Constrictive Pericarditis
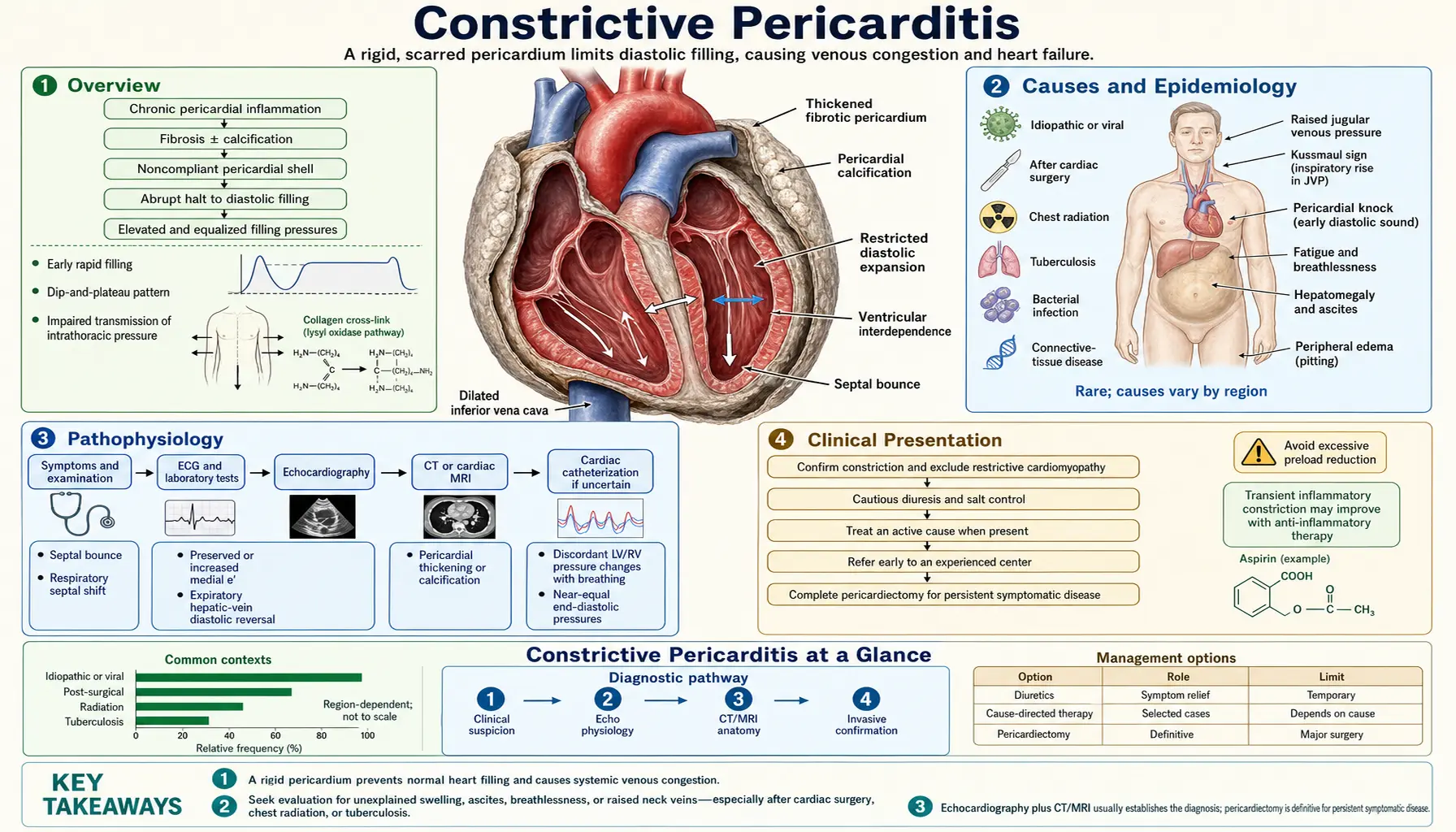
Table of Contents
- Overview
- Causes and Epidemiology
- Pathophysiology
- Clinical Presentation
- Hemodynamics
- Diagnosis
- Differentiation from Restrictive Cardiomyopathy
- Treatment
- Radiation-Associated Constrictive Pericarditis
- Prognosis
- Research Papers
- Connections
- Featured Videos
1. Overview
Constrictive pericarditis (CP) is a chronic condition in which the pericardium — the fibrous sac surrounding the heart — becomes thickened, fibrotic, and often calcified, losing its normal compliance and imposing a rigid external constraint on all four cardiac chambers. Unlike cardiac tamponade, which causes compression through accumulated fluid, CP is a solid structural restriction: the pericardium itself has been replaced by an inelastic scar that physically prevents normal diastolic expansion of the ventricles.
