Campylobacter Treatment and Prevention: Rehydration, Antibiotics, and Food Safety
Campylobacter jejuni infection causes more foodborne illness in the United States than almost any other bacterial pathogen — roughly 1.5 million cases per year. Most patients recover on their own within a week. This page covers when to treat, how to stay hydrated, who genuinely needs antibiotics, and how to prevent the infection in the first place through safe food handling.
Antibiotic Treatment
When antibiotics are needed, azithromycin as first choice, and why ciprofloxacin often fails.
Food Safety
Poultry handling, cooking temperatures, and preventing cross-contamination at home.
Antibiotic Resistance
How veterinary fluoroquinolone use in poultry created a global resistance crisis.
Symptoms & Overview
The typical illness course, high-risk groups, and post-infectious complications.
- Most Cases Are Self-Limiting
- Rehydration: The Core Treatment
- When Antibiotics Are Indicated
- Antibiotic Options Overview
- Preventing Guillain-Barré Syndrome
- Food Safety and Prevention
- Antibiotic Stewardship
- Practical Guidance for High-Risk Groups
- Key Research Papers
- Connections
- Featured Videos
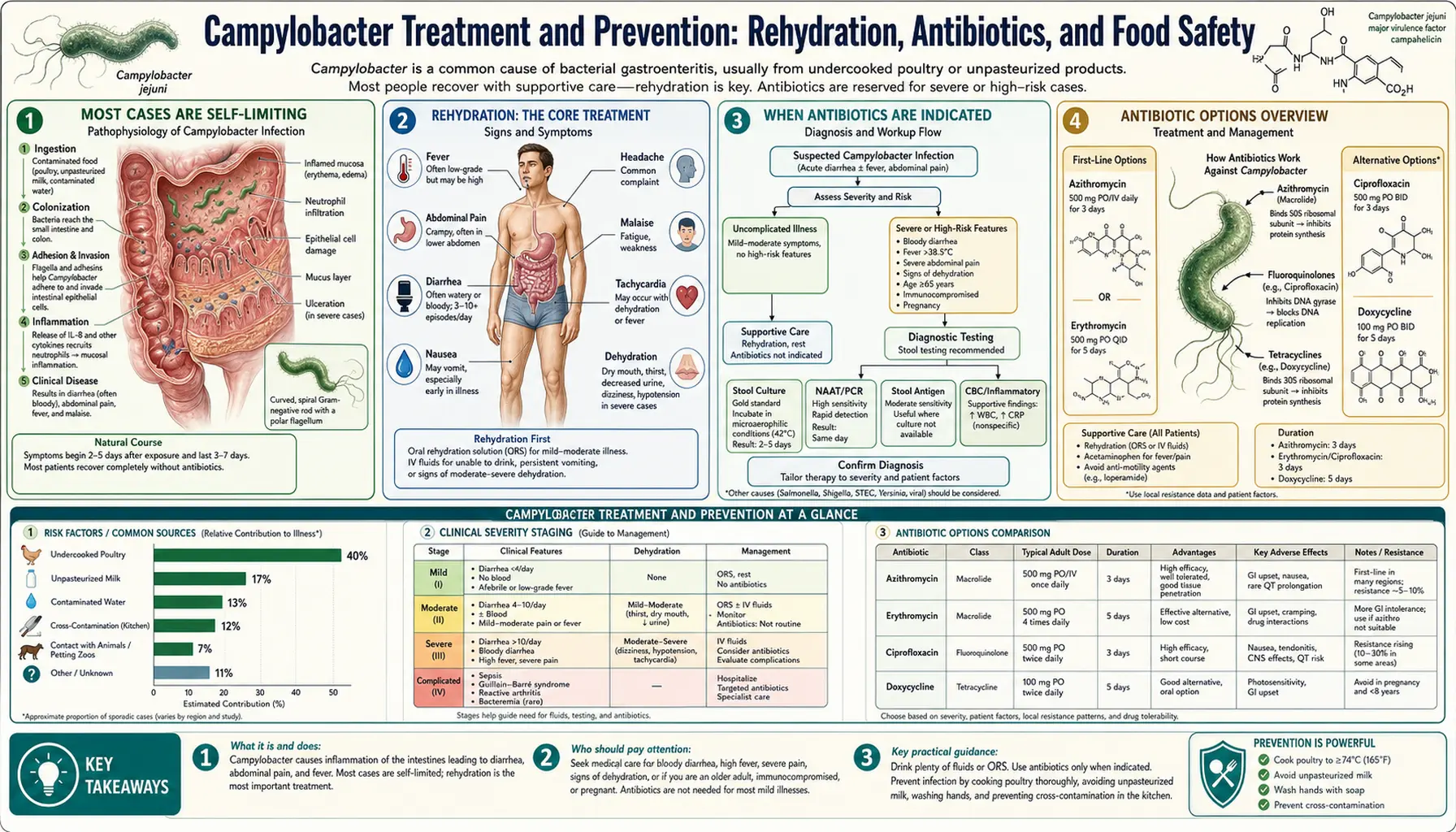
Most Cases Are Self-Limiting
The most important thing to understand about Campylobacter jejuni infection is that the healthy adult body clears it without any antibiotic help. In otherwise healthy people, the illness runs its course in three to seven days, with symptoms peaking around days two through four and then improving naturally as the immune system mounts a response.
