Campylobacteriosis: Diarrhea, Fever, and Abdominal Pain
Campylobacteriosis is one of the most common bacterial causes of foodborne gastroenteritis worldwide, responsible for an estimated 1.5 million illnesses in the United States every year. The hallmark symptoms — profuse diarrhea (often bloody), severe abdominal cramping, and fever — follow a distinctive pattern that can help distinguish Campylobacter from other gut infections. Understanding exactly how and when each symptom appears, what it feels like, and when to seek emergency care can make a significant difference in recovery. This article walks through the full symptom timeline from the earliest warning signs to full recovery.
- The Prodrome: Flu-Like Warning Signs
- Incubation Period
- Character of the Diarrhea
- Severe Abdominal Cramping
- Fever
- Nausea and Vomiting
- Duration and Recovery
- Rare Bacteremia
- Severe Dehydration: Assessment and Management
- Key Research Papers
- Connections
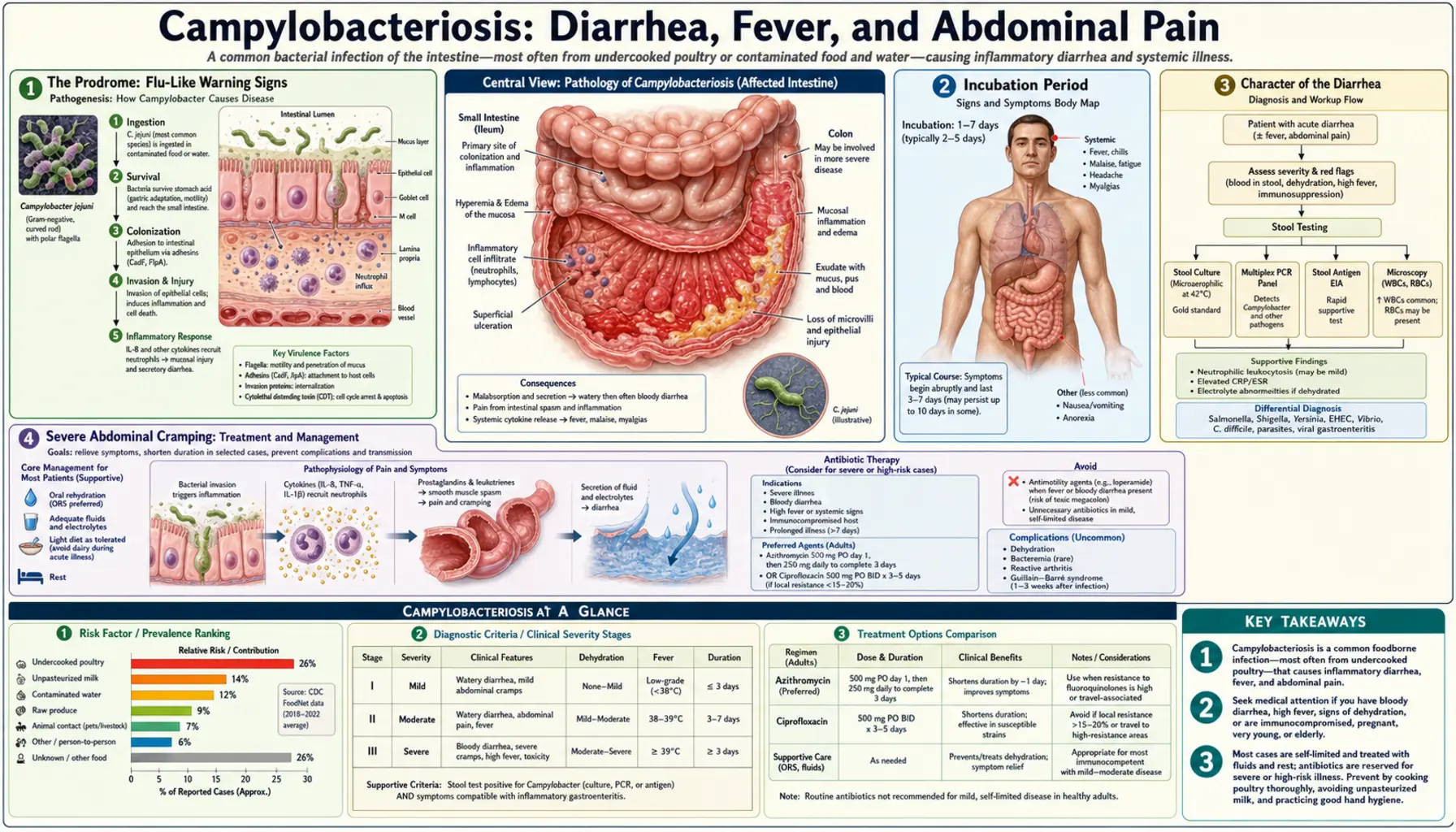
The Prodrome: Flu-Like Warning Signs
Before diarrhea begins, most people with campylobacteriosis experience a prodromal phase lasting 12 to 48 hours. During this window, the infection feels remarkably like influenza — not a stomach bug.