The defining hemodynamic consequence is equal restriction of diastolic filling in all four chambers. Because the rigid pericardial shell limits total cardiac volume, ventricular filling pressures equilibrate — right atrial pressure, left atrial pressure, and both ventricular end-diastolic pressures converge to the same elevated value. This diastolic equalization is the hemodynamic fingerprint of CP and distinguishes it from most other cardiac conditions.
A critically important clinical point: CP is one of the few forms of heart failure that is potentially surgically curable. Pericardiectomy — surgical removal of the fibrotic pericardium — can restore normal cardiac filling and dramatically improve symptoms in the majority of patients. This makes accurate diagnosis and distinction from restrictive cardiomyopathy (which carries a very different prognosis and has no surgical cure) one of the highest-stakes differentials in clinical cardiology.
CP may present insidiously over months to years, often mimicking liver disease (from hepatic congestion and ascites) or nephrotic syndrome, leading to delayed diagnosis. Recognizing the clinical syndrome early — particularly the combination of right heart failure, Kussmaul's sign, a pericardial knock on auscultation, and a history of pericardial injury — is essential for timely referral to an experienced center.
2. Causes and Epidemiology
Constrictive pericarditis results from any process that triggers pericardial inflammation followed by fibrosis and scarring. The relative importance of individual etiologies varies markedly by geographic region and socioeconomic context.
Radiation Therapy
In the developed world, prior chest radiation therapy has become the most common identifiable cause of CP. Mediastinal radiation for breast cancer, Hodgkin lymphoma, and lung cancer delivers doses to the pericardium that trigger an initial radiation pericarditis, followed by fibrosis that evolves over a characteristically long latency period of 10–20 years after treatment. Radiation-associated CP is among the most severe forms — the pericardium is densely fibrotic and may be inseparably fused to the underlying myocardium and epicardium. The myocardium itself is frequently damaged by radiation (radiation cardiomyopathy, coronary artery disease), making surgical intervention substantially more complex and increasing operative risk.
Idiopathic and Post-Viral
In many patients in developed countries, no specific cause can be identified — these cases are classified as idiopathic. Many are presumed to represent sequelae of unrecognized or subclinical viral pericarditis (most commonly coxsackievirus B, echovirus, and adenovirus). Idiopathic CP often responds better to pericardiectomy than radiation-associated forms, with superior long-term outcomes.
Cardiac Surgery
Post-cardiac surgery CP — following coronary artery bypass grafting (CABG), valve repair or replacement, or other cardiac procedures — is an increasingly recognized cause. Post-pericardiotomy syndrome (an immune-mediated pericarditis occurring weeks to months after cardiac surgery) may evolve into CP. The incidence of CP after cardiac surgery is estimated at 0.2–0.3%, but given the large volume of cardiac operations performed annually, it constitutes a meaningful absolute number.
Tuberculosis
TB pericarditis remains the most common cause of CP globally, particularly in sub-Saharan Africa, Southeast Asia, and other regions with high TB prevalence. Tuberculous pericarditis follows a characteristic course: initial exudative pericarditis → organized effusive-constrictive phase → progressive pericardial fibrosis and calcification. Heavy pericardial calcification visible on chest X-ray or CT in the correct geographic and demographic context should prompt TB evaluation. Antituberculous therapy can prevent progression to CP if given early, but established CP requires pericardiectomy.
Other Causes
- Malignancy: direct pericardial invasion or metastasis (lung cancer, breast cancer, lymphoma, mesothelioma); may present as effusive-constrictive physiology
- Uremia: uremic pericarditis in chronic kidney disease (especially pre-dialysis or inadequately dialyzed patients) can lead to CP; dialysis has reduced but not eliminated this etiology
- Connective tissue diseases: systemic lupus erythematosus (SLE), rheumatoid arthritis, systemic sclerosis — pericardial inflammation as part of serositis
- Purulent (bacterial) pericarditis: Staphylococcus aureus, Streptococcus pneumoniae, and gram-negative organisms can cause acute purulent pericarditis that heals with dense fibrosis
- Fungal pericarditis: Histoplasma capsulatum, particularly in endemic regions
- Drug-induced: hydralazine, procainamide, isoniazid (drug-induced lupus mechanism)
Epidemiology: CP is uncommon, with an estimated prevalence of approximately 1 in 10,000 in general populations. It represents a small fraction of heart failure cases but is disproportionately important because it is surgically curable. CP affects men slightly more often than women. It can occur at any age; radiation-associated CP presents later (latency 10–20 years after treatment) and TB-associated CP tends to affect younger patients in endemic regions.