Clinical trials examining antibiotic treatment for Campylobacter diarrhea have consistently shown a modest benefit at best. A landmark systematic review found that antibiotics shorten the duration of illness by an average of approximately 1.3 days — a real but limited benefit. This means that a person who would have been sick for five days might recover in about four days with antibiotics, a difference that matters in severe illness but rarely justifies treatment when disease is mild.
There is also a practical timing problem. Stool cultures — the gold-standard test for identifying Campylobacter and determining antibiotic sensitivities — take 48 to 72 hours to return results. By that point, most patients with mild to moderate illness are already past their worst symptoms and well on their way to recovery. Treating everyone with antibiotics while awaiting culture results would expose millions of people to drug side effects and contribute to the global antibiotic resistance problem without meaningful benefit in most cases.
The clinical decision to treat rests on the severity of illness and the vulnerability of the host — not on the culture result alone. A healthy 30-year-old with three days of watery diarrhea who is staying hydrated is not a candidate for antibiotics. A 65-year-old who is immunosuppressed after a kidney transplant and has profuse bloody diarrhea and a fever of 40°C is a very different situation.
Rehydration: The Core Treatment
Regardless of whether antibiotics are used, rehydration is the cornerstone of treatment for every patient. Campylobacter diarrhea can cause significant fluid and electrolyte losses, especially in children, the elderly, and anyone who vomits as well as having diarrhea. Replacing those losses prevents the complications that turn a self-limited illness into a medical emergency.
Oral rehydration solution (ORS) is the most effective and evidence-based approach to fluid replacement. The World Health Organization ORS formula uses a precise sodium-to-glucose ratio (sodium 75 mmol/L, glucose 75 mmol/L) that exploits the sodium-glucose cotransporter in the intestinal wall to maximize fluid absorption even when the gut is inflamed. Commercially available ORS sachets (Pedialyte, Hydralyte, WHO-standard packets) deliver this ratio reliably. Plain water alone does not adequately replace electrolytes.
What to drink: water with ORS dissolved in it, clear broth (chicken or vegetable), diluted sports drinks, and coconut water can all contribute to fluid replacement. Rice water — water left over from cooking plain white rice — is a traditional remedy with some evidence for reducing stool volume in diarrheal illness.
What to avoid during illness: alcohol (worsens dehydration and irritates the gut), high-caffeine drinks in large amounts (mild diuretic effect), undiluted sugary drinks like full-strength soda or fruit juice (high osmolality can worsen diarrhea through osmotic effect), and dairy products if lactose intolerance is triggered by gut inflammation.
Warning signs that dehydration is worsening and requires medical attention:
- Dizziness or lightheadedness when standing up (orthostatic hypotension)
- No urination for 8 or more hours in adults
- No wet diaper for 6 or more hours in infants
- Sunken eyes or dry mouth in children
- Rapid heart rate or weak pulse
- Extreme fatigue, confusion, or inability to keep any fluids down
Intravenous (IV) fluids are indicated when oral intake is insufficient — typically when vomiting prevents the patient from keeping ORS down, or when signs of moderate to severe dehydration are present on examination. Normal saline or lactated Ringer's solution are standard IV choices in this setting. Most patients who require IV fluids need only a few hours of rehydration before they can transition back to oral intake.
