H. pylori Eradication: Triple and Quadruple Antibiotic Therapy
Getting rid of Helicobacter pylori takes more than a single antibiotic — the bacterium lives deep in the mucus lining of your stomach, an acidic environment that degrades most drugs before they can reach their target. The solution doctors settled on is combination therapy: two or three antibiotics taken at the same time as an acid-suppressing drug that makes the stomach less hostile, so the antibiotics can do their job. This page explains the main regimens in plain language — what each drug does, what success rates to expect, how to handle side effects, and what happens if your first round does not work.
Table of Contents
- Clarithromycin-Based Triple Therapy
- Bismuth Quadruple Therapy
- Concomitant (Non-Bismuth Quadruple) Therapy
- Sequential Therapy
- High-Dose Dual Therapy
- Vonoprazan-Based Regimens
- Side Effects and Practical Patient Tips
- Confirming Cure and Salvage After Two Failed Courses
- Key Research Papers
- Connections
- Featured Videos
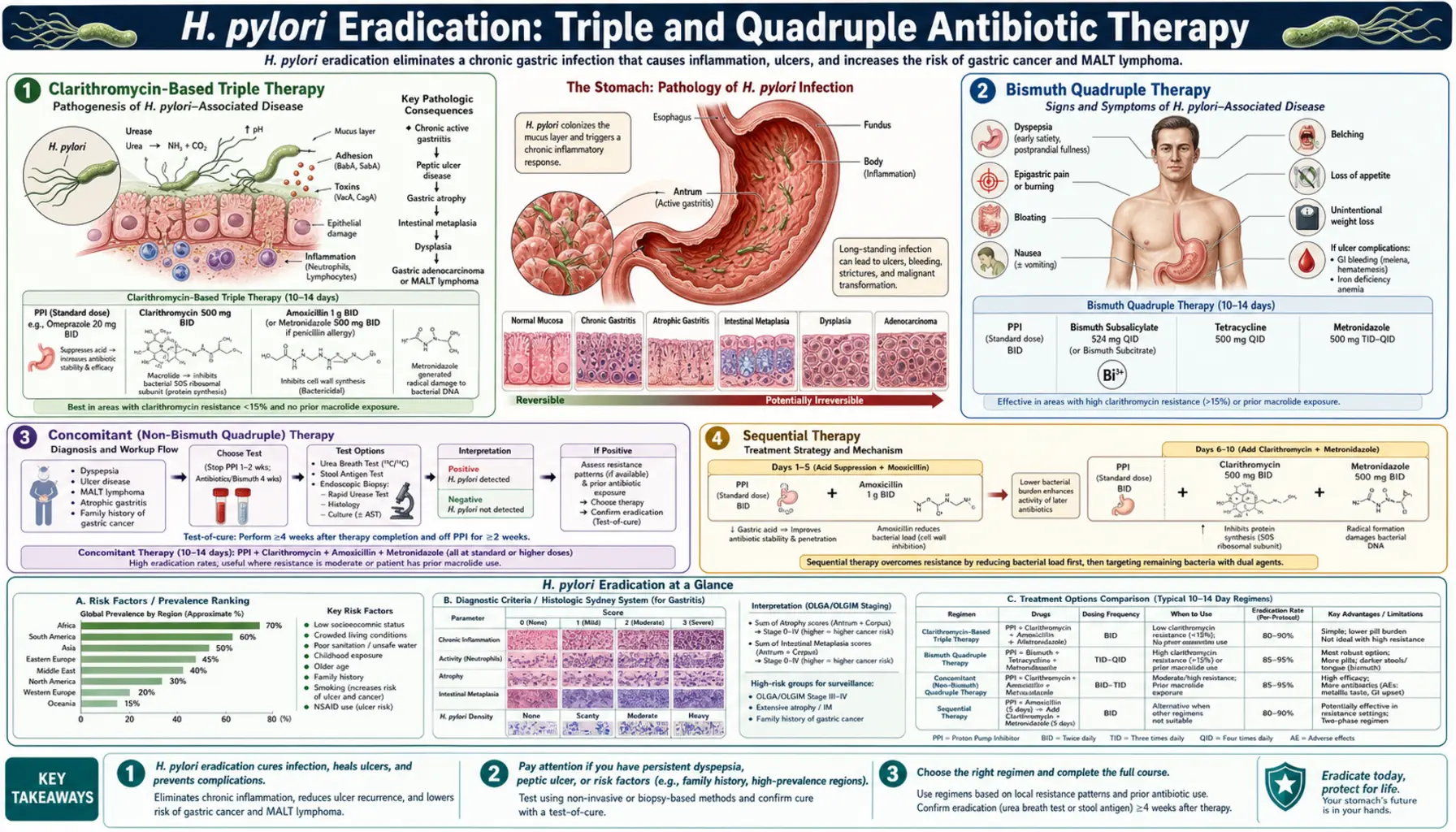
Clarithromycin-Based Triple Therapy
For roughly two decades this was the default first treatment for H. pylori in most of the world. The regimen combines three drugs taken twice a day for 14 days:
- A proton pump inhibitor (PPI) such as omeprazole, lansoprazole, or esomeprazole. PPIs block the acid-producing pumps in your stomach lining, raising the pH high enough for antibiotics to remain stable and active.
