Helicobacter Pylori
Symptoms & Diagnosis
Burning pain, nausea, and how H. pylori is detected with a simple breath test.
Ulcers & Gastritis
How H. pylori erodes the stomach lining, causes ulcers, and triggers chronic inflammation.
Cancer Risk
The link between H. pylori, intestinal metaplasia, and gastric adenocarcinoma.
Diagnosis Tests
Urea breath test, stool antigen test, serology, and endoscopy with biopsy.
Treatment & Eradication
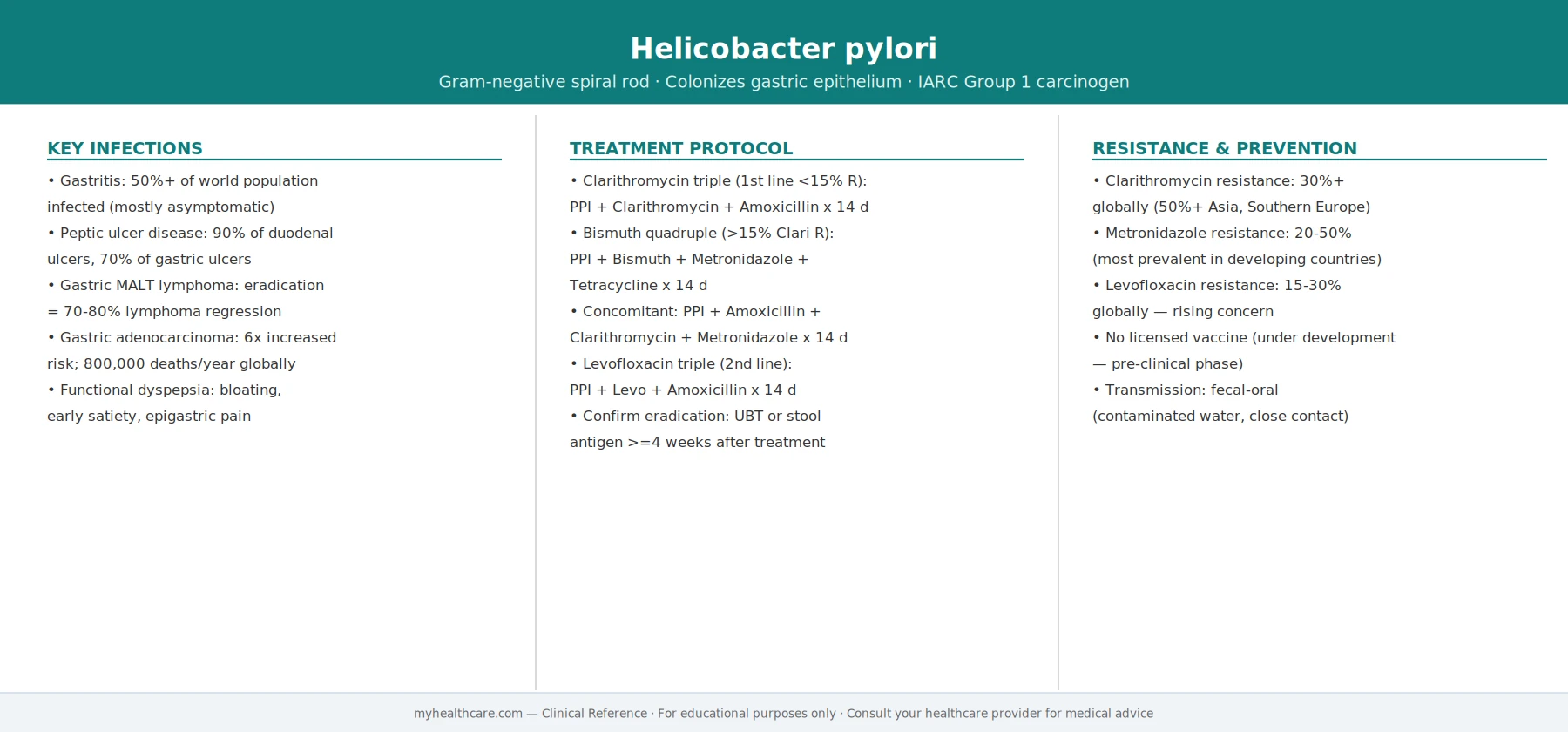
How H. pylori is cured — PPI-based triple and quadruple antibiotic regimens.
Antibiotic Therapy
Clarithromycin triple, bismuth quadruple, and sequential therapy protocols.
Diet & Prevention
Foods that protect the stomach, what to avoid, and preventing reinfection.
Antibiotic Resistance
Rising clarithromycin and metronidazole resistance, and what to use when first-line fails.
