Cardiovascular Disease: History and Discovery
Cardiovascular disease is not one illness but an umbrella term for the many disorders of the heart and the blood vessels — coronary artery disease, stroke, hypertension, heart failure, valve disease, and the rest. Because it is a category rather than a single condition, it has no single inventor or discoverer. Its modern understanding was assembled, piece by piece, over four centuries: from William Harvey's demonstration that the blood circulates (De Motu Cordis, 1628), through the pathologists who first described diseased arteries, to the twentieth century when heart disease became the leading cause of death in the industrialized world and a landmark study in Framingham, Massachusetts (begun 1948) gave us the now-universal idea of cardiovascular "risk factors." What follows traces that cumulative arc — honestly noting where the science is settled and where the debates, such as the diet-heart question, remain genuinely open.
Table of Contents
- An Umbrella Term, Not a Single Disease
- Ancient Evidence: Heart Disease Is Not New
- William Harvey and the Circulation of the Blood
- The Pathologists: Naming the Diseased Artery
- Measuring the Cardiovascular System
- The Twentieth-Century Epidemic
- Framingham and the Birth of the "Risk Factor"
- Ancel Keys and the Diet-Heart Debate
- The Rise and Partial Fall of Cardiovascular Death
- Research Papers and References
- Connections
- Featured Videos
An Umbrella Term, Not a Single Disease
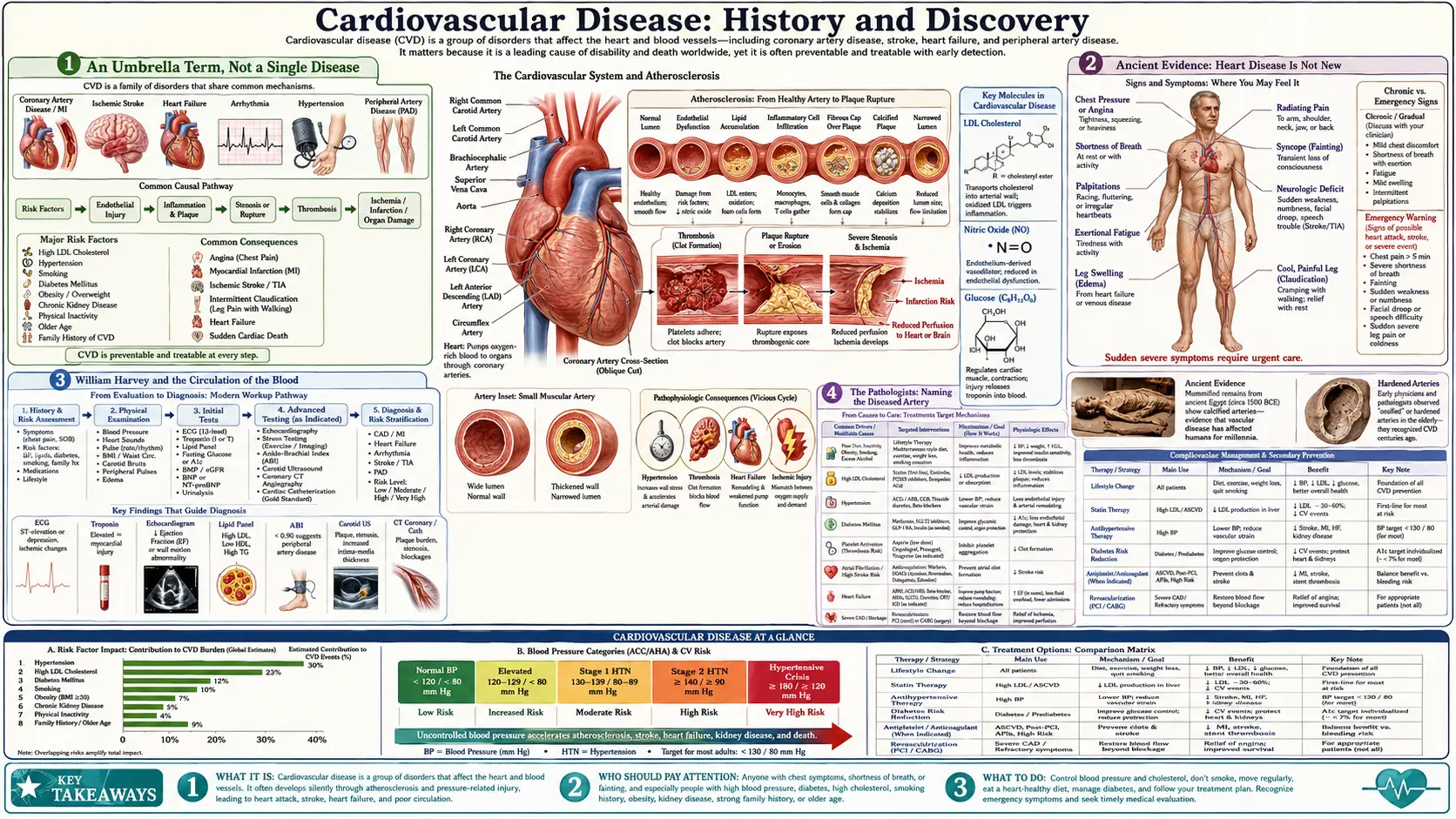
The phrase "cardiovascular disease" (CVD) covers every disorder of the heart (cardio-) and the blood vessels (-vascular). Under that one heading sit conditions as different as a sudden heart attack, a slowly failing heart muscle, a burst or blocked vessel in the brain (stroke), chronically high pressure in the arteries (hypertension), narrowed leg arteries, leaking or stiffened heart valves, and irregular heart rhythms. Because the term groups together many distinct diseases that share a common anatomy and often common underlying processes — chiefly atherosclerosis, the build-up of fatty, fibrous plaque inside artery walls — it is a classification, not a discovery with a date and a discoverer.
This matters for any honest history. There was no single moment when cardiovascular disease was "found," and no one person who can be credited with it. Instead, the story is one of accumulation: anatomists learned how the heart and vessels are built and how blood moves through them; pathologists learned what goes wrong inside a diseased artery; physicians learned to measure blood pressure and read the heart's