3. Pathophysiology
The fundamental pathophysiological derangement in constrictive pericarditis is loss of pericardial compliance. The normal pericardium is a relatively inelastic fibrous sac that passively accommodates cardiac motion without imposing significant constraint under normal filling volumes. In CP, progressive fibrosis and calcification eliminate this accommodation, converting the pericardium into a rigid shell that limits total cardiac volume.
Equal Restriction of All Four Chambers
Because the rigid pericardium constrains the total cardiac volume, the filling of one chamber can only occur at the expense of another. This fixed total volume constraint means that all four chambers share the same absolute filling limit — producing the characteristic diastolic pressure equalization: right atrial pressure = left atrial pressure = right ventricular end-diastolic pressure (RVEDP) = left ventricular end-diastolic pressure (LVEDP) = pulmonary artery diastolic pressure (PAD), all within 5 mmHg of each other. This equalization is pathognomonic and forms the basis for the diagnostic hemodynamic criterion at cardiac catheterization.
Ventricular Interdependence and Septal Bounce
A second key consequence of the rigid pericardial shell is exaggerated ventricular interdependence. Normally, inspiration increases right ventricular (RV) filling and slightly decreases left ventricular (LV) filling — the interventricular septum shifts slightly leftward with inspiration. In CP, the rigid pericardium amplifies this interdependence. Because the total cardiac volume cannot change, increased RV filling during inspiration must displace the interventricular septum sharply leftward, producing the characteristic septal bounce visible on echocardiography — an abnormal, exaggerated septal motion with respiration. This can also be visualized on M-mode echocardiography as abnormal posterior wall motion.
The respiratory variation in ventricular filling also accounts for the exaggerated variation in transvalvular Doppler flow velocities: mitral E velocity decreases by >25% with inspiration (as LV filling is impaired by rightward septal shift) and tricuspid E velocity increases with inspiration. This reciprocal respiratory variation >25% across the atrioventricular valves is a key echocardiographic criterion for CP.
Kussmaul's Sign — Mechanism and Contrast with Tamponade
Kussmaul's sign (jugular venous pressure rises or fails to fall with inspiration) is present in CP. Normally, inspiration increases venous return to the right heart and JVP falls as the RV accommodates the increased flow. In CP, the rigid pericardial shell cannot accommodate the increased RV volume during inspiration — the increased venous return is transmitted back to the jugular veins, causing JVP to rise or remain elevated. Kussmaul's sign is a physical examination hallmark of CP.
In cardiac tamponade, Kussmaul's sign is characteristically absent. Instead, tamponade presents with pulsus paradoxus — an exaggerated fall in systolic blood pressure (>10 mmHg) with inspiration, caused by increased RV filling during inspiration shifting the septum leftward and reducing LV stroke volume. Tamponade also features muffled heart sounds, elevated JVP, and hypotension (Beck's triad). The distinction between tamponade (fluid = compressible, pulsus paradoxus present, urgent pericardiocentesis) and CP (solid fibrosis = rigid shell, Kussmaul's sign present, surgical pericardiectomy) is fundamental.
Transient (Inflammatory) vs. Permanent (Fibrotic) CP
An important clinical distinction: early in the evolution of pericardial disease — particularly post-viral or post-surgical pericarditis — an effusive-constrictive or transient constrictive physiology may develop during the active inflammatory phase. This early constriction is mediated by pericardial inflammation and edema rather than permanent fibrosis. In this phase, anti-inflammatory therapy (NSAIDs + colchicine ± corticosteroids) can resolve the constriction over weeks to months without surgery. Identifying the transient, inflammatory phase is critical — these patients should receive a trial of anti-inflammatory therapy before surgical referral. Gadolinium enhancement of the pericardium on cardiac MRI (suggesting active inflammation rather than inert fibrosis) is the key imaging discriminator.
4. Clinical Presentation
The clinical presentation of constrictive pericarditis is dominated by the consequences of chronically elevated venous pressures — primarily right heart failure — in a patient who may have surprisingly preserved biventricular systolic function. The insidious, slowly progressive course frequently leads to diagnostic delay, with patients sometimes labeled as having idiopathic liver disease, nephrotic syndrome, or cryptogenic ascites before CP is identified.
