Restrictive Cardiomyopathy
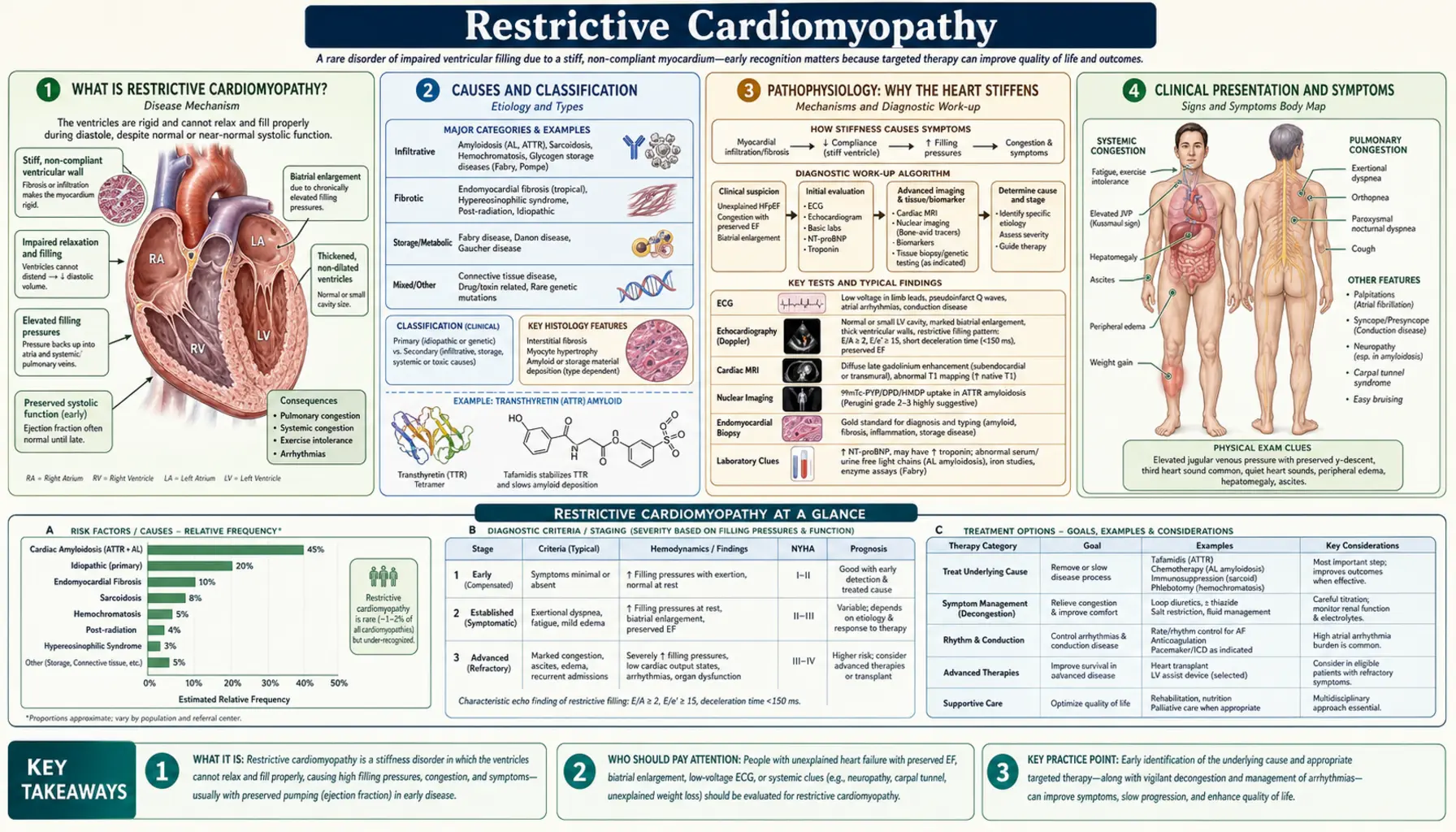
Table of Contents
- What Is Restrictive Cardiomyopathy?
- Causes and Classification
- Pathophysiology: Why the Heart Stiffens
- Clinical Presentation and Symptoms
- Diagnosis: Echo, Cardiac MRI, Catheterization
- Distinguishing RCM from Constrictive Pericarditis
- Treatment by Cause
- Prognosis and Long-Term Outlook
- Research Papers
- Connections
- Featured Videos
What Is Restrictive Cardiomyopathy?