The prodromal symptoms include:
- Fever — temperature 38–40°C (100.4–104°F), abrupt in onset
- Myalgias — generalized muscle aches and body pain, particularly in the legs and lower back
- Headache — often throbbing, frontal
- Malaise — profound fatigue and a sense of feeling unwell before any GI symptoms develop
Two mechanisms drive this early phase. First, C. jejuni can transiently enter the bloodstream (bacteremia) even in otherwise healthy people, triggering systemic immune activation. Second, the intestinal epithelium mounts a rapid cytokine response — releasing interleukin-8 (IL-8), tumor necrosis factor-alpha (TNF-α), and interferon-gamma — before the gut itself has been visibly damaged. These circulating inflammatory signals produce every classic flu symptom.
The practical problem is obvious: someone with fever, aches, and headache 24 hours after eating undercooked chicken typically does not connect those symptoms to their meal. They rest, take acetaminophen, and are shocked when explosive diarrhea arrives the next day. Recognizing the prodrome pattern — especially in the setting of a possible exposure (restaurant meal, barbecue, travel) — allows earlier mental preparation and better fluid management before diarrhea sets in.
Incubation Period
The incubation period for Campylobacter jejuni is typically 2 to 5 days, with a range of 1 to 10 days after eating contaminated food or water. This relatively long incubation period — compared to the 1–6 hours of Staphylococcus aureus toxin illness or even the 6–48 hours of Salmonella — creates a major epidemiological complication: patients almost never correctly identify the causative meal.
By the time diarrhea begins, the responsible meal was consumed 2 to 5 days earlier. People tend to blame the most recent thing they ate — yesterday's salad or this morning's breakfast — rather than the chicken they had at a family gathering four days ago. This mismatch makes both clinical history-taking and public health outbreak investigations difficult.
The long incubation reflects C. jejuni's biology. The infectious dose is low — as few as 500 to 800 organisms can cause illness in healthy adults — but the bacteria must first colonize the small intestine and proximal colon, adhere to and invade epithelial cells, and begin producing cytolethal distending toxin (CDT) and other virulence factors before the inflammatory cascade that drives symptoms gets underway. This takes days, not hours.
In volunteer human infection studies, ingesting known doses of C. jejuni consistently produced illness at 2–5 days, confirming that the long incubation is a true biological feature of this pathogen and not just a recall bias in clinical case series.
Character of the Diarrhea
The diarrhea of campylobacteriosis has a characteristic two-phase evolution that helps clinicians distinguish it from other foodborne illnesses.
Phase 1 — Watery and Profuse (Day 1–2 of diarrhea onset): The first stools are large-volume, watery, and may contain mucus. Patients report urgency and cramping with each episode. Frequency ranges from 3 to 10 bowel movements per day, though severely ill patients may exceed this.
Phase 2 — Bloody and Inflammatory (Day 2–4): Within 1 to 2 days of diarrhea onset, stool character often changes dramatically. Frank blood — bright red, dark red, or mixed with mucus — appears in 50 to 90% of laboratory-confirmed cases in hospital-based series. Some patients describe the stool as looking like "tomato soup" or "raspberry jelly." The bloody phase marks the transition from secretory to invasive pathology, as C. jejuni penetrates the colonic mucosa and triggers a full inflammatory response.