- Clarithromycin — a macrolide antibiotic that works by stopping the bacteria from making proteins they need to survive.
- Amoxicillin — a penicillin-type antibiotic that punches holes in the bacterial cell wall. If you are allergic to penicillin, metronidazole is substituted.
When local clarithromycin resistance rates are below 15%, triple therapy still achieves around 80% eradication on the first try — a reasonable result for a regimen that is well tolerated and inexpensive. However, in many Western cities and throughout East Asia, resistance rates have climbed above 20–30%, dropping cure rates to 60–70% or lower. For this reason, most major guidelines now recommend testing for clarithromycin resistance (via culture or PCR) before prescribing this regimen, or reserving it for regions where resistance surveillance confirms it is still effective. The American College of Gastroenterology updated its position in 2017 to recommend bismuth quadruple therapy or concomitant therapy as preferred first-line options where resistance data are lacking.
Duration matters: 14-day courses outperform 7-day courses by roughly 5–10 percentage points in eradication rate, and that difference is clinically meaningful when you are trying to avoid a second course of antibiotics.
Bismuth Quadruple Therapy
This regimen adds bismuth — the same compound found in Pepto-Bismol — to a three-drug backbone. The standard schedule, taken for 10 to 14 days, is:
- PPI twice daily (acid suppression)
- Bismuth subcitrate or subsalicylate four times daily. Bismuth coats the stomach lining and has a direct toxic effect on H. pylori without being an antibiotic in the conventional sense. Because bacteria cannot easily develop resistance to bismuth, this drug remains effective even when the antibiotics in the regimen have partial resistance.
- Tetracycline four times daily — a broad-spectrum antibiotic that, like clarithromycin, interrupts bacterial protein synthesis, but via a different binding site that clarithromycin-resistant strains typically cannot block.
- Metronidazole three or four times daily. This antibiotic is chemically activated inside bacterial cells into a form that damages their DNA. When combined with bismuth and tetracycline, even strains with partial metronidazole resistance are often cleared.
Bismuth quadruple therapy achieves eradication rates of 85–90% in most clinical trials, even in populations with high clarithromycin resistance. It is the preferred first-line regimen according to the 2017 ACG guidelines and the Maastricht V European Consensus whenever resistance data are not available or resistance is suspected. The main drawback is pill burden: patients take 14 or more tablets per day, spread across four dosing times. Bismuth can also turn stools and the tongue temporarily dark — this is harmless but alarming if you are not warned in advance.
One practical note: in the United States, bismuth subcitrate is sold as the combination product Pylera (bismuth subcitrate + tetracycline + metronidazole in a single capsule taken four times daily plus a separate PPI), which dramatically simplifies the pill count and has been shown to achieve approximately 93% eradication in intention-to-treat analyses.
Concomitant (Non-Bismuth Quadruple) Therapy
Concomitant therapy takes a different approach to the resistance problem: rather than using bismuth, it combines all four active agents — a PPI plus clarithromycin, amoxicillin, and metronidazole — taken simultaneously for 10 to 14 days.