When Antibiotics Are Indicated
Antibiotic treatment is appropriate in specific clinical situations where the risk-benefit calculation tips decisively in favor of treatment. These are not arbitrary rules — they reflect the populations where antibiotics demonstrably change outcomes.
Severe disease regardless of immune status:
- High fever above 39°C (102.2°F)
- Profuse bloody diarrhea
- Diarrhea lasting more than one week without improvement
- Signs of dehydration requiring IV fluids
- Clinical evidence of systemic illness (bacteremia, meningitis, reactive arthritis)
Immunocompromised patients: People with impaired immunity are at risk for Campylobacter bacteremia — where the bacteria invade the bloodstream from the gut — and for prolonged, severe illness that the immune system cannot resolve on its own. This includes:
- HIV/AIDS, especially with low CD4 counts
- Solid organ or bone marrow transplant recipients on immunosuppressive drugs
- People undergoing active chemotherapy
- Long-term high-dose corticosteroid users
- Asplenia (absent spleen, whether surgical or functional)
- Hypogammaglobulinemia or other primary antibody deficiencies
Age extremes: Elderly patients and very young infants with severe symptoms may benefit from antibiotics even without confirmed immunosuppression, given reduced physiological reserve.
Confirmed bacteremia: Blood culture positive for Campylobacter requires antibiotic treatment regardless of symptom severity, as untreated bacteremia can lead to seeding of distant sites including heart valves and joints.
Occupational indications: Healthcare workers, food handlers, and childcare workers may receive antibiotic treatment to shorten the period of fecal shedding and reduce transmission risk to vulnerable contacts — even when their own illness is relatively mild. Campylobacter can be shed in stool for 2-7 weeks after recovery without antibiotics.
Pregnancy: Campylobacter infection during pregnancy carries a risk of premature labor, fetal loss, and neonatal infection. Pregnant women with confirmed or strongly suspected Campylobacter gastroenteritis are generally offered antibiotic treatment, balancing fetal risk against drug safety profiles.
Antibiotic Options Overview
The antibiotic landscape for Campylobacter treatment has shifted dramatically over the past two decades. What was once a straightforward choice — ciprofloxacin or another fluoroquinolone — is now complicated by widespread fluoroquinolone resistance that renders this entire drug class unreliable in many parts of the world.
Azithromycin is now the preferred first-line antibiotic for Campylobacter infection in most regions. It belongs to the macrolide class and has maintained susceptibility rates above 90% in most high-income countries, compared to fluoroquinolone resistance rates that have climbed to 50-80% in many European nations and even higher in parts of Asia.
Why ciprofloxacin often fails: Fluoroquinolone resistance in Campylobacter is mediated primarily by point mutations in the gyrA gene that alter the target enzyme, DNA gyrase. These mutations arise rapidly under selective pressure. A patient who acquired Campylobacter from imported poultry or traveled internationally has a high probability of carrying a fluoroquinolone-resistant strain. Prescribing ciprofloxacin empirically without susceptibility data in high-resistance regions means a substantial fraction of patients receive an ineffective drug.
The full details of azithromycin dosing, fluoroquinolone resistance mechanisms, alternative agents for treatment failures, and resistance testing are covered in the dedicated sub-article: Antibiotic Treatment.
The broader story of how veterinary fluoroquinolone use in poultry farming created this public health crisis is documented in: Antibiotic Resistance.
Preventing Guillain-Barré Syndrome
Guillain-Barré syndrome (GBS) is the most feared complication of Campylobacter infection — a rare but potentially severe immune attack on the peripheral nervous system that can cause ascending paralysis. Approximately 1 in 1,000 to 1 in 2,000 Campylobacter infections triggers GBS, making Campylobacter the single most commonly identified antecedent infection for this condition.
The hard truth is that no specific intervention can reliably prevent GBS once Campylobacter diarrhea has started. The immune response that eventually cross-reacts with nerve myelin is already in motion when the intestinal illness begins. GBS typically appears 1 to 4 weeks after the diarrheal illness resolves, by which point the original infection is over.