Restrictive cardiomyopathy (RCM) is a disease of the heart muscle in which the ventricles become abnormally stiff and rigid, making it difficult for the heart to fill with blood between beats. Unlike a weak or enlarged heart — where the problem is in pumping — in RCM the squeeze (systolic function) is preserved, sometimes until late in the disease. The critical problem is that the heart cannot relax and accept blood normally. Every beat, less blood enters, and less blood leaves to the rest of the body.
Think of it this way: a healthy ventricle is like a soft rubber bulb — it fills easily and springs back with each squeeze. In RCM, that bulb becomes rigid, like a hard plastic cup. You can press it (squeeze) effectively, but it is nearly impossible to let it refill between squeezes.
RCM is the rarest of the three main cardiomyopathy types. In dilated cardiomyopathy (DCM), the heart is enlarged and weakened. In hypertrophic cardiomyopathy (HCM), the muscle wall is abnormally thickened. In RCM, the walls may look normal in thickness and size — the problem is stiffness at the cellular level, within the muscle fibers and the extracellular matrix that holds them together.
How the World Cardiology Community Classifies RCM
The European Society of Cardiology (ESC) 2023 cardiomyopathy classification defines RCM as a myocardial disorder characterized by impaired ventricular filling, with normal or reduced diastolic volumes, normal or near-normal systolic function, and normal wall thickness. Both ventricles are typically affected, and the biatrial enlargement that results is one of the most recognizable features on echocardiography. The WHO/ESC framework groups RCM alongside DCM, HCM, and arrhythmogenic cardiomyopathy as a distinct phenotype, while recognizing that RCM is often a secondary manifestation of a systemic infiltrative or storage disease rather than a primary heart muscle disorder.
Causes and Classification
RCM can arise from many different underlying diseases. Finding the cause matters enormously — because the cause determines whether a specific treatment exists. The two broadest categories are infiltrative diseases (something abnormal being deposited between the heart muscle cells) and endomyocardial diseases (fibrosis of the inner lining of the heart). A smaller group is truly idiopathic (no identifiable cause).
Infiltrative Causes (Most Common in Developed Countries)
- Cardiac amyloidosis — the most common infiltrative cause in the United States and Europe. Abnormal misfolded proteins (amyloid fibrils) are deposited in the myocardial interstitium, stiffening the walls. Two main types cause cardiac disease: AL amyloidosis (light-chain, from a plasma cell disorder) and ATTR amyloidosis (transthyretin, either hereditary or age-related "wild-type"). The classic echocardiographic appearance is "sparkling" or granular myocardial texture with thickened walls. See also Cardiac Amyloidosis.
- Cardiac sarcoidosis — non-caseating granulomas (clusters of immune cells) infiltrate the myocardium and conduction system. The heart disease in sarcoidosis is often silent until a serious arrhythmia or heart block occurs. Sudden cardiac death is a real risk even in patients with mild systolic dysfunction.
- Hemochromatosis — iron accumulates in cardiomyocytes (heart muscle cells) in patients with hereditary hemochromatosis (HFE gene mutation) or transfusion-related iron overload. Iron deposits stiffen the myocardium and are toxic to mitochondria. Critically, this is one of the few causes of RCM that can be partially reversed with early treatment (phlebotomy or iron chelation).
Storage Disease Causes
- Fabry disease — an X-linked lysosomal storage disorder caused by mutations in the GLA gene encoding the enzyme alpha-galactosidase A. Glycosphingolipids accumulate in cardiomyocytes, causing progressive wall thickening, LV hypertrophy, and eventually restrictive physiology. Enzyme replacement therapy (agalsidase alfa or beta) is available, and the oral chaperone migalastat works for amenable GLA mutations.
- Gaucher disease — glucocerebrosidase deficiency leads to glucocerebroside accumulation in macrophages; cardiac involvement is rare but can cause restrictive physiology. Enzyme replacement therapy is also available.