electrical signals; and epidemiologists, in the twentieth century, learned who gets these diseases and why. Each layer was laid by different people in different centuries, and the umbrella term we now use is the sum of all of them. The sections that follow credit specific figures for specific, verifiable contributions — Harvey for circulation, Herrick for the clinical picture of a heart attack, Kannel and the Framingham team for the risk-factor concept — while resisting the temptation to crown any one of them the "discoverer of cardiovascular disease," a title that does not exist.
Ancient Evidence: Heart Disease Is Not New
It is tempting to think of cardiovascular disease as a purely modern affliction — a product of fast food, tobacco, and sedentary office life. The fossil and archaeological record says otherwise. The most striking evidence comes from ancient Egyptian mummies. In the Horus Study, an international team of cardiologists and Egyptologists used whole-body CT scanning to look for arterial calcification — a hallmark of atherosclerosis — in preserved bodies spanning the Middle Kingdom to the Greco-Roman period. Of 44 mummies with identifiable arteries, 20 showed definite or probable atherosclerosis, with calcified deposits in the aorta and in the coronary, carotid, iliac, femoral, and leg arteries.
The finding was not confined to Egypt. An expanded Horus analysis of 137 mummies from four widely separated ancient populations — ancient Egyptians, ancient Peruvians, the Ancestral Puebloans of the American Southwest, and the Unangan hunter-gatherers of the Aleutian Islands — found probable or definite atherosclerosis in 34% of them, and in all four populations. Because these peoples ate very different diets and lived very different lives (including pre-agricultural hunter-gatherers), the work suggests that atherosclerosis is, to some degree, an ancient and perhaps partly intrinsic feature of human ageing — not solely a creation of the modern world.
Written and physical records reinforce the picture. Ancient Egyptian medical papyri describe chest pain and a weak or fluttering pulse; classical Greek and Roman physicians wrote of sudden death and of dropsy (the old term for the body-wide swelling of heart failure). None of these observers understood the mechanism — that awaited Harvey and the pathologists — but the diseases themselves were plainly present. The honest lesson is twofold: cardiovascular disease has shadowed humanity for millennia, and its dramatic twentieth-century surge in industrialized nations shows that environment and behavior powerfully shape how common and how deadly it becomes.