This shift to bloody diarrhea is the key distinguishing feature that sets campylobacteriosis apart from many other common gastroenteritides. Norovirus and rotavirus almost never produce bloody stool. Clostridium perfringens and enterotoxigenic E. coli (traveler's diarrhea) are typically watery-only. Bloody diarrhea with fever narrows the differential to Campylobacter, Salmonella, Shigella, E. coli O157:H7, and Entamoeba histolytica.
Stool microscopy during the inflammatory phase shows abundant polymorphonuclear cells (PMNs, also called fecal leukocytes) — a hallmark of invasive bacterial diarrhea. A positive fecal lactoferrin or calprotectin test (which detects PMN breakdown products) is a more sensitive and specific marker of the same process and is increasingly used in outpatient settings where microscopy is unavailable.
Stool volumes are relatively small per episode — 100 to 300 mL — compared to the liter-per-hour output of cholera. The urgency and frequency are the primary burden, not massive volume losses. This matters for dehydration assessment (see below).
Severe Abdominal Cramping
Abdominal cramping is frequently described by patients as the most distressing symptom of campylobacteriosis — more painful, in many accounts, than the diarrhea itself.
The cramping has a distinctive localization: the right lower quadrant of the abdomen, in the region of the terminal ileum and cecum. This is because C. jejuni preferentially colonizes and invades the terminal ileum before spreading to the colon. The inflammation of the terminal ileum and ileocecal region produces pain that is anatomically indistinguishable from appendicitis.
The clinical consequence is significant. Emergency physicians worldwide have performed appendectomies on Campylobacter patients, only to find a normal appendix and a severely inflamed terminal ileum (terminal ileitis) — a condition sometimes called "Campylobacter pseudoappendicitis." In the pre-imaging era, misdiagnosis rates were high. Even today, right lower quadrant pain with rebound tenderness and fever in a young person can easily trigger a surgical evaluation before stool culture results are back.
Several features help distinguish Campylobacter cramping from true appendicitis:
- Cramping begins before diarrhea and is colicky (wave-like, coming and going), whereas appendicitis pain is typically constant and progressively worsens
- Diarrhea itself (especially bloody diarrhea) is highly unusual in appendicitis
- Campylobacter cramping is often diffuse initially, shifting to the right lower quadrant — appendicitis is typically right lower quadrant from the start
- Fever pattern is different: Campylobacter fever tends to be higher and earlier in the course
CT scan of the abdomen in Campylobacter pseudoappendicitis shows thickening of the terminal ileal wall and mesenteric lymphadenopathy — a pattern consistent with infectious enteritis rather than appendicitis. Clinicians with a high index of suspicion for foodborne illness in the right context can avoid unnecessary surgery with CT imaging and stool culture.
Fever
Fever is present in 50 to 90% of culture-confirmed campylobacteriosis cases, making it one of the most reliable clinical markers of this infection. Typical temperatures range from 38.0°C to 40.0°C (100.4°F to 104°F), though temperatures above 40°C are seen in severe cases, particularly in children and the elderly.
The classic clinical triad of campylobacteriosis is:
- Fever (≥38°C)
- Bloody diarrhea
- Severe abdominal cramping
This triad, when present together, is highly suggestive of an invasive bacterial enteritis and should prompt stool culture in almost all clinical settings. No other common foodborne pathogen produces all three simultaneously as reliably as Campylobacter.
The mechanism of fever is dual. In the prodromal phase (before diarrhea), fever arises from cytokine release triggered by early mucosal invasion. In the diarrheal phase, fever reflects the intense colonic inflammation driven by PMN infiltration, the release of prostaglandin E2, and — in a subset of patients — genuine transient bacteremia with circulating bacterial lipopolysaccharide (LPS) activating systemic innate immune responses.