The rationale is straightforward: if a strain is resistant to one antibiotic, the other two are still active. Because resistance to all three antibiotics at once in the same bacterial strain is statistically rare, concomitant therapy maintains high eradication rates of 85–90% even in areas with dual (clarithromycin plus metronidazole) resistance rates that would each individually undermine a two-drug regimen.
This regimen is gaining favor in Europe and parts of Asia where bismuth is not readily available. Side effects are somewhat more frequent than with triple therapy — more antibiotics means more nausea, diarrhea, and disruption to normal gut bacteria — but most people complete the course without serious problems. As with any regimen that includes clarithromycin, its value is diminished in areas where local clarithromycin resistance exceeds 15–20%.
Sequential Therapy
Sequential therapy was designed to defeat clarithromycin resistance through a two-stage assault. The idea is that a preliminary course of amoxicillin weakens the bacterial cell wall, making it harder for bacteria to pump clarithromycin out before it can act. The schedule:
- Days 1–5: PPI twice daily + amoxicillin 1 g twice daily
- Days 6–10: PPI twice daily + clarithromycin 500 mg twice daily + metronidazole 500 mg twice daily (or tinidazole)
Early Italian studies from the 2000s reported eradication rates above 90% for sequential therapy versus 76% for standard triple therapy. These results generated significant enthusiasm, and for several years sequential therapy was recommended as first-line in Italy and some other European countries.
However, later meta-analyses including populations from East Asia, the Middle East, and the Americas found that sequential therapy performed no better than concomitant therapy, and it failed more predictably in strains with dual clarithromycin-plus-metronidazole resistance. Most current guidelines — including the 2017 ACG and Maastricht V — rate sequential therapy as acceptable but not preferred over concomitant therapy, and not clearly superior to bismuth quadruple therapy. Its main advantage is a slightly lower pill count in the first five days.
High-Dose Dual Therapy
High-dose dual therapy (HDDT) strips the regimen back to just two drugs: a very high dose of a PPI plus amoxicillin taken four times per day. The typical protocol is:
- Amoxicillin 750 mg to 1 g four times daily for 14 days
- High-dose PPI — for example, esomeprazole 40 mg or rabeprazole 20 mg — three or four times daily
The reasoning: amoxicillin resistance in H. pylori is genuinely rare (below 1–2% globally), so amoxicillin remains effective almost everywhere. The obstacle has always been drug stability in acid — amoxicillin is rapidly degraded at low pH. By taking a high-dose PPI multiple times daily, the stomach pH is raised more consistently than with conventional twice-daily dosing, allowing amoxicillin to reach and kill bacteria without being inactivated first.
Meta-analyses from Taiwan, where this approach was pioneered, have reported eradication rates of 85–90% for HDDT. Comparable results are emerging in US and European trials, particularly with the newer potassium-competitive acid blockers (see below). Because amoxicillin is well tolerated and H. pylori does not readily develop resistance to it, HDDT is especially attractive in patients who have already failed a clarithromycin-containing regimen or in areas of high clarithromycin resistance. It also avoids metronidazole, another drug with rising resistance rates.
Vonoprazan-Based Regimens
Vonoprazan (brand name Voquezna in the United States) belongs to a new class of acid suppressants called potassium-competitive acid blockers, or P-CABs. Unlike conventional PPIs, which require activation in an acidic environment and take several days to reach full effect, vonoprazan works immediately and maintains stomach pH above 6 for longer periods throughout the day — including during meals and at night, when PPIs typically lose their grip.
This superior acid suppression has two consequences for H. pylori eradication:
- Antibiotics that are acid-labile — amoxicillin in particular — survive longer in the stomach and penetrate the mucus layer more effectively.
- Many PPIs are metabolized rapidly by an enzyme called CYP2C19, meaning that fast metabolizers clear the drug quickly and get subtherapeutic acid suppression. Vonoprazan largely bypasses CYP2C19, so its effect is more predictable across genetic subtypes.
The landmark VOCAL-1 and VOCAL-2 trials conducted in the United States tested two vonoprazan-based regimens against bismuth quadruple therapy:
- Vonoprazan triple therapy: vonoprazan 20 mg twice daily + amoxicillin 1 g twice daily + clarithromycin 500 mg twice daily × 14 days. Eradication rate approximately 78–80% (intention-to-treat), broadly comparable to bismuth quadruple therapy.