William Harvey and the Circulation of the Blood
The single most important foundation for understanding cardiovascular disease is the realization that blood circulates — that the heart is a pump driving blood through a closed loop of vessels and back to itself. This was established by the English physician William Harvey (1578–1657) in his short Latin treatise Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus ("An Anatomical Exercise on the Motion of the Heart and Blood in Animals"), published in Frankfurt in 1628 and universally known as De Motu Cordis. Before Harvey, Western medicine still largely followed the second-century authority Galen, who taught that blood was continuously made in the liver, consumed by the tissues, and passed between the heart's chambers through invisible pores — with no circulation at all.
Harvey's achievement was as much about method as conclusion. He combined careful dissection, live-animal observation, and a now-famous piece of quantitative reasoning: he estimated the volume of blood the heart ejects with each beat and multiplied by the heart rate, showing that in a single hour the heart pumps far more blood than the body could possibly manufacture from food. The blood, therefore, had to be the same blood, used over and over — it must circulate. He demonstrated the one-way flow directly with a simple forearm experiment: a ligature that swelled the veins made their valves stand out, and he showed that venous blood could be pushed only toward the heart, never away, proving the valves enforce a single direction of flow.
Harvey could not see the tiny vessels linking arteries to veins; the capillaries were observed only later, by Marcello Malpighi in 1661 using the new microscope, completing the circuit Harvey had deduced. Even so, De Motu Cordis is rightly regarded as the founding document of cardiovascular physiology. Without the concept of circulation, none of the later understanding of cardiovascular disease — blocked coronary arteries starving the heart muscle, clots travelling to the brain, pressure building in a closed system — would have been possible. Harvey supplied the framework inside which every later discovery would make sense.
The Pathologists: Naming the Diseased Artery
If Harvey explained how a healthy cardiovascular system works, it fell to the pathologists of the eighteenth and nineteenth centuries to describe what a diseased one looks like. As anatomists began routinely opening the bodies of people who had died of chest pain, sudden collapse, or dropsy, they found arteries hardened, narrowed, and lined with yellowish, gritty, fatty deposits. The term atherosclerosis — from Greek athere (gruel or porridge, for the soft lipid core) and skleros (hard, for the fibrous cap) — came into use in the early twentieth century, generally credited to Felix Marchand around 1904, to capture exactly this combination of soft and hard within the artery wall.
The nineteenth century also produced a foundational debate about why arteries degenerate — one whose terms still echo in modern cardiology. The Austrian pathologist Carl von Rokitansky (1804–1878) proposed an "incrustation" theory, arguing that the plaque began with deposits derived from blood and clot (thrombus) on the vessel wall, with any inflammation a secondary response. His German contemporary Rudolf Virchow (1821–1902) argued instead that inflammation of the artery wall was the primary, initiating event, while also recognizing the lipid ("Cholesterin") accumulation within the lesions. For much of the twentieth century the field treated atherosclerosis mainly as passive cholesterol storage; remarkably, modern research has substantially vindicated Virchow's emphasis on inflammation, recognizing atherosclerosis as an active, chronic inflammatory process — while also confirming a genuine role for incorporated thrombus, as Rokitansky maintained. Both pathologists, it turns out, saw part of the truth.
The clinical counterpart arrived in 1912, when the Chicago physician James B. Herrick published "Clinical Features of Sudden Obstruction of the Coronary Arteries" in JAMA — the first influential clinical description of what we now call a heart attack, linking it to thrombosis (clotting) in a coronary artery. Crucially, Herrick argued that such an event was not inevitably fatal, a hopeful and, at the time, controversial idea. By his own account his 1912 paper "fell flat as a pancake" and was ignored until he revisited the subject, with electrocardiographic evidence, in 1918–1919. The diseased artery now had both a pathological description and a clinical face.
Measuring the Cardiovascular System
Understanding cardiovascular disease in living patients required tools to measure the system without opening the body. Two nineteenth- and early-twentieth-century inventions transformed cardiology from a discipline of autopsy into one of bedside diagnosis: the blood-pressure cuff and the electrocardiogram.