Endomyocardial Causes (Most Common Worldwide)
- Endomyocardial fibrosis (EMF) — the most common cause of restrictive cardiomyopathy globally, concentrated in tropical sub-Saharan Africa, South Asia, and South America. Dense fibrosis of the endocardium and subendocardium progressively obliterates the apical portions of one or both ventricles. The exact cause is not fully understood but is associated with eosinophilia, parasitic infections, and nutritional factors. Treatment is largely surgical (endocardiectomy) once advanced.
- Löffler's endocarditis — the acute inflammatory phase of endomyocardial disease driven by hypereosinophilic syndrome. Activated eosinophils release toxic granule proteins that damage the endocardium, leading to thrombus formation and eventually fibrosis identical to EMF. Treatment of the underlying eosinophilia (corticosteroids, hydroxyurea, imatinib) can prevent progression if caught early.
Other Causes
- Radiation-induced cardiomyopathy — mediastinal radiation therapy (for lymphoma, breast cancer, esophageal cancer) causes progressive myocardial fibrosis and can produce a restrictive phenotype years to decades after treatment.
- Idiopathic RCM — when no systemic cause is identified after thorough evaluation, RCM is labeled idiopathic. This group can be familial, with mutations identified in sarcomere genes including troponin I (TNNI3) and troponin T (TNNT2). It is rare, can occur in children, and carries a poor prognosis.
Pathophysiology: Why the Heart Stiffens
To understand RCM, it helps to understand normal diastole. In a healthy heart, after each beat the ventricles actively relax (an energy-requiring process) and their pressure drops rapidly, drawing blood in from the atria. The atria then contract to top off the last 20–30% of ventricular filling. This whole process happens in less than a second, and ventricular pressure stays low throughout.
In RCM, the myocardium loses its ability to relax normally. Infiltrating material (amyloid fibrils, iron, granulomas) or fibrosis of the interstitium disrupts the normal cytoskeletal and extracellular matrix architecture. The heart is like a muscle that can no longer "let go." The result is that even a small increase in blood volume entering the ventricle causes a large, disproportionate rise in filling pressure.
The Cascade of Consequences
Elevated left ventricular end-diastolic pressure (LVEDP) backs up into the left atrium — the atrium dilates trying to cope with the sustained high pressure. Elevated left atrial pressure backs up further into the pulmonary veins, causing pulmonary venous hypertension. The patient feels this as progressive dyspnea — especially with exertion, then at rest, then lying flat (orthopnea). The dilated left atrium is highly prone to atrial fibrillation, which removes the atrial "kick" that fills the stiff ventricle and often precipitates acute decompensation.
In most cases, both ventricles are involved, so right-sided filling pressures also rise — elevated right atrial pressure causes jugular venous distension, hepatomegaly, ascites, and bilateral leg edema. The hallmark of RCM on cardiac catheterization is equalization of diastolic pressures across all four chambers — right atrial pressure equals right ventricular diastolic pressure equals pulmonary capillary wedge pressure equals LVEDP, all typically 15–30 mmHg.
The Square Root Sign and Rapid Early Filling
On cardiac catheterization, the ventricular diastolic pressure tracing in RCM shows a characteristic shape called the "dip-and-plateau" or "square root sign": pressure drops sharply at the start of diastole (rapid early filling as the ventricle tries to relax) and then abruptly plateaus at an elevated level for the remainder of diastole — the plateau represents the point at which the stiff ventricle has reached the limit of its expansion and simply cannot accommodate any more volume. On echocardiography, this manifests as a very high early diastolic filling velocity (E-wave) followed by a very short deceleration time — filling goes in fast and stops fast.
Clinical Presentation and Symptoms
RCM presents differently in its early and late stages, and the initial symptoms are easy to mistake for ordinary heart failure or even a lung problem. Many patients spend years being treated for "heart failure" before RCM is identified.
Early Symptoms
- Dyspnea on exertion — the most common early symptom. The stiff heart cannot increase its output during activity; pulmonary pressures rise rapidly with exertion, causing breathlessness.
- Fatigue and exercise intolerance — the heart cannot boost cardiac output on demand, so muscles get less blood during activity.
- Ankle swelling — as right-sided pressures rise, fluid accumulates in dependent tissues.
Advanced Symptoms
- Orthopnea and paroxysmal nocturnal dyspnea — difficulty breathing when lying flat; the patient sleeps on multiple pillows or in a recliner.
