Campylobacter Treatment: Azithromycin and Antibiotic Options
- Why Most Cases Don't Need Antibiotics
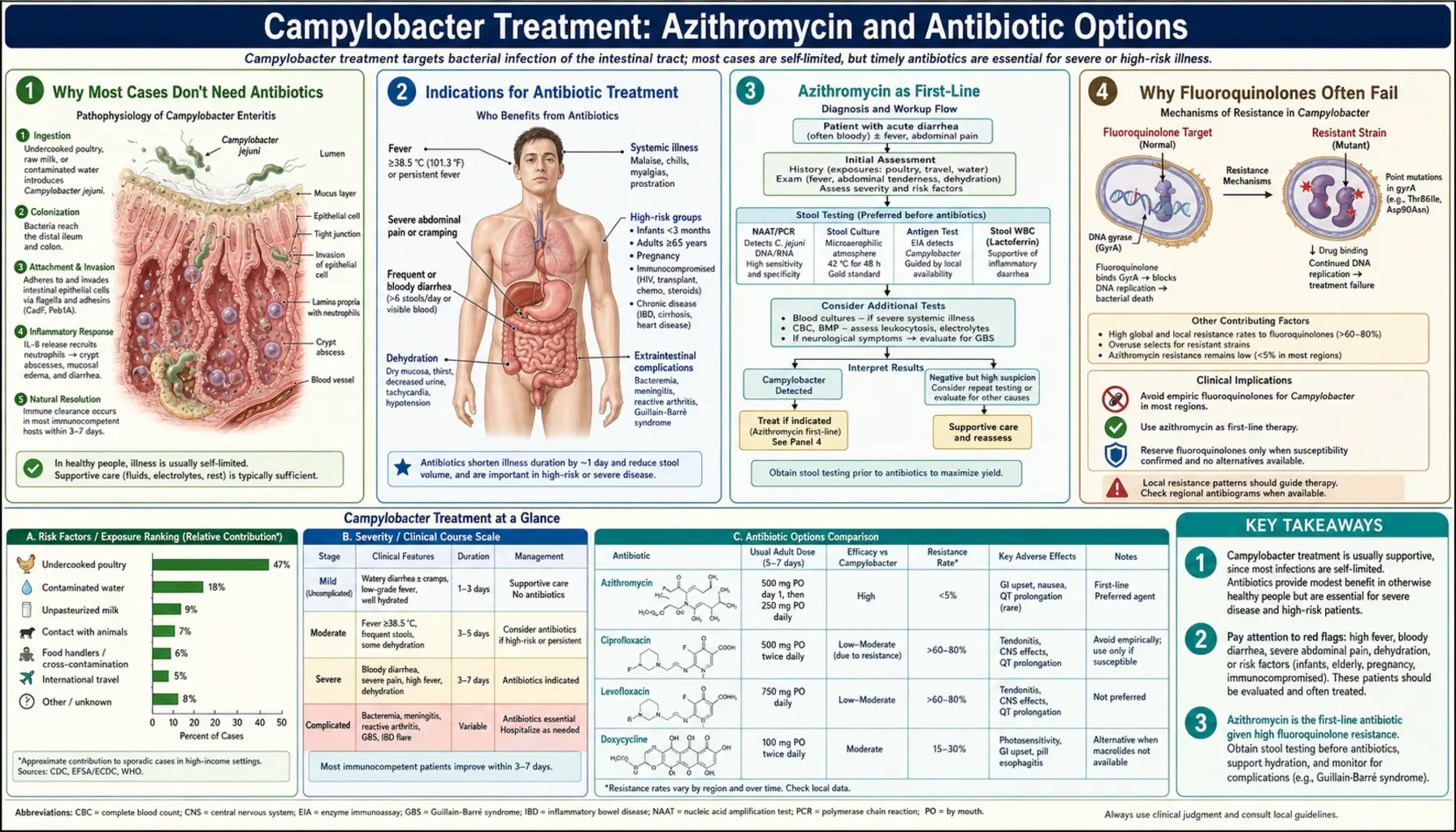
- Indications for Antibiotic Treatment
- Azithromycin as First-Line
- Why Fluoroquinolones Often Fail
- Treatment Duration
- Gentamicin and Carbapenem for Invasive Disease
- Oral Rehydration Therapy
- What Not to Take
- Key Research Papers
- Connections
Why Most Cases Don't Need Antibiotics
Campylobacter jejuni infection is self-limiting in the vast majority of otherwise healthy adults. The immune system clears the infection without any antimicrobial help, typically within 5 to 10 days. A landmark meta-analysis by Ternhag and colleagues (2007) found that antibiotics shorten illness duration by only about 1.3 days on average — a modest gain that has to be weighed against real costs: antibiotic side effects (diarrhea, nausea, rash, Clostridioides difficile risk), out-of-pocket expense, and the population-level harm of accelerating resistance.