Reliable, non-invasive blood-pressure measurement arrived in stages. In 1896 the Italian physician Scipione Riva-Rocci introduced a practical mercury sphygmomanometer with an inflatable upper-arm cuff, allowing systolic pressure to be read from the point at which the pulse disappeared. In 1905 the Russian surgeon Nikolai Korotkoff added the auscultatory method — listening with a stethoscope over the artery for the now-famous "Korotkoff sounds" — which made it possible to read both the systolic and the diastolic pressure. The familiar two-number blood-pressure reading dates from this advance, and it is what eventually made hypertension measurable, trackable, and treatable rather than an invisible condition discovered only at autopsy.
The heart's electrical activity became readable through the Dutch physiologist Willem Einthoven, who built a practical string-galvanometer electrocardiograph in the first decade of the twentieth century and defined the P-QRS-T waves still used today; he won the 1924 Nobel Prize in Physiology or Medicine for it. The ECG let physicians detect heart attacks, rhythm disturbances, and cardiac strain from the body surface. Later, cardiac catheterization — pioneered in part by Werner Forssmann, who in 1929 famously threaded a catheter into his own heart — opened the way to coronary angiography and, ultimately, angioplasty and stenting. Together these tools turned cardiovascular disease into something a doctor could see, quantify, and follow over time — the essential precondition for the great epidemiological studies that followed.
The Twentieth-Century Epidemic
One of the most important facts in the history of cardiovascular disease is that it rose to dominance in the twentieth century. In the United States in 1900, heart disease was only about the fourth-leading cause of death, well behind infectious killers such as pneumonia, influenza, and tuberculosis. Within a few decades that ranking had been turned upside down. By the late 1950s, cardiovascular diseases accounted for roughly two-thirds of all deaths in the United States, and heart disease had become — and long remained — the leading cause of death in industrialized nations.
Part of this dramatic shift was, paradoxically, a sign of progress. As sanitation, vaccination, and (from the 1940s) antibiotics tamed the infectious diseases that had once killed people young, more individuals survived into middle and old age — the years in which atherosclerotic cardiovascular disease takes its toll. In that sense, the rise of heart disease partly reflected the defeat of other killers and a rising life expectancy. But that is not the whole story. The first half of the century also brought mass cigarette smoking, increasingly rich and calorie-dense diets, and more sedentary work and transport — an environment that genuinely increased the burden of atherosclerosis, not merely uncovered it.
By mid-century the scale of the problem was impossible to ignore: seemingly healthy, often prominent middle-aged men were dropping dead of heart attacks, and physicians had little ability to predict or prevent it. (The 1955 heart attack of U.S. President Dwight Eisenhower, reported in unusual clinical detail, crystallized public alarm.) Medicine grasped the pathology of a heart attack, thanks to the pathologists and to Herrick, but had almost no understanding of its causes at the population level — of why one person succumbed and another did not. Filling that gap is exactly what the great post-war epidemiological studies set out to do, and it is where the modern idea of cardiovascular disease as a preventable condition was born.
Framingham and the Birth of the "Risk Factor"
The landmark response to the mid-century epidemic was the Framingham Heart Study, launched in 1948 in the town of Framingham, Massachusetts, just west of Boston. Rather than studying people who were already sick, the Framingham investigators did something then unusual: they enrolled more than 5,000 healthy adult residents and followed them for decades, examining them every few years and recording, with each new heart attack and stroke, what had distinguished the people who fell ill from those who stayed well. It became the longest-running and most influential cardiovascular cohort study in history, eventually following the original participants' children and grandchildren.
Framingham's defining contribution was conceptual: it identified and popularized the now-ubiquitous idea of the cardiovascular "risk factor." The term entered wide medical use through a seminal 1961 Framingham paper by William Kannel and colleagues, "Factors of Risk in the Development of Coronary Heart Disease," which framed conditions such as high blood pressure, high blood cholesterol, and abnormal ECG findings as measurable predictors of future heart disease. Over the following years the study's data implicated the cluster now taught to every medical student and printed on every clinic poster: hypertension, elevated cholesterol, cigarette smoking, diabetes, obesity, and physical inactivity. The very phrasing of cardiovascular prevention — "know your numbers," "modify your risk factors" — descends directly from Framingham.