Fever typically peaks at days 1–3 of the diarrheal illness and then begins to subside as the immune response clears the infection. Persistent high fever beyond day 5, or fever that resolves and then returns, should raise concern for complications: bacteremia, reactive arthritis, or — rarely — Guillain-Barré syndrome (GBS), which can present with fever recurrence weeks after the initial GI illness.
Using antipyretics (acetaminophen or ibuprofen) to manage fever is appropriate for comfort. There is no evidence that fever reduction in campylobacteriosis impairs bacterial clearance or prolongs illness.
Nausea and Vomiting
Nausea and vomiting are present but are considerably less prominent in campylobacteriosis than in norovirus gastroenteritis or Staphylococcus aureus food poisoning — and this relative difference is diagnostically useful.
Nausea is reported by approximately 50 to 70% of patients. Vomiting occurs in 15 to 25% — substantially lower than the 75%+ vomiting rates seen in norovirus outbreaks. When vomiting does occur, it tends to:
- Begin during the prodromal phase (before diarrhea) or at diarrhea onset
- Be mild to moderate in severity (1–3 episodes rather than continuous retching)
- Resolve within 24 to 48 hours, even as diarrhea continues
The relatively spared vomiting reflex reflects the primary site of C. jejuni pathology. This bacterium predominantly infects the small intestine and colon — not the stomach. Vigorous vomiting is typically driven by gastric involvement or by toxins that act on the chemoreceptor trigger zone (CTZ) in the brainstem, as with staph toxin. C. jejuni produces no emetic toxin acting on the CTZ.
Practically, the pattern of nausea-without-much-vomiting combined with severe cramping, bloody diarrhea, and fever points strongly toward a colonic invasive pathogen rather than a "stomach flu." Patients who are vomiting profusely and have minimal diarrhea more likely have norovirus, staph food poisoning, or bacillus cereus emetic syndrome.
For patients who do vomit, the priority is protecting hydration. Even brief vomiting episodes can significantly impair oral rehydration if the patient cannot keep fluids down. Small sips of oral rehydration solution every 5 to 10 minutes — rather than drinking large volumes — is more likely to stay down.
Duration and Recovery
The typical course of uncomplicated campylobacteriosis in a healthy adult is 3 to 7 days. Understanding the phased recovery timeline helps patients know what to expect and when improvement is off-schedule.
Days 1–3 (Acute Peak): This is the most symptomatic period. Fever is highest, diarrhea frequency peaks (up to 10 or more episodes per day), bloody stools are most prominent, and cramping is most severe. Most patients feel severely unwell and may require time off work or school.
Days 3–5 (Plateau and Early Improvement): Fever typically begins to break. Diarrhea frequency decreases. Bloody stools begin to clear before watery stools fully resolve — the bleeding stops before the bowel returns to normal. Cramping lessens in intensity. Nausea usually resolves completely during this phase.
Days 5–7 (Recovery): Most healthy adults are functionally recovered by day 7. Stool consistency normalizes. Energy begins to return. Some patients notice that their stools remain loose or slightly more frequent than baseline for a few additional days — this is normal and does not indicate treatment failure or relapse.
Post-Illness Fatigue (Weeks 1–2): A significant minority of patients report persistent fatigue lasting 1 to 2 weeks after clinical resolution of diarrhea. This post-infectious fatigue is well-recognized and appears to relate to immune activation rather than ongoing bacterial infection. Campylobacter is cleared from the stool by the time fatigue peaks in this post-illness window. Rest and gradual return to normal activity is the appropriate management.
Prolonged Illness in Immunocompromised Patients: Patients with HIV/AIDS, hematologic malignancies, organ transplants, or on long-term corticosteroids can have campylobacteriosis lasting weeks to months. In these patients, the infection may relapse after apparent recovery, particularly if antibiotic treatment is not given. Stool cultures should be repeated in any immunocompromised patient with recurrent diarrhea.
Relapse in healthy adults is uncommon (less than 5%) but can occur, particularly if the patient had a brief or incomplete antibiotic course, was re-exposed to the same contaminated source, or has subtle immune dysfunction. A second episode of diarrhea with the same characteristics 1 to 2 weeks after apparent recovery should prompt repeat stool culture.