- Vonoprazan dual therapy: vonoprazan 20 mg twice daily + amoxicillin 1 g three times daily × 14 days. Eradication rate approximately 80–84% (intention-to-treat) — matching or exceeding triple therapy with fewer antibiotics and less disruption to gut flora.
The FDA approved vonoprazan-based regimens for H. pylori eradication in May 2022, making them available in the US. In Japan, where vonoprazan has been used since 2015, real-world data confirm eradication rates consistently in the 85–90% range for vonoprazan-amoxicillin dual therapy. These regimens are now recommended as first-line options in the 2022 ACG guidelines update for the United States.
Vonoprazan costs considerably more than generic PPIs, but for patients who have failed one prior course of antibiotics — or in whom a test shows high local clarithromycin resistance — the improved acid suppression and the option of a two-drug amoxicillin-only backbone may justify the extra expense.
Side Effects and Practical Patient Tips
All eradication regimens carry a risk of side effects, but most are manageable if you know what to expect.
Common side effects by drug
- Clarithromycin: A persistent metallic or bitter taste in the mouth is the most frequently reported complaint — up to 30% of patients notice it. Nausea and stomach upset are also common. Taking clarithromycin with food significantly reduces nausea.
- Metronidazole: Also causes metallic taste. More importantly, it causes a severe and dangerous reaction with alcohol — nausea, flushing, rapid heartbeat, and vomiting. Avoid all alcohol for the entire course plus 48 hours afterward.
- Amoxicillin: Diarrhea and loose stools are the main issues. Soft, loose stools for a few days are normal; watery or bloody diarrhea should be reported to your doctor immediately (see C. diff below).
- Tetracycline: Makes your skin significantly more sensitive to sunlight. Wear sunscreen and protective clothing while taking it. Do not take tetracycline with dairy products, antacids, or iron supplements — they bind to tetracycline in the gut and prevent absorption. Take it on an empty stomach, or at least two hours away from these foods.
- Bismuth: Turns stools dark or black and can temporarily discolor the tongue. This is harmless. Do not confuse dark stools from bismuth with black tarry stools from a bleeding ulcer — if you have stomach pain alongside dark stools, call your doctor.
- PPIs (all): Headache and mild diarrhea are the most common complaints. Long-term PPI use (months to years) carries small risks of magnesium and vitamin B12 deficiency, but a 10–14 day eradication course does not produce these problems.
Risk of Clostridioides difficile (C. diff)
Any antibiotic course can disturb the normal gut bacteria and allow C. difficile to overgrow, causing severe, watery, foul-smelling diarrhea that can begin during or up to 8 weeks after completing antibiotics. The risk is small for a 14-day eradication course, but it is real. If you develop more than three watery stools per day during or after treatment, contact your doctor — this needs testing and specific treatment. Taking a probiotic (such as Lactobacillus rhamnosus GG or Saccharomyces boulardii) alongside antibiotics modestly reduces diarrhea risk, though it does not reliably improve eradication rates.
Tips for completing the course
- Set phone alarms for every dose — missing doses is the single biggest reason eradication fails.
- Take antibiotics with a full meal rather than on an empty stomach (except tetracycline — see above).
- Take PPIs 30 minutes before eating, not with food, to maximize their acid-suppressing effect.
- Avoid smoking during and after treatment — smoking reduces mucosal blood flow, slows healing, and is associated with lower eradication rates.
- Do not stop early even if you feel better. H. pylori is not eliminated until the full course is finished.
Confirming Cure and What to Do After Two Failed Courses
Testing for successful eradication
Symptoms alone cannot confirm eradication — the bacteria may still be present even if your stomach feels better. The standard approach is to retest four weeks after completing the antibiotic course (and at least two weeks after stopping any PPI). The preferred non-invasive tests are:
- Urea breath test (UBT): You swallow a capsule or drink containing labeled urea. If H. pylori is still present, it breaks down the urea and the labeled carbon appears in your exhaled breath. Sensitivity and specificity both exceed 95%. This is the gold standard for confirming cure.