- Ascites and hepatomegaly — chronic elevation of right atrial pressure causes fluid accumulation in the abdomen and liver congestion. The abdomen may become prominently distended even before significant leg edema develops.
- Cardiac cachexia — in advanced biventricular failure, patients lose muscle mass and body weight despite adequate food intake, due to poor perfusion of tissues, chronic inflammation, and gut congestion impairing nutrient absorption.
Physical Examination Findings
- Elevated jugular venous pressure (JVP) — the jugular veins are prominently distended, often visible with the patient sitting upright.
- Kussmaul's sign — a paradoxical rise in jugular venous pressure with inspiration (normally JVP falls with inspiration). This happens because the stiff ventricles cannot accommodate the increased venous return that occurs during inspiration. Kussmaul's sign is present in RCM and also in constrictive pericarditis — its absence helps distinguish cardiac tamponade from these two conditions.
- S3 or S4 gallop — extra heart sounds reflecting abnormal ventricular filling; an S4 ("Tennessee" gallop) reflects stiffness.
- Hepatomegaly and ascites — from chronic right heart failure and elevated hepatic venous pressure.
Complications That May Be the First Sign
RCM is notorious for presenting with a dramatic complication before the underlying diagnosis is made:
- Atrial fibrillation — the dilated atria are electrically unstable. AF may trigger acute hemodynamic deterioration in RCM patients because loss of atrial contraction significantly reduces filling of the non-compliant ventricle.
- Thromboembolic events — stagnant blood in dilated atria and low-flow states promote clot formation. Stroke and systemic embolism are important causes of morbidity in RCM, particularly in amyloidosis.
- Syncope and sudden cardiac death — especially in sarcoidosis (which infiltrates the conduction system), amyloidosis (both AL and ATTR), and hemochromatosis. Complete heart block and ventricular fibrillation can occur even when systolic function appears preserved.
Diagnosis: Echo, Cardiac MRI, Catheterization
No single test diagnoses RCM definitively. The diagnosis requires combining clinical findings, echocardiography, cardiac MRI (for tissue characterization), and often cardiac catheterization to confirm the hemodynamic pattern. A biopsy — of the heart, fat pad, bone marrow, or rectum — may be needed to confirm specific causes such as amyloidosis or sarcoidosis.
Echocardiography
Echo is the front-line test and the most commonly used tool. Key findings in RCM include:
- Biatrial enlargement — often dramatic; both left and right atria are dilated from chronically elevated filling pressures. This is one of the most consistent echocardiographic features of RCM.
- Normal or near-normal ejection fraction (EF) — preserved systolic function (EF typically 50–65%) until late stages. Normal or mildly thickened walls.
- Restrictive filling pattern on Doppler — E/A ratio greater than 2.0 (the early-to-late filling velocity ratio is very high because active atrial contraction contributes little to a stiff ventricle); short deceleration time (DT) less than 150 ms (the rapidly entering blood hits the rigid wall and decelerates abruptly).
- Tissue Doppler imaging (TDI) — myocardial annular velocity (e') is low (typically less than 8 cm/s) because the myocardium itself cannot relax; this is a crucial finding that helps distinguish RCM from constrictive pericarditis (where e' is preserved). The ratio of E to e' (E/e') is elevated (greater than 15), reflecting high filling pressure.
- Right ventricular dysfunction — as disease advances, RV systolic function may decline, which worsens prognosis considerably.
- In amyloidosis specifically: "sparkling" or granular myocardial texture; thickened interatrial septum; thickened valves; small pericardial effusion — a characteristic constellation that should prompt immediate suspicion for amyloid.
Cardiac MRI
Cardiac MRI has become the gold standard for tissue characterization in RCM — it can often distinguish between causes non-invasively:
- Late gadolinium enhancement (LGE) — reveals areas of scar or abnormal protein deposition. Pattern recognition helps identify the cause:
- Diffuse subendocardial LGE with difficulty nulling the myocardium = amyloidosis (amyloid fibrils trap gadolinium)
- Patchy mid-myocardial or epicardial LGE = sarcoidosis (granulomas scar the midwall)
- Absence of LGE in a thickened heart with low T1 signal = hemochromatosis (iron quenches signal)
- T1 mapping — elevated native T1 values indicate fibrosis or amyloid infiltration; reduced T1 values indicate iron deposition (hemochromatosis). Extracellular volume (ECV) fraction from T1 mapping quantifies interstitial expansion — ECV above 40% is strongly suggestive of amyloidosis.