Symptoms
- Dyspnea: initially exertional, progressing to rest; results from elevated left atrial pressure and pulmonary venous congestion; may be less prominent than in other causes of heart failure if right heart failure dominates
- Peripheral edema: often severe, extending above the ankles to involve the thighs and abdomen; a hallmark of chronically elevated right-sided pressures
- Ascites: may be massive, often disproportionate to the degree of peripheral edema; hepatic venous congestion causes transudative ascites that mimics cirrhosis; frequently the presenting complaint
- Fatigue and exercise intolerance: fixed cardiac output (cannot augment filling with exertion due to rigid pericardium) produces a low, fixed cardiac output state; exertional fatigue may be the earliest symptom
- Abdominal discomfort: from hepatomegaly, ascites, and mesenteric venous congestion; may produce early satiety and anorexia
- Cachexia: in advanced, long-standing CP; a protein-losing enteropathy from mesenteric venous congestion can exacerbate nutritional depletion
Signs
- Elevated jugular venous pressure (JVP): universally present in established CP; prominent Y descent (rapid early diastolic ventricular filling) is characteristic; Kussmaul's sign (JVP rises or fails to fall with inspiration) is highly specific for CP
- Pericardial knock: a high-pitched, early diastolic sound occurring shortly after S2, heard best at the left sternal border or apex; represents the abrupt cessation of ventricular filling when the rigid pericardium halts diastolic expansion; earlier than the S3 gallop of heart failure and higher in pitch; a pathognomonic physical finding when present
- Hepatomegaly: congestive hepatomegaly; may be pulsatile; hepatic veins are engorged; in chronic CP, hepatic fibrosis (cardiac cirrhosis) may develop, further complicating the clinical picture
- Ascites: typically non-tense unless very advanced; protein-rich transudative fluid from hepatic congestion
- Peripheral edema: bilateral, pitting, often extending to the thighs
- Absent pulsus paradoxus: in contrast to tamponade, pulsus paradoxus is typically absent or mild in CP; this distinction has significant diagnostic value at the bedside
Contrast with Cardiac Tamponade
The bedside distinction between CP and tamponade is of immediate clinical importance, since tamponade requires urgent pericardiocentesis while CP requires planned pericardiectomy. Key differentiators:
- Tamponade: pulsus paradoxus (>10 mmHg fall in SBP with inspiration) present; Kussmaul's sign absent; Beck's triad (hypotension, elevated JVP, muffled heart sounds); acute-subacute onset
- CP: pulsus paradoxus absent or minimal; Kussmaul's sign present; pericardial knock; chronic insidious course; normal or near-normal blood pressure until late
5. Hemodynamics
Cardiac catheterization provides the definitive hemodynamic characterization of constrictive pericarditis. While echocardiography and cardiac MRI can strongly suggest the diagnosis non-invasively, right heart catheterization — and often simultaneous right and left heart catheterization — remains the gold standard for confirming constrictive physiology and differentiating CP from restrictive cardiomyopathy.
The Square Root Sign (Dip-and-Plateau)
The most characteristic hemodynamic waveform in CP is the square root sign on ventricular pressure tracings. During diastole, ventricular pressure demonstrates:
- Rapid early diastolic pressure drop: as the atrioventricular valve opens, blood rushes rapidly into the ventricle (the "dip") — early diastolic filling is actually accelerated in CP because of the steep atrio-ventricular pressure gradient built up by elevated atrial pressures
- Abrupt mid-diastolic plateau: filling abruptly halts when the expanding ventricle meets the rigid pericardial wall (the "plateau") — no further filling occurs through mid and late diastole
On the ventricular pressure trace, this creates a waveform resembling a square root symbol (√), also called the "dip-and-plateau" pattern. On the atrial pressure tracing, the rapid early diastolic filling is reflected as a prominent, steep Y descent (rapid fall in atrial pressure as blood empties into the ventricle during early diastole).
Diastolic Pressure Equalization
The pathognomonic hemodynamic finding in CP is equalization of all diastolic filling pressures within 5 mmHg:
- Right atrial mean pressure = Left atrial mean pressure (or PCWP)
- RVEDP = LVEDP
- Pulmonary artery diastolic pressure = LVEDP
- Typical values: all pressures equalized at 15–25 mmHg
- The LVEDP − RVEDP difference is <5 mmHg (often <2 mmHg)
Respiratory Discordance of RV and LV Pressures
A critical differentiating hemodynamic feature between CP and restrictive cardiomyopathy (RCM) is the respiratory behavior of simultaneous RV and LV systolic pressures. In CP, the fixed total pericardial volume means that as inspiration increases RV filling and RV systolic pressure rises, LV filling simultaneously decreases and LV systolic pressure falls — the two ventricular pressure peaks move in opposite directions with respiration (discordance). In RCM, both pressures rise and fall together with respiration (concordance), because there is no fixed external constraint. This RV-LV pressure discordance on respiratory variation, measured on simultaneous high-fidelity pressure tracings during right and left heart catheterization, is the most definitive invasive test for distinguishing CP from RCM when the diagnosis remains uncertain after non-invasive testing.