- Stool antigen test: Detects H. pylori proteins in a stool sample. Sensitivity is slightly lower than UBT but still above 90%, and it is widely available without a specialist visit.
Blood antibody tests are not useful for confirming eradication — antibodies remain positive for months to years after the infection is cleared and cannot distinguish active from past infection.
If the first course fails
Eradication failure usually means antibiotic resistance. Your doctor's next step should ideally be resistance testing via upper endoscopy with biopsy for culture and sensitivity, or a molecular PCR panel. Armed with that information, the second regimen can be chosen specifically to avoid the resistant drugs. If testing is not available:
- If first-line was triple therapy (clarithromycin + amoxicillin), switch to bismuth quadruple therapy or a vonoprazan-based regimen.
- If first-line was bismuth quadruple therapy, switch to levofloxacin triple therapy (PPI + levofloxacin + amoxicillin) or a vonoprazan-amoxicillin dual regimen.
After two failed courses, culture-guided therapy is strongly preferred — empiric third-line therapy risks further selecting resistant strains. Salvage options at this stage include rifabutin-based therapy (PPI + rifabutin + amoxicillin), which uses an antibiotic from the tuberculosis toolkit that H. pylori rarely resists, or high-dose dual therapy with vonoprazan if not already used. Specialist gastroenterology referral is appropriate after two treatment failures.
Key Research Papers
The following peer-reviewed studies underpin the treatment recommendations described on this page.
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am J Gastroenterol. 2017. — Search PubMed
- Fallone CA, Chiba N, van Zanten SV, et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology. 2016. — Search PubMed
- Malfertheiner P, Megraud F, O'Morain CA, et al. Management of Helicobacter pylori infection — the Maastricht V/Florence Consensus Report. Gut. 2017. — Search PubMed
- Nyssen OP, McNicholl AG, Megraud F, et al. Sequential versus standard triple first-line therapy for Helicobacter pylori eradication. Cochrane Database Syst Rev. 2016. — Search PubMed
- Luther J, Higgins PDR, Schoenfeld PS, Moayyedi P, Vakil N, Chey WD. Empiric quadruple vs. triple therapy for primary treatment of Helicobacter pylori infection: Systematic review and meta-analysis of efficacy and tolerability. Am J Gastroenterol. 2010. — Search PubMed
- Romano M, Cuomo A, Gravina AG, et al. Empirical levofloxacin-containing versus clarithromycin-containing sequential therapy for Helicobacter pylori eradication. Gut. 2010. — Search PubMed
- Megraud F, Bruyndonckx R, Coenen S, et al. Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut. 2021. — Search PubMed
- Rokkas T, Georgopoulos SD, Niv Y, O'Morain C. Efficacy of vonoprazan-based versus proton pump inhibitor-based triple therapy for Helicobacter pylori eradication: a systematic review and meta-analysis. Ann Gastroenterol. 2021. — Search PubMed
- Graham DY, Dore MP. Update on the use of bismuth to treat Helicobacter pylori infections. Clin Infect Dis. 2016. — Search PubMed
- Hsu PI, Wu DC, Chen WC, et al. Randomized controlled trial comparing 7-day triple, 10-day sequential, and 7-day concomitant therapies for Helicobacter pylori infection. Antimicrob Agents Chemother. 2014. — Search PubMed
- McNicholl AG, Linares PM, Nyssen OP, Calvet X, Gisbert JP. Meta-analysis: esomeprazole or rabeprazole vs. first-generation pump inhibitors in the treatment of Helicobacter pylori infection. Aliment Pharmacol Ther. 2012. — Search PubMed
- Chey WD, Mégraud F, Laine L, et al. Vonoprazan triple and dual therapy for Helicobacter pylori infection in the United States and Europe: Randomized Clinical Trial. Gastroenterology. 2022. — Search PubMed
- Graham DY, Lee YC, Wu MS. Rational Helicobacter pylori therapy: evidence-based medicine rather than medicine-based evidence. Clin Gastroenterol Hepatol. 2014. — Search PubMed
Connections
- All Bacteria
- H. pylori — Main Hub
- H. pylori Treatment & Eradication Overview
- Clarithromycin and Metronidazole Resistance
- Diet and Prevention for H. pylori
- Peptic Ulcer Disease