Rare Bacteremia
Bloodstream invasion — bacteremia — is an uncommon but serious complication of C. jejuni infection, occurring in fewer than 1% of immunocompetent hosts. The rate rises substantially in people with conditions that impair host defenses.
High-Risk Groups for Bacteremia:
- Adults over 65 years old
- People living with HIV/AIDS (especially with CD4 count below 200 cells/µL)
- Individuals with liver disease (cirrhosis, hepatic failure)
- Those with hematologic malignancy (leukemia, lymphoma) or solid tumors
- Recipients of immunosuppressive therapy (chemotherapy, corticosteroids, biologic agents)
- People with hypogammaglobulinemia or complement deficiency
- Infants under 6 months old
Which Species is More Dangerous: It is worth noting that Campylobacter fetus — a less common species than C. jejuni — is disproportionately responsible for bacteremia and extra-intestinal infections. C. fetus has a surface protein layer (S-layer) that resists complement-mediated killing, making it particularly adept at surviving in the bloodstream. In bacteremic Campylobacter cases in elderly or immunocompromised patients, C. fetus is often the culprit even though it is far less common as a cause of routine gastroenteritis.
Clinical Presentation of Bacteremia: The presentation of Campylobacter bacteremia is often deceptive. Rather than diarrhea, the predominant symptom is fever — sometimes high and spiking — without prominent gastrointestinal complaints. The GI symptoms may be mild or absent entirely, shifting clinical suspicion away from a foodborne pathogen. Blood cultures are positive; stool cultures may be negative. This presentation is sometimes described as a "Campylobacter fever of unknown origin."
Serious Complications of Bacteremia:
- Mycotic (infectious) aneurysm — rare but life-threatening; Campylobacter seeding of atherosclerotic plaques in the aorta or its branches; presents as abdominal or back pain, pulsatile abdominal mass; high mortality without rapid surgical intervention
- Septic thrombophlebitis — infected clots in veins, particularly mesenteric or hepatic veins
- Meningitis — rare; predominantly in neonates and severely immunocompromised adults
- Septic arthritis — purulent joint infection; distinct from the more common reactive arthritis (which is sterile)
- Endocarditis — extremely rare; reported in patients with underlying valvular disease
Outcomes: Mortality from Campylobacter bacteremia ranges from 10 to 15% in reported case series, concentrated entirely in the high-risk groups above. In healthy adults under 65 without immune compromise, bacteremia is so rare that mortality attributable to it is effectively zero. Prompt diagnosis with blood cultures and appropriate antibiotic therapy (azithromycin or a carbapenem for severely ill patients) is essential for survival in at-risk individuals.
Severe Dehydration: Assessment and Management
Dehydration is the most common serious complication of campylobacteriosis across all age groups. Although individual stool volumes are relatively modest (unlike cholera), frequent episodes over days combined with reduced oral intake can produce clinically significant fluid and electrolyte depletion.
Assessing Dehydration at Home: Practical signs that dehydration is worsening and medical attention may be needed:
- Urine is dark yellow, amber, or you have not urinated in 8+ hours
- Dry mouth and lips that do not improve with drinking small amounts of water
- Dizziness or lightheadedness when standing up (orthostatic hypotension)
- Rapid heart rate felt at rest (heart "pounding")
- Sunken eyes or skin that does not snap back quickly when pinched
- In infants: sunken fontanelle (soft spot), no tears when crying, no wet diapers for 6+ hours
Oral Rehydration Salts (ORS): ORS is the first-line management for mild-to-moderate dehydration from campylobacteriosis. ORS works better than plain water because the glucose-sodium cotransport mechanism in gut enterocytes remains functional even during bacterial diarrhea — glucose actively pulls sodium (and water) across the intestinal lining even when secretory pathways are disrupted. Plain water lacks this co-transport mechanism and is less effective at rehydrating the gut.
Commercial ORS packets (Pedialyte, Normalyte, WHO ORS formula) are appropriate for all ages. Coconut water and sports drinks have too little sodium and too much sugar for severely dehydrated individuals — they are acceptable for mild dehydration. Soda and juice should be avoided because high osmolality can worsen diarrhea.