Honesty requires one clarification often glossed over in popular accounts. Framingham is frequently said to have invented the term "risk factor," but historians have shown the phrase appeared earlier — in occupational-health writing as far back as the 1920s and elsewhere in 1950s medicine. What Framingham did, decisively, was to give the concept rigorous epidemiological content for heart disease and to popularize it; the term itself did not gain broad momentum in medicine and public health until the mid-1970s. The accurate statement — and the one this page makes — is that the modern cardiovascular risk-factor framework was established and made famous by Framingham, crystallizing around Kannel's 1961 publication, rather than coined from nothing there.
Ancel Keys and the Diet-Heart Debate
While Framingham was mapping risk factors in one American town, the Minnesota physiologist Ancel Keys (1904–2004) was pursuing a related question across nations: did diet — specifically dietary fat — explain why some populations suffered far more heart disease than others? His vehicle was the Seven Countries Study, designed in 1958 and formally begun that autumn, which enrolled roughly 12,000–13,000 middle-aged men in 16 cohorts across the United States, Finland, the Netherlands, Italy, Yugoslavia, Greece, and Japan. It was the first major study to compare diet, blood cholesterol, and heart disease systematically across very different cultures.
Keys reported that populations eating more saturated fat tended to have higher blood cholesterol and higher rates of coronary heart disease, and that those eating a Mediterranean-style pattern rich in olive oil, vegetables, and fish fared better. From this work flowed the influential diet-heart hypothesis — the idea that saturated fat raises cholesterol, which in turn drives atherosclerosis — and much of the early scientific case for the now-celebrated Mediterranean diet. Keys's ideas shaped decades of dietary guidelines in the United States and beyond, helping to make "low saturated fat" a public-health watchword.
This is also one of the most genuinely contested chapters in cardiovascular history, and it deserves an honest accounting rather than a verdict. Critics have argued that the study selected and excluded countries in ways that may have favored its conclusion (the often-cited example is the exclusion of high-fat, relatively low-heart-disease France), that some dietary data — notably in Greece, partly collected during the Lenten fast — were distorted, and that sugar and refined carbohydrate were under-weighed as alternative culprits. Defenders counter that the central correlation between saturated fat, cholesterol, and heart disease has broadly held up and that the Mediterranean pattern remains well supported by later trials. The fair summary is that Keys's work was enormously influential and partly vindicated, yet methodologically criticized and incomplete; the precise role of different dietary fats and sugars in cardiovascular disease is still actively researched and debated today, and single-nutrient verdicts deserve caution.
The Rise and Partial Fall of Cardiovascular Death
The history of cardiovascular disease does not end with its rise — it includes a remarkable, and still incomplete, decline. After roughly sixty years of steady increase, age-adjusted death rates from coronary heart disease and stroke in the United States began an unexpected fall in the mid-1960s, a downturn first widely noticed and reported in the 1970s. By the year 2000, age-adjusted cardiovascular mortality had dropped to roughly one-third of its 1960s peak — one of the great public-health achievements of the twentieth century, and a direct payoff of the understanding assembled over the preceding centuries.
Analysts generally attribute this decline to two broad forces working together. The first is prevention: population-wide reductions in cigarette smoking, lower average blood-cholesterol levels, better detection and treatment of high blood pressure, and broad public-health campaigns — the practical application of the Framingham risk-factor concept and the diet-and-lifestyle lessons of Keys's era. The second is treatment: coronary care units, bystander CPR and portable defibrillators, clot-dissolving and clot-preventing drugs, coronary artery bypass surgery, angioplasty and stents, and medications such as statins and antihypertensives. Roughly speaking, studies credit about half the decline to risk-factor reduction and about half to medical and surgical treatment, though the exact split varies by population and period.