Pulmonary Artery Pressure
Pulmonary artery systolic pressure in CP is typically modestly elevated (30–45 mmHg), reflecting the chronically elevated left atrial pressure. Severely elevated pulmonary hypertension (>60 mmHg) is unusual in CP and should prompt consideration of an alternative or concurrent diagnosis. By contrast, in severe RCM, pulmonary hypertension may be more prominent. The relatively modest pulmonary hypertension in CP (proportionate to the elevated PCWP) is consistent with passive pulmonary venous hypertension rather than reactive pulmonary arterial disease.
6. Diagnosis
The diagnosis of CP integrates clinical history, physical examination, imaging, and hemodynamics. No single test is definitively diagnostic in isolation; the diagnosis rests on the convergence of multiple supportive findings.
Chest X-Ray
Pericardial calcification on plain chest X-ray — appearing as a curvilinear opacity following the cardiac contour, best seen on the lateral view — is highly specific for CP when present. However, it is absent in many cases (particularly idiopathic and post-surgical CP) and its absence does not exclude the diagnosis. Pleural effusions and signs of pulmonary venous congestion may also be present.
CT of the Chest
CT is the most sensitive imaging modality for detecting pericardial calcification and thickening. Key CT findings in CP:
- Pericardial calcification: ≥3 mm of calcification is highly specific for CP; typically involves the AV groove and right ventricular free wall
- Pericardial thickening: >3–4 mm is abnormal; may be diffuse or focal; thickening without calcification is more common in early or non-calcific CP (post-surgical, post-viral)
- Dilated inferior vena cava and hepatic veins; bilateral pleural effusions; ascites — secondary signs of systemic venous hypertension
- Tubular, non-dilated ventricles with dilated atria — the "funnel-shaped" ventricular morphology from pericardial constriction
Cardiac MRI
Cardiac MRI (CMR) is the most informative non-invasive test for evaluating pericardial disease and myocardial structure. CMR findings in CP:
- Pericardial thickening: >3–4 mm is abnormal; best visualized on double-inversion recovery sequences
- Gadolinium enhancement of the pericardium: indicates active pericardial inflammation rather than inert fibrosis — this is the key finding that identifies transient constrictive pericarditis likely to respond to anti-inflammatory therapy, potentially avoiding surgery. Lack of enhancement suggests established fibrous or calcific CP requiring pericardiectomy.
- Myocardial tethering: adhesion between the pericardium and myocardium seen as restricted epicardial motion — implies pericardium is fused to the heart surface, complicating pericardiectomy
- Real-time cine MRI: can demonstrate septal bounce and abnormal septal motion with respiration
Echocardiography
Echocardiography is the first-line imaging modality and provides multiple complementary signs. No single echo finding is pathognomonic, but the combination is highly diagnostic:
- Septal bounce: abnormal leftward-then-rightward motion of the interventricular septum, most prominent in early diastole — one of the most specific echo signs of CP; represents exaggerated interventricular dependence
- M-mode posterior wall motion: flat or near-flat posterior wall motion in mid-late diastole (corresponds to the plateau phase of filling)
- Annulus reversus on tissue Doppler imaging (TDI): normally, medial mitral annulus velocity (e') exceeds lateral annular velocity due to the lateral wall's greater excursion. In CP, the medial annulus is constrained by the thickened pericardium at the AV groove, causing medial e' to be lower than lateral e' (lateral e' > medial e'), the reverse of normal — hence "annulus reversus." This finding is highly specific for CP and helps distinguish it from RCM (where both annular velocities are reduced).