Can early antibiotic treatment reduce GBS risk? This is theoretically plausible — by reducing the bacterial load in the gut sooner, antibiotics might limit exposure to the LOS (lipooligosaccharide) antigens on Campylobacter that molecularly mimic gangliosides on nerve membranes. However, there are no completed randomized controlled trials demonstrating that antibiotic treatment of Campylobacter enteritis reduces GBS incidence. The evidence gap is partly due to the rarity of GBS (making trials logistically difficult) and partly because by the time GBS risk becomes apparent — 1-4 weeks post-diarrhea — the treatment decision window has long passed.
What to watch for: Anyone who has had Campylobacter diarrhea should be aware of GBS warning signs in the weeks following recovery:
- Tingling or pins-and-needles sensation starting in the feet or hands
- Progressive leg weakness, especially difficulty climbing stairs
- Difficulty walking, unsteady gait
- Back pain combined with leg weakness
- Facial weakness, difficulty swallowing or speaking
- Shortness of breath (a red flag for respiratory muscle involvement)
Any of these symptoms after a recent diarrheal illness warrant emergency evaluation. GBS can progress to respiratory failure within hours. The treatments for GBS itself — intravenous immunoglobulin (IVIG) and plasmapheresis — are most effective when started early in the disease course. Full details are in: Guillain-Barré Syndrome.
Food Safety and Prevention
Campylobacter jejuni is fundamentally a food safety problem. Unlike Salmonella or E. coli outbreaks that sometimes trace to produce or water, the vast majority of Campylobacter cases trace back to a single source: poultry, particularly chicken. Studies consistently find Campylobacter contamination on 40-80% of retail chicken in the United States and similar proportions across Europe and Australia.
The bacteria live harmlessly in the intestines of chickens and turkeys and contaminate carcasses during slaughter. They do not make the bird visibly sick or smell different. They survive refrigeration for days and are invisible to the naked eye.
The two critical prevention points are cooking temperature and cross-contamination. Campylobacter is reliably killed by cooking poultry to an internal temperature of 165°F (74°C) throughout — not just on the surface. A meat thermometer inserted into the thickest part of the breast, away from bone, is the only reliable check.
Cross-contamination occurs when raw poultry juices contact surfaces, utensils, or foods that will be eaten without further cooking — salad vegetables, bread, cooked foods. Even a tiny amount of contaminated juice can cause infection. The prevention steps are straightforward but must actually be practiced:
- Use a dedicated cutting board for raw poultry
- Wash hands thoroughly with soap after handling raw poultry
- Refrigerate poultry separately from ready-to-eat foods
- Do not rinse raw chicken (it spreads bacteria to the sink and surrounding surfaces)
- Clean and sanitize all surfaces that contacted raw poultry before using them for other foods
Other less common but real sources include unpasteurized milk, untreated water, contact with farm animals or their environment, and international travel to regions with lower food hygiene standards.
Full details on safe food handling, high-risk food categories, travel precautions, and preventing household spread are covered in: Food Safety and Prevention.
Antibiotic Stewardship
Campylobacter jejuni causes roughly 1.5 million illnesses annually in the United States, making it one of the most common foodborne bacterial pathogens in the country. If everyone with Campylobacter received antibiotics, the sheer volume of antibiotic prescriptions would be enormous — and most of them would be unnecessary, since the majority of patients recover without treatment.
Antibiotic stewardship — using antibiotics only when they genuinely improve outcomes — is not just about individual patients. It is about protecting the effectiveness of the drugs we have for the patients who genuinely need them. Every unnecessary antibiotic course creates selective pressure that favors resistant strains. The global fluoroquinolone resistance crisis in Campylobacter is itself a cautionary tale: widespread fluoroquinolone use in both human medicine and veterinary agriculture has driven resistance rates high enough that these drugs are now unreliable for treating the very illness they were once effective against.
The fluoroquinolone story is particularly stark because it implicates the agricultural sector as much as human medicine. The FDA approved fluoroquinolone use in poultry flocks in 1995; resistance rates in human Campylobacter isolates rose in parallel with veterinary use. The FDA eventually withdrew approval for fluoroquinolone use in poultry in 2005, but resistance remains entrenched because the bacteria carrying resistance genes continue to circulate.