- T2 mapping — elevated T2 indicates active myocardial inflammation (sarcoidosis, myocarditis). Useful for guiding biopsy timing and monitoring treatment response in sarcoidosis.
Nuclear Imaging (Bone Scintigraphy)
Technetium pyrophosphate (Tc-99m PYP) or DPD bone scintigraphy has become an important non-invasive test for ATTR amyloidosis specifically. In ATTR amyloidosis, bone tracers bind avidly to transthyretin amyloid deposits in the myocardium, producing a characteristic cardiac uptake pattern. A grade 2 or 3 cardiac signal with absent blood-pool activity in the absence of monoclonal protein (confirmed by serum/urine protein electrophoresis and free light chain assay) is diagnostic for ATTR amyloidosis without need for biopsy. This test does not reliably detect AL amyloidosis.
Cardiac Catheterization
When non-invasive testing is inconclusive — particularly to distinguish RCM from constrictive pericarditis — cardiac catheterization with simultaneous left- and right-heart pressure measurements is definitive:
- Equalization of diastolic pressures — right atrial pressure, right ventricular diastolic pressure, pulmonary capillary wedge pressure, and left ventricular end-diastolic pressure are all within 5 mmHg of each other (all elevated, typically 15–30 mmHg). This "equalization" pattern is present in both RCM and constrictive pericarditis.
- Square root sign — the dip-and-plateau pattern in the ventricular diastolic pressure tracing, reflecting rapid early filling followed by an abrupt halt.
- Preserved LVEF — normal or near-normal systolic function on left ventriculography.
- Respirophasic dissociation (key differentiator) — in constrictive pericarditis, left and right ventricular pressures move in opposite directions with respiration (ventricular interdependence); in RCM, they move together or show no significant variation (myocardial stiffness is the cause, not pericardial constraint).
Endomyocardial Biopsy
When non-invasive tests have not established a specific cause — especially if the distinction between AL and ATTR amyloidosis is needed, or if sarcoidosis is suspected but nuclear and MRI findings are non-diagnostic — endomyocardial biopsy may be performed. Biopsy samples show Congo-red staining (amyloid), non-caseating granulomas (sarcoidosis), or iron deposition (hemochromatosis). In AL amyloidosis, a less invasive fat pad biopsy or bone marrow biopsy may also demonstrate amyloid.
Distinguishing RCM from Constrictive Pericarditis
This is one of the most important clinical distinctions in cardiology — and one of the most difficult. Both conditions cause elevated and equalized filling pressures, signs of venous congestion, and similar symptoms. But the treatments are completely different: RCM is managed medically (and ultimately with transplantation); constrictive pericarditis is cured surgically by removing the pericardium (pericardiectomy). Missing the diagnosis of constrictive pericarditis means a potentially curable patient receives no effective treatment.
Key Distinguishing Features
- CT scan / MRI of the pericardium — pericardial thickening (greater than 3–4 mm) strongly suggests constrictive pericarditis. A normal pericardium on CT/MRI points toward RCM. Pericardial calcification on CT or plain film is pathognomonic of constrictive pericarditis (though it can be absent in early constrictive disease).
- Tissue Doppler annular velocity (e') — the single most useful echocardiographic differentiator: e' greater than 8–10 cm/s = constrictive pericarditis (the myocardium itself is normal and contracts vigorously, producing high annular velocity — the constrained filling is external); e' less than 8 cm/s = RCM (the myocardium is stiff and diseased, producing low annular velocity regardless of external constraint).
- Respirophasic variation in Doppler flows — in constrictive pericarditis, inspiration causes a greater than 25% reduction in mitral E-wave velocity (because the fixed pericardium means inspiratory filling of the right heart comes at the direct expense of the left heart). In RCM, there is minimal respirophasic variation — both ventricles are equally stiff and there is less ventricular interdependence. This test is highly sensitive and specific when performed correctly.
- Kussmaul's sign — present in both RCM and constrictive pericarditis; helps separate both from cardiac tamponade (where it is absent).