- Respiratory variation in mitral E velocity >25%: mitral E velocity decreases ≥25% from expiration to inspiration (reflecting reduced LV filling during inspiration due to interventricular dependence); reciprocal increase in tricuspid E velocity during inspiration
- Hepatic vein Doppler: expiratory hepatic vein flow reversal (diastolic reversal augments on expiration, the reverse of normal) — contrast with restrictive cardiomyopathy where inspiratory reversal predominates
- Inferior vena cava dilation: dilated, non-collapsing IVC indicating chronically elevated right atrial pressure
- Preserved or near-normal LVEF: systolic function is typically preserved in CP; severely reduced EF should prompt reconsideration or evaluation for concurrent myocardial disease
Right Heart Catheterization
When non-invasive testing is inconclusive or when differentiation from RCM is critical, right heart catheterization (with simultaneous left heart catheterization if needed) provides definitive hemodynamic characterization as detailed in the Hemodynamics section. Provocative testing (rapid saline infusion to unmask constrictive physiology that is not apparent at rest) may be required in early or partially treated CP where resting pressures are only mildly elevated.
7. Differentiation from Restrictive Cardiomyopathy
The differential diagnosis of CP versus restrictive cardiomyopathy (RCM) is one of the most clinically important distinctions in cardiology. Both conditions present with diastolic heart failure, elevated filling pressures, and diastolic pressure equalization on cardiac catheterization. The critical difference: CP is potentially surgically curable by pericardiectomy; RCM has no surgical cure and carries a worse prognosis. Misclassifying CP as RCM denies the patient a curative operation; misclassifying RCM as CP exposes the patient to high-risk surgery with no benefit.
Clinical and Imaging Features Favoring CP
- History of pericardial injury: prior chest radiation, cardiac surgery, TB, viral pericarditis
- Pericardial calcification on CT (highly specific)
- Pericardial thickening >3–4 mm on CT or CMR
- Septal bounce on echocardiography
- Annulus reversus on TDI (lateral e' > medial e')
- Respiratory variation >25% in mitral E velocity
- Expiratory hepatic vein flow reversal
- Gadolinium pericardial enhancement on CMR (transient inflammatory CP)
- No evidence of myocardial disease
Clinical and Imaging Features Favoring RCM
- Evidence of infiltrative or storage myocardial disease: amyloidosis (birefringent Congo red staining, "sparkling" myocardium on echo, global subendocardial LGE on CMR, bone scintigraphy positive for ATTR), hemochromatosis, Fabry disease, glycogen storage disease, sarcoidosis
- Normal pericardial thickness on CT/CMR
- No septal bounce
- Annulus normalis or reduced (both medial and lateral e' reduced — annulus paradoxus pattern in amyloid)
- No respiratory variation in mitral E velocity (or inspiratory augmentation of hepatic vein reversal)
- Prominent biatrial enlargement
- Elevated NT-proBNP (markedly elevated in most RCM, may be less striking in pure CP)
Hemodynamic Differentiation at Catheterization
When imaging is inconclusive, simultaneous high-fidelity RV and LV pressure recording during catheterization provides the most definitive differentiation:
- CP: RV-LV systolic pressure discordance with respiration (RV systolic pressure increases during inspiration while LV systolic pressure decreases); RV-LV area index (ratio of RV to LV stroke work changes with respiration) >1.1 suggests CP
- RCM: RV-LV systolic pressure concordance with respiration (both rise and fall together)
- Both CP and RCM: LVEDP − RVEDP <5 mmHg at rest; in RCM, the gradient may widen with volume challenge; in CP it remains equalized
Role of Cardiac MRI
CMR is the most useful single non-invasive test for differentiating CP from RCM. Pericardial thickening, myocardial tethering, and gadolinium pericardial enhancement all favor CP. The LGE pattern in RCM is characteristically myocardial (global subendocardial in amyloid, patchy mid-wall in sarcoid or other infiltrative diseases) rather than pericardial. CMR also characterizes myocardial tissue properties (T1 mapping for amyloid, T2 mapping for edema, ECV for fibrosis quantification) that may establish the cause of RCM.
8. Treatment
Treatment of CP is fundamentally divided based on whether the constriction is transient (inflammatory, potentially reversible) or permanent (established fibrosis/calcification, requiring surgery).
