging
Staged F0–F4 by the Metavir or Ishak system. Approximately 30% of newly-diagnosed AIH patients already have F3–F4 fibrosis at first biopsy, emphasizing the silent progression of untreated disease.
Treatment
AIH treatment has two phases: induction of remission and long-term maintenance.
Indications for Treatment
- Active AIH with AST ≥10× ULN, or AST ≥5× ULN + IgG ≥2× ULN, or bridging/multilobular necrosis on biopsy: treat immediately (30-day mortality 40% untreated in these groups)
- Asymptomatic AIH with interface hepatitis and ≥F2 fibrosis: treat
- Asymptomatic AIH with interface hepatitis and F0–F1: treat (prevents progression)
- AIH with F4 (cirrhosis) and active inflammation: treat cautiously
Standard Induction — IAIHG Protocol
Option 1 (preferred for women, young patients, DM2 risk):
- Prednisolone 30–40 mg/day × 2 weeks → taper by 5 mg every 2 weeks to 10 mg/day
- Simultaneously, add azathioprine 50 mg/day from week 2 → increase to 1–2 mg/kg/day once transaminases are improving (azathioprine monotherapy in active hepatitis risks worsening via immunosuppression of the regulatory arm)
- Reach maintenance: prednisolone 5–10 mg/day + azathioprine 1–2 mg/kg/day
Option 2 (monotherapy with prednisolone alone):
- Prednisolone 40–60 mg/day → taper more slowly
- Reserved for cytopenias making azathioprine risky, pregnancy (azathioprine FDA Category D), malignancy history
Budesonide (for Non-Cirrhotic AIH)
- Budesonide 3 mg three times daily (9 mg/day total) + azathioprine
- 80% first-pass hepatic extraction = fewer systemic steroid side effects (less Cushingoid appearance, osteoporosis, DM2 risk)
- Important contraindication: cirrhosis — extensive portosystemic shunting bypasses first-pass extraction, eliminating budesonide's safety advantage; prednisolone must be used in cirrhosis
Monitoring Remission
- Biochemical remission: normalization of AST, ALT, IgG, bilirubin — target within 6–12 months; IgG normalization is the most reliable marker
- Histological remission: biopsy at 3 years of biochemical remission to confirm; histological remission lags behind biochemical by 3–6 months
- Histological remission (≤minimal activity on biopsy) required before considering withdrawal of therapy
Treatment Withdrawal
- IAIHG guidelines: treatment withdrawal considered only after ≥2 years of biochemical + histological remission
- Relapse rate after withdrawal: approximately 60–80% at 3 years — most patients require lifelong treatment
- Relapse is defined as AST/ALT >3× ULN after withdrawal; reinstate prednisolone + AZA at initial doses
- After a second relapse, long-term maintenance therapy is recommended indefinitely
Second-Line Therapies (AZA Intolerance, Refractory Disease)
- Mycophenolate mofetil (MMF) 1–2 g/day: first-choice AZA-alternative; achieves remission in ~60–75% of AZA-intolerant patients
- Tacrolimus: effective for refractory AIH; monitored by trough levels; nephrotoxicity risk
- Cyclosporine: less preferred than tacrolimus; similar efficacy; more drug interactions
- Rituximab (anti-CD20): emerging option for refractory AIH; small case series; targets B cell lineage and plasma cells
- Infliximab: use with caution — TNF-alpha inhibitors can paradoxically cause drug-induced AIH in some patients
Liver Transplantation
- Indicated for AIH presenting as acute liver failure (not responding to steroids within 7 days), or decompensated AIH-cirrhosis not manageable medically
- Post-transplant outcomes: 5-year survival 80–85%
- Recurrent AIH in transplanted liver: 20–35% at 10 years; usually responds to augmented immunosuppression
Overlap Syndromes: AIH-PSC and AIH-PBC
AIH overlaps with the two other autoimmune liver diseases, PSC and PBC, in approximately 7–10% of cases. These overlap syndromes require modified treatment.
AIH-PSC Overlap
- More common in children and adolescents
- Typical: elevated AST/ALT and positive ANA/ASMA (AIH features) PLUS ALP/GGT elevation and biliary strictures on MRCP (PSC features)
- Histology: both interface hepatitis AND onion-skin periductal fibrosis (rare to find both on one biopsy)
- Treatment: prednisolone + AZA (as for AIH) — but UDCA may also be added; response to immunosuppression is better than pure PSC but worse than pure AIH; transplant rates higher than pure AIH
- Pediatric AIH-PSC ("autoimmune sclerosing cholangitis"): originally described as a childhood variant; now recognized as the juvenile form of AIH-PSC overlap
AIH-PBC Overlap (Paris Criteria Diagnosis)
Paris Criteria require at least 2 of 3 features from each disease:
- AIH features: ALT ≥5× ULN, IgG ≥2× ULN or positive ASMA, interface hepatitis on biopsy
- PBC features: ALP ≥2× ULN or GGT ≥5× ULN, positive AMA at titer ≥1:40, florid duct lesion on biopsy
- Treatment: both UDCA (13–15 mg/kg/day) AND prednisolone ± AZA; UDCA alone inadequate; prednisolone alone does not address the biliary component
Research Papers
- Manns MP et al. "Diagnosis and Management of Autoimmune Hepatitis." Hepatology 2010 (AASLD practice guidelines) — Search PubMed
- Hennes EM et al. "Simplified criteria for the diagnosis of autoimmune hepatitis." Hepatology 2008 (simplified IAIHG scoring) — Search PubMed
- European Association for the Study of the Liver. "EASL Clinical Practice Guidelines: Autoimmune hepatitis." Journal of Hepatology 2015 — Search PubMed
- Johnson PJ, McFarlane IG. "Meeting report: International Autoimmune Hepatitis Group." Hepatology 1993 (original IAIHG scoring system) — Search PubMed
- Vergani D et al. "Liver autoimmune serology: a consensus statement from the committee for autoimmune serology of the International Autoimmune Hepatitis Group." Journal of Hepatology 2004 — Search PubMed
- Lohse AW et al. "Diagnosis and differentiation of autoimmune hepatitis." Journal of Hepatology 2011 — Search PubMed
- Czaja AJ. "Diagnosis and Management of Autoimmune Hepatitis: Current Status and Future Directions." Gut and Liver 2016 — Search PubMed
- Heneghan MA et al. "Autoimmune hepatitis." Lancet 2013 — Search PubMed
- Gregorio GV et al. "Autoimmune hepatitis in childhood: a 20-year experience." Hepatology 1997 (Type 2 AIH in children) — Search PubMed
- Chazouillères O et al. "Primary biliary cirrhosis–autoimmune hepatitis overlap syndrome: clinical features and response to therapy." Hepatology 1998 (Paris criteria AIH-PBC) — Search PubMed
- Zachou K et al. "Precise classification criteria and endpoint definitions for autoimmune hepatitis." Journal of Hepatology 2013 — Search PubMed
- Mack CL et al. "Diagnosis and Management of Autoimmune Hepatitis in Adults and Children." Hepatology 2020 — Search PubMed
Connections
- Nephrology & Hepatology
- Cirrhosis
- Primary Biliary Cholangitis
- Primary Sclerosing Cholangitis
- Liver Disease
- Hepatic Encephalopathy
- MASLD
- Alcoholic Hepatitis
- Hepatitis C
- Hepatitis — the umbrella overview of liver inflammation; viral hepatitis must be excluded before AIH can be diagnosed.
- Systemic Lupus Erythematosus
- Hashimoto's Thyroiditis
- AST (Aspartate Aminotransferase)
- ALT (Alanine Aminotransferase)
- Bilirubin