- BNP/NT-proBNP — markedly elevated in RCM (the stiff, stressed myocardium releases high levels of natriuretic peptides); moderately elevated in constrictive pericarditis (the myocardium is normal). A dramatically high BNP with no obvious reason favors RCM.
- Right heart catheterization respirophasic pressures — the gold standard when non-invasive tests are inconclusive: simultaneous LV and RV pressure measurement during respiration. In constrictive pericarditis, inspiration increases RV systolic pressure while simultaneously decreasing LV systolic pressure (discordant). In RCM, LV and RV systolic pressures move in the same direction with respiration (concordant) because the myocardium is the limiting factor, not the pericardium.
Why This Matters for Patients
Patients with constrictive pericarditis who are correctly diagnosed and undergo successful pericardiectomy can return to near-normal hemodynamics — often a dramatic, life-changing improvement. Patients with RCM who receive this surgery gain nothing (there is no rigid pericardium to remove) and face surgical risk for no benefit. The evaluation may require multiple tests and occasionally an expert center consultation before the distinction is certain.
Treatment by Cause
There is no single treatment for RCM — the approach is almost entirely determined by what is causing the stiffness. In some cases a specific therapy exists; in many, treatment is supportive. The underlying message for patients: knowing your diagnosis precisely is not just an academic exercise — it changes what doctors can offer.
Symptom Management (All Causes)
- Diuretics — the cornerstone of symptomatic relief. Careful use of loop diuretics (furosemide, torsemide) reduces congestion (pulmonary edema, leg swelling, ascites). However, in RCM the stiff ventricle depends critically on high filling pressures to generate any stroke volume — too aggressive diuresis causes the cardiac output to fall and the patient to feel worse. The therapeutic window is narrow: relieving congestion without emptying the tank.
- Heart rate control — the stiff ventricle benefits from a slower heart rate, which allows more time for filling in each cardiac cycle. Beta-blockers or non-dihydropyridine calcium channel blockers (verapamil, diltiazem) are used cautiously. However, beta-blockers can worsen RCM in some patients (especially amyloidosis) and must be used carefully.
- ACE inhibitors / ARBs — may help reduce filling pressures but must be used carefully because these agents lower preload and can cause symptomatic hypotension in the fixed-output state of RCM.
- Anticoagulation — strongly indicated in patients with atrial fibrillation (high stroke risk) and should be considered in sinus rhythm if there is significant atrial enlargement and documented sluggish flow. The choice of agent (warfarin vs. NOAC) depends on the underlying cause — in amyloidosis, some NOACs are preferred; in valvular disease, warfarin is needed.
Disease-Specific Treatments
- ATTR amyloidosis — Tafamidis: A transthyretin stabilizer that prevents the TTR protein from misfolding and forming amyloid fibrils. Approved by the FDA in 2019 for both wild-type and hereditary ATTR amyloid cardiomyopathy. The ATTR-ACT trial demonstrated a significant reduction in all-cause mortality and cardiovascular hospitalization with tafamidis 80 mg daily. This was a watershed moment — the first approved disease-modifying therapy for any form of cardiac amyloidosis. Earlier treatment (before advanced cardiac dysfunction) produces better outcomes.
- AL amyloidosis: The priority is treating the underlying plasma cell dyscrasia (analogous to treating the factory making the bad protein). Modern regimens include daratumumab (anti-CD38 monoclonal antibody) combined with bortezomib (a proteasome inhibitor) and dexamethasone. Achieving a deep hematologic response (very low circulating light chains) allows the cardiac amyloid burden to stabilize or slowly regress. Autologous stem cell transplant is an option in carefully selected patients with limited cardiac involvement. Cardiac transplantation alone is insufficient in AL amyloidosis because light chains from the bone marrow will re-infiltrate the new heart.
- Hemochromatosis: Regular therapeutic phlebotomy (blood removal) to deplete iron stores is effective — if started before significant myocardial fibrosis has developed, it can partially reverse the cardiomyopathy and prevent progression. For patients who cannot tolerate phlebotomy (severe anemia), iron chelation therapy with deferoxamine (IV or SC) or deferasirox (oral) removes excess iron. This is one of the most satisfying causes of RCM to diagnose because early treatment genuinely changes the outcome.