Transient Constrictive Pericarditis — Anti-Inflammatory Trial
In patients with recent-onset CP (weeks to a few months post-viral pericarditis, post-cardiac surgery, or post-pericardiocentesis) where gadolinium enhancement of the pericardium on CMR suggests active inflammation, a structured anti-inflammatory trial of 3 months should be attempted before surgical referral:
- NSAIDs: ibuprofen 400–600 mg three times daily, or indomethacin 25–50 mg three times daily; weight-based dosing with proton pump inhibitor gastroprotection; continued for 3 months with gradual taper
- Colchicine 0.5 mg twice daily (once daily if weight <70 kg or intolerant): added to NSAID therapy; reduces inflammatory recurrence; continued for 3 months; contraindicated in severe renal or hepatic impairment
- Prednisolone 0.2–0.5 mg/kg/day: added for patients who fail NSAID + colchicine alone, or for patients where NSAIDs are contraindicated; corticosteroids are effective but associated with higher recurrence rates than NSAID + colchicine alone, and long-term steroid use should be minimized
- Reassess at 3 months with clinical evaluation, echocardiography, and CMR; complete resolution is the goal — surgery is averted in a significant proportion of patients with transient CP
Permanent Constrictive Pericarditis — Pericardiectomy
Pericardiectomy (surgical decortication — removal of the fibrotic/calcified pericardium) is the definitive and standard treatment for established CP that has failed or is not a candidate for anti-inflammatory therapy.
- Extent of resection: complete pericardiectomy via median sternotomy, resecting pericardium from the diaphragm to the great vessels; more complete resection is associated with better outcomes; incomplete decortication is a major cause of suboptimal results and persistent symptoms
- Outcomes: at experienced centers, 75–90% of patients experience significant symptomatic improvement following complete pericardiectomy; NYHA functional class improvement of 1–2 classes is typical; most patients return to near-normal activity
- Operative mortality: 5–10% at experienced surgical centers for non-radiation-associated CP; higher mortality for radiation-associated CP (10–20%) due to underlying myocardial and vascular disease
- Time to benefit: hemodynamic improvement may be immediate but full functional recovery takes months — the chronically congested myocardium requires time to remodel and recover; normalization of filling pressures precedes normalization of cardiac output and exercise capacity
- Timing: pericardiectomy should not be delayed in patients with established CP and functional limitation; progressive hepatic congestion, ascites, and protein-losing enteropathy worsen perioperative outcomes if surgery is unduly postponed
- Cardiopulmonary bypass: required in approximately 25–50% of pericardiectomies (dense epicardial adhesions, calcification penetrating into myocardium, need for concomitant procedures); bypass increases operative risk but is sometimes unavoidable
Medical Management (Palliative or Bridge)
Medical therapy does not change the natural history of established CP but provides symptom relief:
- Diuretics: loop diuretics (furosemide, bumetanide) ± aldosterone antagonists (spironolactone) for volume overload, edema, and ascites; use cautiously — over-diuresis reduces ventricular preload and may severely decrease cardiac output in the already preload-dependent constrictive physiology
- Heart rate control: CP patients depend on heart rate to maintain cardiac output (stroke volume is fixed); excessive bradycardia from rate-limiting agents (beta-blockers, calcium channel blockers) can precipitate hemodynamic compromise — use these agents with caution
- Salt restriction and fluid management
- Medical therapy alone is not curative and is reserved for patients who are not surgical candidates (extremely high operative risk, end-stage radiation-associated CP with refractory myocardial damage)
9. Radiation-Associated Constrictive Pericarditis
Radiation-associated CP deserves special emphasis as the most severe and surgically challenging form of the disease. As cancer survival improves — particularly for breast cancer, Hodgkin lymphoma, and lung cancer — the long-term cardiac complications of mediastinal and thoracic radiation therapy are becoming increasingly prevalent.
Pathogenesis and Latency
Ionizing radiation damages vascular endothelium, myocardial cells, and pericardial mesothelium through direct DNA damage, reactive oxygen species generation, and downstream inflammatory cascades. Radiation pericarditis may be acute (occurring during or shortly after radiation, usually asymptomatic) or delayed. The characteristic latency for clinically significant constrictive pericarditis is 10–20 years after chest radiation, though cases have been reported as early as 5 years and as late as 30+ years post-treatment. The latency reflects the slow evolution of fibrosis over years following the initial radiation-induced injury.