The honest closing note is that the victory is partial and possibly fragile. Cardiovascular disease remains the leading cause of death worldwide, and in some recent years and regions the long decline has slowed or stalled, pressured by rising obesity and type 2 diabetes. The arc — ancient and intrinsic, magnified into a twentieth-century epidemic, then beaten partway back by knowledge and effort — is not a finished story but an ongoing one. It is also a hopeful one: hard mortality data show that cardiovascular disease is substantially preventable and treatable, and that the cumulative work of Harvey, the pathologists, the instrument-makers, Framingham, and countless others translates into real years of life. The companion Cardiovascular Disease overview covers today's prevention and treatment in practical detail.
Research Papers and References
The references below combine peer-reviewed historical and scientific articles — with real DOIs or PubMed identifiers where verified — with curated PubMed topic-search links into the broader literature. Historical primary works (Harvey's De Motu Cordis, 1628; Herrick's 1912 JAMA paper; Kannel's 1961 Framingham paper) are named in the article as historical sources. Each link opens in a new tab at its publisher or at PubMed (National Library of Medicine).
- Ribatti D. William Harvey and the discovery of the circulation of the blood. Journal of Angiogenesis Research. 2009;1:3. — doi:10.1186/2040-2384-1-3
- Thompson R.C., Allam A.H., Lombardi G.P., et al. Atherosclerosis across 4000 years of human history: the Horus study of four ancient populations. The Lancet. 2013;381(9873):1211-1222. — doi:10.1016/S0140-6736(13)60598-X
- Allam A.H., Thompson R.C., Wann L.S., et al. Atherosclerosis in ancient Egyptian mummies: the Horus study. JACC: Cardiovascular Imaging. 2011;4(4):315-327. — doi:10.1016/j.jcmg.2011.02.002
- Herrick J.B. Clinical features of sudden obstruction of the coronary arteries (landmark article, JAMA 1912). — PubMed: PMID 6350634
- Mayerl C., Lukasser M., Sedivy R., et al. Atherosclerosis research from past to present — on the track of two pathologists with opposing views, Carl von Rokitansky and Rudolf Virchow. Virchows Archiv. 2006;449(1):96-103. — doi:10.1007/s00428-006-0176-7
- Kannel W.B., Dawber T.R., Kagan A., Revotskie N., Stokes J. Factors of risk in the development of coronary heart disease — six-year follow-up experience. The Framingham Study. Annals of Internal Medicine. 1961;55:33-50. — doi:10.7326/0003-4819-55-1-33
- Mahmood S.S., Levy D., Vasan R.S., Wang T.J. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. The Lancet. 2014;383(9921):999-1008. — doi:10.1016/S0140-6736(13)61752-3
- Oppenheimer G.M. Becoming the Framingham Study, 1947-1950. American Journal of Public Health. 2005;95(4):602-610. — doi:10.2105/AJPH.2003.026419
- Keys A., Menotti A., Karvonen M.J., et al. The diet and 15-year death rate in the Seven Countries Study. American Journal of Epidemiology. 1986;124(6):903-915. — doi:10.1093/oxfordjournals.aje.a114480
- Pett K.D., Willett W.C., Vartiainen E., Katz D.L. The Seven Countries Study. European Heart Journal. 2017;38(42):3119-3121. — doi:10.1093/eurheartj/ehx603
- Mensah G.A., Wei G.S., Sorlie P.D., et al. Decline in cardiovascular mortality: possible causes and implications. Circulation Research. 2017;120(2):366-380. — doi:10.1161/CIRCRESAHA.116.309115
- Dalen J.E., Alpert J.S., Goldberg R.J., Weinstein R.S. The epidemic of the 20th century: coronary heart disease. The American Journal of Medicine. 2014;127(9):807-812. — doi:10.1016/j.amjmed.2014.04.015
- History of blood-pressure measurement — Riva-Rocci, Korotkoff, and the sphygmomanometer — PubMed: history of blood-pressure measurement
- Willem Einthoven and the history of the electrocardiogram — PubMed: Einthoven and the history of the ECG
External Authoritative Resources
- NHLBI (NIH) — Heart and Vascular Diseases
- American Heart Association — Health Topics
- World Health Organization — Cardiovascular Diseases Fact Sheet
Connections
- Cardiology
- Cardiovascular Disease (Overview)
- Atherosclerosis
- Coronary Artery Disease
- Hypertension
- Heart Failure
- Stroke
- Cholesterol Management
- All Conditions