Reserving antibiotics for patients who genuinely need them — those with severe illness, immunosuppression, bacteremia, or occupational transmission risk — is both clinically correct and socially responsible. The goal is not to deny treatment to sick people; it is to ensure that treatment is available and effective for those who truly need it, now and in the future.
Practical Guidance for High-Risk Groups
Different patients face different risks from Campylobacter infection, and the practical recommendations vary accordingly.
Healthy adults: Rest, drink ORS, avoid solid foods until nausea improves, then reintroduce bland foods gradually (rice, toast, bananas, cooked vegetables). Avoid dairy until diarrhea resolves. Watch for signs of dehydration. Seek care if fever exceeds 39°C, blood in stool is heavy, or symptoms are not improving by day 5-7.
Children under 5: Children dehydrate faster than adults and are at higher risk for serious complications. Use age-appropriate ORS (Pedialyte or equivalent) — not sports drinks or fruit juice, which have the wrong electrolyte-to-sugar ratio for small children. Seek medical attention promptly for any infant with diarrhea who appears listless, has sunken fontanelle, or is not producing tears when crying.
Elderly adults: Reduced physiological reserve means dehydration can become serious faster. Social isolation can delay recognition that someone is deteriorating. Family members checking in are important. A lower threshold for seeking medical care is appropriate.
People with HIV/AIDS or other immunodeficiencies: Campylobacter can cause recurrent or relapsing bacteremic illness in people with severe immunodeficiency. Antibiotic prophylaxis may be discussed with an infectious disease specialist. Any febrile illness should prompt early medical evaluation.
Pregnant women: Avoid unpasteurized dairy and undercooked poultry throughout pregnancy. If Campylobacter illness is suspected during pregnancy, contact an obstetrician promptly rather than managing at home. Azithromycin is considered relatively safe in pregnancy; fluoroquinolones are avoided.
Travelers to high-incidence regions: Southeast Asia, South Asia, Sub-Saharan Africa, and parts of Latin America have high Campylobacter rates. Travel food safety rules apply: eat only thoroughly cooked food, avoid raw salads and unpeeled fruit unless you peel it yourself, drink only bottled or boiled water, avoid ice. Pack oral rehydration sachets. A travel medicine consultation before departure can address antibiotic prophylaxis options for certain itineraries.
Key Research Papers
- Kaakoush NO, et al. Global epidemiology of Campylobacter infection. Clin Microbiol Rev 2015;28:687-720. — Search PubMed
- Allos BM. Campylobacter jejuni infections: update on emerging issues and trends. Clin Infect Dis 2001;32:1201-6. — Search PubMed
- Wieczorek K, Osek J. Antimicrobial resistance mechanisms among Campylobacter. Biomed Res Int 2013;2013:340605. — Search PubMed
- Engberg J, et al. Quinolone and macrolide resistance in Campylobacter jejuni and C. coli: resistance mechanisms and trends in human isolates. Emerg Infect Dis 2001;7:24-34. — Search PubMed
- Tack DM, et al. Preliminary incidence and trends of infections with pathogens transmitted commonly through food. MMWR 2020;69(17):509-14. — Search PubMed
- Nachamkin I, et al. Campylobacter species and Guillain-Barré syndrome. Clin Microbiol Rev 1998;11:555-67. PMID 9665983
- Scallan E, et al. Foodborne illness acquired in the United States — major pathogens. Emerg Infect Dis 2011;17:7-15. PMID 21192848
- Young KT, Davis LM, DiRita VJ. Campylobacter jejuni: molecular biology and pathogenesis. Nat Rev Microbiol 2007;5:665-79. — Search PubMed
- Blaser MJ. Epidemiologic and clinical features of Campylobacter jejuni infections. J Infect Dis 1997;176(Suppl 2):S103-5. — Search PubMed
- Crushell E, et al. Enteric Campylobacter: purging its secrets? Pediatr Res 2004;55:3-12. PMID 14605259
Connections
- Campylobacter Jejuni Overview
- Symptoms & Diagnosis Hub
- Diarrhea & GI Symptoms
- Guillain-Barré Syndrome
- Azithromycin & Antibiotic Treatment
- Food Safety and Prevention
- Fluoroquinolone Resistance
- Gastroenterology
- Salmonella
- All Bacteria