Pathological Severity
Radiation-associated CP differs qualitatively from idiopathic or post-viral CP in pathological severity:
- The pericardium is densely fibrotic — often calcified and inseparably adherent to the myocardium and epicardium
- The myocardium itself is frequently damaged: radiation cardiomyopathy, with myocardial fibrosis, diastolic dysfunction, and occasionally systolic dysfunction coexist with the pericardial constriction, blurring the pure constrictive hemodynamic picture
- Radiation-induced coronary artery disease — premature atherosclerosis, particularly of the left anterior descending artery in left-sided chest radiation — may coexist and require simultaneous coronary revascularization at the time of pericardiectomy
- Valvular disease (radiation-induced fibrosis of the aortic and mitral valves) may also be present, further increasing surgical complexity
Surgical Outcomes
Pericardiectomy for radiation-associated CP carries substantially higher operative risk than for other etiologies:
- Operative mortality is approximately 10–20% at experienced centers, compared to 5–10% for idiopathic CP
- Long-term (5-year) survival after pericardiectomy for radiation-associated CP is approximately 50%, compared to 80–90% for idiopathic or post-surgical CP
- The inferior long-term outcomes reflect underlying radiation-induced myocardial damage that persists despite successful pericardial decortication — many patients have residual diastolic dysfunction from radiation cardiomyopathy even after the pericardial constraint is relieved
- Multidisciplinary preoperative planning is essential: cardiac surgery, oncology, radiation oncology, and cardiology collaboration; careful assessment of coronary artery disease (coronary CT angiography or cardiac catheterization), valvular disease, and myocardial function
- Patients who are surgical candidates should still be offered pericardiectomy, since medical therapy offers no alternative — but realistic counseling about the higher perioperative risk and limited long-term benefit compared to non-radiation CP is essential
Prevention
Modern radiation oncology techniques have dramatically reduced the cardiac dose delivered during cancer treatment. Intensity-modulated radiation therapy (IMRT), proton beam therapy, deep-inspiration breath-hold techniques (for left breast cancer), and cardiac-sparing radiation planning aim to minimize pericardial dose. These advances are expected to reduce the future incidence of radiation-associated CP, though the 10–20 year latency means that cases from older treatment regimens will continue to present for years to come.
10. Prognosis
The prognosis of constrictive pericarditis is highly dependent on etiology, timeliness of diagnosis, and access to surgical expertise.
Without Treatment
Untreated established CP follows a course of progressive right and eventually biventricular heart failure. Chronically elevated venous pressures lead to cardiac cirrhosis (hepatic fibrosis from persistent congestion), protein-losing enteropathy, nutritional depletion, renal venous congestion, and cachexia. Without pericardiectomy, median survival from the onset of significant symptoms is typically less than 5 years, with progressive functional decline dominating the clinical course.
After Pericardiectomy
Pericardiectomy dramatically improves outcomes for most patients with non-radiation CP:
- Idiopathic and post-viral CP: 5-year survival post-pericardiectomy approximately 80–90%; most patients achieve sustained symptomatic improvement; recurrence after complete pericardiectomy is uncommon (<5%)
- Post-surgical CP: similar to idiopathic outcomes; 5-year survival approximately 80%; slightly higher operative risk due to pericardial adhesions from prior surgery
- TB-associated CP: good outcomes when pericardiectomy is combined with completion of antituberculous therapy; outcomes comparable to idiopathic CP in most series
- Radiation-associated CP: substantially worse; 5-year survival approximately 50%; limited by underlying myocardial and vascular radiation damage
Predictors of Poor Outcomes After Pericardiectomy
- Radiation as the etiology — most important prognostic factor
- Preoperative NYHA Class IV (most advanced functional limitation)
- Reduced LVEF (suggests concurrent myocardial disease beyond pure pericardial constriction)
- Renal dysfunction (elevated creatinine predicts higher perioperative mortality)
- Hepatic dysfunction or established cardiac cirrhosis (impairs surgical recovery)
- Incomplete pericardiectomy (inadequate decortication is a major cause of persistent symptoms and reoperation)
- Need for cardiopulmonary bypass
- Older age
Recurrence
Recurrent CP after complete pericardiectomy is uncommon, occurring in fewer than 5% of cases. Incomplete resection, leaving residual pericardial tissue (particularly at the posterior left ventricle and great vessels), is the primary cause of persistent or recurrent constrictive physiology. When recurrence does occur, re-do pericardiectomy carries substantially higher risk than the initial operation due to pericardial and epicardial adhesions, and outcomes are more variable.
Transient CP
Patients with inflammatory (transient) CP who respond to anti-inflammatory therapy have an excellent prognosis. Complete resolution of constrictive physiology occurs in the majority, with no requirement for pericardiectomy. Long-term follow-up is warranted, as some patients may develop recurrent episodes or ultimately progress to permanent CP if anti-inflammatory therapy is inadequate.
11. Research Papers
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Cardiology
- Pericarditis
- Cardiac Tamponade
- Heart Failure
- Cardiomyopathy
- Myocarditis
- Cardiac Sarcoidosis
- HFpEF
- Cardiac Amyloidosis
- Pulmonary Hypertension
- Hypertrophic Cardiomyopathy
- Arrhythmia
- All Conditions