- Cardiac sarcoidosis: Immunosuppression with corticosteroids (prednisone 40–60 mg/day, tapering over months to 5–10 mg/day maintenance) is standard first-line therapy. It can reduce granulomatous inflammation, improve conduction disease, and stabilize ventricular function. Steroid-sparing agents (methotrexate, azathioprine, hydroxychloroquine) are used for long-term maintenance. Conduction disease (complete heart block, Wenckebach) and ventricular arrhythmias require pacemaker or ICD implantation — sarcoidosis is one of the leading causes of sudden cardiac death in young adults with cardiomyopathy in many countries.
- Fabry disease: Enzyme replacement therapy — agalsidase alfa (Replagal) or agalsidase beta (Fabrazyme), infused intravenously every two weeks — can stabilize or slow cardiac disease progression. The oral pharmacological chaperone migalastat is approved for patients with amenable GLA mutations (approximately 35–50% of the known mutation spectrum). Treatment is most effective when started before significant fibrosis has developed (detected by cardiac MRI).
- Endomyocardial fibrosis: Medical therapy is of limited benefit in advanced EMF. Surgical endocardiectomy (surgical removal of the fibrotic endocardium with valve repair or replacement) is the definitive treatment for advanced disease, improving symptoms and functional class in selected patients. In hypereosinophilic syndrome or Löffler's, treating the eosinophilia aggressively (corticosteroids, hydroxyurea, imatinib for FIP1L1-PDGFRA rearrangement) in the acute/inflammatory phase can prevent progression to fibrosis.
Device Therapy
- Pacemaker — indicated for high-degree heart block or sinus node dysfunction (common in sarcoidosis, amyloidosis, hemochromatosis).
- ICD (implantable cardioverter-defibrillator) — for ventricular arrhythmia risk, particularly in cardiac sarcoidosis and amyloidosis with reduced EF. Decision-making is complex because RCM patients often have very limited cardiac reserve, and multiple shocks can be poorly tolerated.
Heart Transplantation
Cardiac transplantation is the definitive treatment for end-stage RCM that does not respond to medical therapy. Outcomes are generally good in idiopathic RCM and hemochromatosis. Special considerations apply:
- AL amyloidosis: Heart transplant alone is insufficient — the light chains will re-infiltrate the transplanted heart. Patients require a combined heart transplant followed by autologous stem cell transplant to eliminate the plasma cell clone. Only highly selected patients (younger, preserved performance status, limited organ damage) are candidates.
- Hereditary ATTR amyloidosis: Combined heart-liver transplant can be considered in selected patients with the Val122Ile or Val30Met mutations — the liver produces the mutant transthyretin, so replacing both the heart and the liver removes both the damaged organ and the source of the toxic protein.
- Cardiac sarcoidosis and idiopathic RCM: Standard heart transplantation offers good outcomes; sarcoidosis may recur in the transplanted heart but this is usually manageable.
Prognosis and Long-Term Outlook
The prognosis of RCM depends more on its cause than on anything else. The range is wide — from near-normal survival with early-treated hemochromatosis to median survival measured in months with untreated AL amyloidosis. Most causes, once symptoms are established, carry a worse prognosis than dilated or hypertrophic cardiomyopathy.
Prognosis by Cause
- Idiopathic RCM: Poor. Five-year survival is approximately 30–50% in adults. Children with idiopathic RCM have an even worse prognosis without transplantation — it is the most common indication for pediatric heart transplant in some series. Predictors of worse outcome include older age, syncope, elevated filling pressures, and right ventricular dysfunction.
- AL amyloidosis: Historically the worst — median survival was 1–2 years after cardiac involvement was recognized, with many patients dying within 6 months of presentation in advanced disease. Modern plasma cell-directed therapy (daratumumab-bortezomib-dexamethasone) has substantially improved outcomes: patients who achieve a very good partial response or better have much longer survival. However, patients presenting with severe biventricular dysfunction (low voltage on ECG, very low EF, elevated troponin) have poor short-term prognosis even with treatment.
- ATTR amyloidosis: Better than AL, particularly wild-type ATTR (which typically presents in men over age 65 and progresses slowly). Tafamidis has changed the natural history — in the ATTR-ACT trial, all-cause mortality was significantly reduced over 30 months. Median survival in untreated ATTR cardiomyopathy was previously 2–6 years; with tafamidis, this has improved substantially.