Practical ORS strategy: sip 2–4 ounces every 10–15 minutes rather than drinking large volumes at once. Large volumes trigger the gastrocolic reflex and can worsen cramping. Consistency matters more than speed.
When to Go to the Hospital for IV Fluids:
- Cannot keep any liquids down due to vomiting lasting more than 24 hours
- Signs of severe dehydration: very rapid heart rate, confusion or lethargy, minimal or no urination over 12 hours, blood pressure drop on standing
- High fever (above 39.5°C / 103°F) that is not responding to acetaminophen
- Bloody diarrhea and fever in an infant under 12 months (emergency)
- Any diarrheal illness in a patient with chronic kidney disease, heart failure, or on diuretics — electrolyte imbalances can be severe and rapid in these groups
- Elderly patients (over 75) who appear confused or very weak — age impairs the thirst mechanism and physiologic compensation for dehydration
In hospital, IV normal saline or lactated Ringer's solution is used for rapid rehydration. Electrolyte panels guide correction of hyponatremia, hypokalemia (low potassium from diarrheal losses), and metabolic alkalosis. Most patients requiring IV fluids improve rapidly and are discharged within 24 to 48 hours once oral intake is tolerated.
Key Research Papers
- Blaser MJ, Berkowitz ID, LaForce FM, Cravens J, Reller LB, Wang WL. Campylobacter enteritis: clinical and epidemiologic features. Ann Intern Med. 1979;91:179-185. — Search PubMed
- Blaser MJ, Wells JG, Feldman RA, Pollard RA, Allen JR. Campylobacter enteritis in the United States. A multicenter study. Ann Intern Med. 1983;98:360-368. — Search PubMed
- Skirrow MB. Campylobacter enteritis: a "new" disease. Br Med J. 1977;2:9-11. PMID 871765
- Ketley JM. Pathogenesis of enteric infection by Campylobacter. Microbiology. 1997;143:5-21. — Search PubMed
- Black RE, Levine MM, Clements ML, Hughes TP, Blaser MJ. Experimental Campylobacter jejuni infection in humans. J Infect Dis. 1988;157:472-479. — Search PubMed
- Kaakoush NO, Castaño-Rodríguez N, Mitchell HM, Man SM. Global epidemiology of Campylobacter infection. Clin Microbiol Rev. 2015;28:687-720. — Search PubMed
- Young KT, Davis LM, DiRita VJ. Campylobacter jejuni: molecular biology and pathogenesis. Nat Rev Microbiol. 2007;5:665-679. — Search PubMed
- Crushell E, Harty S, Sharif F, Bourke B. Enteric Campylobacter: purging its secrets? Pediatr Res. 2004;55:3-12. PMID 14605259
- Blaser MJ, Cravens J, Powers BW, Wang WL. Campylobacter enteritis associated with canine infection. Lancet. 1978;2:979-981. PMID 82205
- Blaser MJ, Glass RI, Huq MI, Stoll B, Kibrya GM, Alim AR. Isolation of Campylobacter fetus subsp. jejuni from Bangladeshi children. J Clin Microbiol. 1980;12:744-747. — Search PubMed
- Pai CH, Sorger S, Lafleur L, Lackman L, Marks MI. Campylobacter gastroenteritis in children. J Pediatr. 1979;94:589-591. — Search PubMed
- Scallan E, Hoekstra RM, Angulo FJ, et al. Foodborne illness acquired in the United States — major pathogens. Emerg Infect Dis. 2011;17:7-15. PMID 21192848
Connections
- All Bacteria
- Campylobacter Jejuni — Main Overview
- Campylobacter Symptoms & Diagnosis Hub
- Guillain-Barré Syndrome and Complications
- Diagnosis: Stool Culture and PCR
- Campylobacter Treatments & Prevention Hub
- Azithromycin and Antibiotic Treatment
- Food Safety and Prevention
- Fluoroquinolone Resistance
- Gastroenterology — Disease Category