Helicobacter pylori (usually shortened to H. pylori) is a common stomach bacterium that most people have never heard of, yet it lives in the stomachs of roughly half the world's population. For most carriers it causes no trouble at all. But in a minority it quietly drives stomach inflammation, ulcers, and — over decades — a meaningful share of the world's stomach cancer. The good news: it is detectable with a simple breath or stool test, and it can usually be cured with a one- or two-week course of medicines. This page explains what H. pylori is, what it does, how doctors find it, and how it is treated, in plain language.
Table of Contents
- What H. pylori Is
- A Nobel-Prize Discovery
- What It Causes
- Symptoms
- Diagnosis
- Treatment — Eradication
- When to See a Doctor & Who Gets Tested
- Research Papers
- Connections
- Featured Videos
What H. pylori Is
Helicobacter pylori is a spiral-shaped (corkscrew-like) bacterium that colonizes the lining of the stomach. It is remarkably common: a large 2017 analysis estimated that about 4.4 billion people — more than half the world's population — carried the infection. Prevalence is much higher in developing regions and has been falling in wealthier countries as living conditions and sanitation have improved.
Most people who carry it picked it up in early childhood, often from close family contact, and the bacterium can quietly persist for the rest of a person's life if it is never treated. The stomach is one of the most hostile places in the body — its acid is strong enough to dissolve food and kill most microbes — but H. pylori has a clever trick. It produces an enzyme called urease, which breaks down urea into ammonia and carbon dioxide, neutralizing acid in the tiny zone right around the bacterium and letting it burrow into the protective mucus layer. That same urease is what several common tests exploit to detect the infection.
A Nobel-Prize Discovery
Until the 1980s, doctors were taught that stomach and duodenal ulcers were caused by stress, spicy food, and excess acid — and treatment focused on neutralizing acid, not curing anything. Two Australian researchers, gastroenterologist Barry Marshall and pathologist Robin Warren, overturned that dogma. Warren had repeatedly seen curved bacteria in stomach biopsies sitting right next to inflamed tissue, and together they argued the bacterium was the cause, not a bystander.
The medical establishment was deeply skeptical — everyone "knew" no bacterium could survive in stomach acid. To make his case, Marshall famously drank a culture of the bacteria himself and developed gastritis, helping demonstrate that the microbe caused stomach inflammation. Their work was eventually vindicated, and in 2005 Marshall and Warren were awarded the Nobel Prize in Physiology or Medicine "for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease." It remains one of medicine's great examples of a simple idea overturning accepted wisdom.
What It Causes
Here is the reassuring part first: most people who carry H. pylori never develop any disease from it at all. They live their whole lives with the bacterium and never know.
That said, when H. pylori does cause problems, they can be serious. It is the leading cause of chronic gastritis (long-term inflammation of the stomach lining) and is responsible for the majority of peptic ulcers — open sores in the lining of the stomach (gastric ulcers) or the first part of the small intestine (duodenal ulcers). Before this bacterium was understood, these ulcers were often a recurring, lifelong problem; once it is eradicated, the great majority of these ulcers heal and stay healed.
H. pylori is also classified by the World Health Organization's International Agency for Research on Cancer (IARC) as a Group 1 (definite) human carcinogen. It is the single most important risk factor for gastric (stomach) cancer and is also linked to a rare stomach immune-system cancer called MALT lymphoma. It is important to frame this honestly: the great majority of infected people will never develop stomach cancer, and infection alone is far from a cancer sentence. But the risk is real at a population level, and clearing the infection has been shown to reduce the chance of developing gastric cancer — which is a major reason doctors treat it. For MALT lymphoma confined to the stomach, eradicating H. pylori can by itself cause many of these tumors to regress.
Symptoms
In most carriers, H. pylori causes no symptoms whatsoever. When it does cause symptoms, they typically reflect the gastritis or ulcer it has produced, and may include:
- A burning, gnawing, or dull ache in the upper abdomen (often called dyspepsia), classically worse when the stomach is empty — for example between meals or during the night — and sometimes eased by eating or by antacids.
- Bloating and a feeling of fullness.
- Nausea, and sometimes a reduced appetite.
- Frequent burping or unexplained indigestion that keeps coming back.
These symptoms are common and have many possible causes, so they do not prove an H. pylori infection on their own. More worrying "alarm" symptoms — covered in the next-to-last section — need prompt medical attention rather than home remedies.
Diagnosis
There are several reliable ways to test for H. pylori, and the choice depends on the situation:
- Urea breath test. You swallow a harmless drink or capsule containing specially labeled urea. If H. pylori is present, its urease enzyme breaks the urea down and you exhale a marker that the test detects. It is highly accurate and detects an active, current infection.
- Stool antigen test. A lab checks a stool sample for proteins (antigens) from the bacterium. Like the breath test, it detects active infection, and it is accurate and inexpensive.