- Cardiac sarcoidosis: Highly variable. Patients with isolated cardiac involvement and preserved EF can have years of stability on immunosuppression. Those presenting with advanced LV dysfunction, ventricular tachycardia, or complete heart block have a significantly higher risk of sudden cardiac death — ICD implantation is an important part of management.
- Hemochromatosis: Excellent if diagnosed and treated early. Phlebotomy prevents disease progression and can partially reverse established cardiomyopathy. Untreated patients with severe iron overload and established fibrosis have much worse outcomes, similar to idiopathic DCM.
- Endomyocardial fibrosis: Poor in advanced stages. Surgical endocardiectomy provides symptomatic improvement but the fibrotic process tends to recur. Five-year survival after surgery is approximately 60–70% in experienced centers.
- Fabry disease: With enzyme replacement therapy started early, cardiac disease can be stabilized. Without treatment, progressive hypertrophy, fibrosis, arrhythmias, and heart failure occur in the fourth to sixth decades in hemizygous males. Female carriers have more variable but often significant cardiac involvement.
General Prognostic Indicators
Across all causes, the following features indicate worse prognosis in RCM: right ventricular dysfunction and failure (a key determinant of transplant listing urgency), severe tricuspid regurgitation, very high filling pressures (LVEDP greater than 25 mmHg), severely elevated BNP/NT-proBNP, renal dysfunction (cardiorenal syndrome), atrial fibrillation with poor rate control, recurrent heart failure hospitalizations, low blood pressure or dependence on inotropic support. The development of restrictive physiology in any cardiomyopathy is a marker of advanced disease and portends a poor prognosis without escalation of therapy or consideration of transplantation.
Research Papers
The following citations are from published peer-reviewed literature on restrictive cardiomyopathy, its causes, diagnosis, and treatment.
- Search PubMed (Restrictive cardiomyopathy — landmark NEJM review covering pathophysiology, causes, diagnosis, and management)
- Habib G et al., 2014 — PMID: 25173340 (ESC cardiomyopathy guidelines: classification, diagnosis and management across all cardiomyopathy phenotypes)
- Search PubMed (ESC 2023 cardiomyopathy classification — updated framework including genetic and phenotypic refinements)
- Search PubMed (Restrictive cardiomyopathy — AHA scientific statement on epidemiology, pathophysiology and clinical management)
- Search PubMed (Tafamidis for transthyretin amyloid cardiomyopathy — ATTR-ACT trial; tafamidis reduced all-cause mortality and cardiovascular hospitalization)
- Search PubMed (Echocardiographic differentiation of RCM from constrictive pericarditis — tissue Doppler and respirophasic Doppler criteria)
- Search PubMed (Echocardiographic assessment of restrictive cardiomyopathy: key Doppler parameters and filling patterns)
- Search PubMed (Fabry disease cardiomyopathy: natural history, diagnosis, and response to enzyme replacement therapy)
- Search PubMed (Cardiomyopathy of iron overload — hemochromatosis cardiac manifestations, diagnosis, and treatment response)
- Search PubMed (Cardiac sarcoidosis: long-term outcomes and predictors of sudden cardiac death in a large single-center cohort)
- Search PubMed (Idiopathic restrictive cardiomyopathy: long-term outcomes and predictors of survival, transplant-free survival, and sudden death)
- Search PubMed (Incidence and predictors of implantable cardioverter-defibrillator therapy in cardiac sarcoidosis)
PubMed Topic Searches
- Restrictive cardiomyopathy diagnosis and treatment
- ATTR amyloidosis cardiomyopathy tafamidis
- Restrictive cardiomyopathy vs constrictive pericarditis differentiation
- Cardiac sarcoidosis sudden death ICD
- Endomyocardial fibrosis treatment outcomes
Connections
- Cardiology
- Cardiomyopathy (Overview)
- Dilated Cardiomyopathy
- Hypertrophic Cardiomyopathy
- Cardiac Amyloidosis
- Cardiac Sarcoidosis
- Constrictive Pericarditis
- Heart Failure
- HFpEF
- Atrial Fibrillation
- Heart Block
- Ventricular Tachycardia
- Cardiovascular Disease
- Pericarditis — inflammation of the pericardium; its constrictive form is the key mimic RCM must be told apart from.