- Blood antibody test. This looks for antibodies to H. pylori. It is less useful, because antibodies can linger for years — so a positive result cannot tell whether the infection is active now or was cleared in the past. It is generally not preferred when better tests are available.
- Endoscopy with biopsy. A thin camera is passed into the stomach and small tissue samples are taken. This is used when there are alarm features, or in older patients, where it is important to look directly at the stomach lining (for example, to rule out cancer).
The breath test and stool antigen test are both the preferred ways to confirm that treatment worked (a "test of cure").
One practical point that genuinely matters: several common medicines can suppress the bacteria enough to produce a false-negative result on breath and stool tests — making it look like the infection is gone when it is not. In general, proton pump inhibitors (PPIs) such as omeprazole should be stopped for about 1–2 weeks, and antibiotics and bismuth for about 4 weeks, before a breath or stool test. Your doctor may bridge you with a different type of acid medicine in the meantime. Always follow your clinician's specific instructions on what to stop and for how long.
Treatment — Eradication
H. pylori is never treated with a single antibiotic — used alone, antibiotics fail and the bacteria can become resistant. Instead, doctors use combination therapy: an acid-lowering drug (a PPI) plus two or more antibiotics, taken together for about 10 to 14 days.
A widely used first-line option is bismuth quadruple therapy — a PPI, bismuth (the active ingredient in some over-the-counter stomach remedies), and two antibiotics — which is especially favored in regions where resistance to the antibiotic clarithromycin is high. The reason regimens have shifted over the years, and the main reason treatments fail, is growing antibiotic resistance. Because of this, the exact combination a doctor chooses depends increasingly on local resistance patterns and on which antibiotics a patient has taken before.
Two things make the difference between success and failure:
- Finishing the full course. These regimens involve several pills a day and can cause side effects like a metallic taste, nausea, or loose stools, which tempts people to stop early. Stopping early is a leading cause of treatment failure and resistance — take every dose for the full prescribed period.
- Confirming the cure. After treatment, a test of cure (a urea breath test or stool antigen test) should be done at least 4 weeks after finishing the antibiotics, and after pausing PPIs as described above, to make sure the bacterium is truly gone. If it is not, a different combination is used for a second attempt.
When to See a Doctor & Who Gets Tested
Medical guidelines follow a "test-and-treat" approach: if H. pylori is found in someone who should be tested, it should be treated. Groups in whom testing is recommended include people with:
- An active or past peptic ulcer (stomach or duodenal).
- Certain cases of ongoing indigestion (dyspepsia), particularly in younger patients without alarm features.
- A family history of stomach cancer.
- MALT lymphoma of the stomach.
- Long-term use of certain medicines, or other reasons identified by their doctor.
Some symptoms are "alarm features" that mean you should seek medical care promptly and will usually need an endoscopy rather than testing alone. See a doctor without delay if you have any of the following:
- Difficulty or pain swallowing.
- Unintended weight loss.
- Vomiting blood, or vomit that looks like coffee grounds.
- Black, tarry, or bloody stools (a sign of bleeding in the digestive tract).
- Anemia (low blood count), unexplained or found on blood tests.
- Persistent vomiting.
These can be signs of a bleeding ulcer or other serious problem and should never be managed with home remedies alone.
Research Papers
- Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1(8390):1311–1315. doi:10.1016/S0140-6736(84)91816-6 — The landmark paper that first linked the bacterium to gastritis and ulcers, launching a revolution in how these diseases are understood.
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017;112(2):212–239. doi:10.1038/ajg.2016.563 — The American College of Gastroenterology's authoritative guidance on which combination therapies to use and how to confirm a cure.
- Malfertheiner P, Megraud F, Rokkas T, et al. Management of Helicobacter pylori infection: the Maastricht VI/Florence consensus report. Gut. 2022;71(9):1724–1762. doi:10.1136/gutjnl-2022-327745 — The leading European consensus on diagnosis and treatment, emphasizing tailoring therapy to local antibiotic resistance.
- Hooi JKY, Lai WY, Ng WK, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology. 2017;153(2):420–429. doi:10.1053/j.gastro.2017.04.022 — Estimated about 4.4 billion people — more than half the world's population — were infected in 2015, with wide regional variation.
- Ford AC, Forman D, Hunt RH, Yuan Y, Moayyedi P. Helicobacter pylori eradication therapy to prevent gastric cancer in healthy asymptomatic infected individuals: systematic review and meta-analysis of randomised controlled trials. BMJ. 2014;348:g3174. doi:10.1136/bmj.g3174 — Pooled trials found eradication reduced the risk of gastric cancer (relative risk about 0.66), supporting treatment as a prevention strategy.
Connections
- All Bacteria
- Peptic Ulcer Disease
- GERD
- Inflammatory Bowel Disease
- Gastroenterology Conditions
- All Conditions
- Stomach Cancer