There is also a practical timing problem. Stool culture takes 48 to 72 hours to return a positive result, and PCR panels take 24 to 48 hours. By the time a confirmed Campylobacter result lands in a doctor's inbox, most patients have already passed the peak of illness and are improving on their own. Starting antibiotics at that point provides little clinical benefit and still carries all the downside risks.
Current guidance from the Infectious Diseases Society of America (IDSA) and the European Centre for Disease Prevention and Control (ECDC) both recommend against routine antibiotic treatment for uncomplicated Campylobacter gastroenteritis. The priority in straightforward cases is supportive care: fluids, rest, and time.
Indications for Antibiotic Treatment
Certain patients genuinely need antibiotics, and recognizing those situations is just as important as avoiding unnecessary prescriptions in others. The following clinical scenarios warrant treatment:
- High fever (>39°C / 102.2°F) — suggests a more aggressive or invasive infection
- Bloody diarrhea persisting beyond one week — prolonged mucosal damage or invasive spread
- Signs of dehydration requiring hospital admission — IV antibiotics may be added alongside IV fluids
- Bacteremia (positive blood culture) — organism has left the gut; systemic treatment is mandatory
- Immunocompromised host — HIV/AIDS, solid-organ transplant, hematologic malignancy, high-dose corticosteroids, biologic therapies, or surgical splenectomy all impair the T-cell and macrophage responses needed to clear Campylobacter; these patients face prolonged infection, relapse, and bacteremia
- Very young infants (<3 months) — immature immune defenses and risk of rapid deterioration
- Elderly patients with severe symptoms — age-related immune decline and higher dehydration risk
- Pregnancy — maternal bacteremia can seed the placenta and cause premature labor, neonatal sepsis, or stillbirth
- Healthcare workers and food handlers — shortening the duration of fecal shedding matters when others are at risk; treatment reduces infectious period from a median of 2–4 weeks to several days
If you fall into any of these categories and have confirmed or strongly suspected Campylobacter infection, discuss antibiotic treatment with your doctor promptly — don't wait for the stool culture to come back if clinical suspicion is high.
Azithromycin as First-Line
When antibiotics are genuinely needed for Campylobacter jejuni, azithromycin is the first choice in most international guidelines. It belongs to the macrolide class — the same family as erythromycin and clarithromycin — and works by binding to the 50S ribosomal subunit, blocking bacterial protein synthesis.
Adult Dosing
- Standard course: 500 mg once daily for 3 days
- Alternative single-dose: 1 g (1000 mg) as a one-time dose (used in some resource-limited settings or when compliance is a concern)
- Severe or immunocompromised: some guidelines extend to 5 days or switch to IV erythromycin
Pediatric Dosing
- 10 mg/kg once daily for 3 days (maximum 500 mg/day)
- Well-tolerated in children; azithromycin suspension is available for young children who cannot swallow tablets
Why Azithromycin Works Better Than Alternatives
Azithromycin has two pharmacological advantages for gut infections. First, it concentrates inside tissue and macrophages at levels 10- to 100-fold above serum — important because Campylobacter invades the intestinal mucosa and survives inside host cells. Second, macrolide resistance in C. jejuni remains relatively low in many countries: 5–10% in most of Northern Europe and North America, though rising in some regions. This contrasts sharply with fluoroquinolone resistance, which has blown past 50% in much of the world.
Azithromycin's long half-life (68 hours) means once-daily dosing is sufficient and tissue levels stay therapeutic for days after the last dose. Side effects are generally mild: nausea, loose stools, and abdominal cramping are the most common; rare but serious cardiac effects (QT prolongation) exist but are uncommon at standard doses in otherwise healthy people.
Why Fluoroquinolones Often Fail
Until the late 1990s, ciprofloxacin was the default first-line antibiotic for Campylobacter — and in the test tube it looks excellent: low minimum inhibitory concentrations (MICs), good GI penetration, broad spectrum. In practice, empiric ciprofloxacin treatment for Campylobacter now fails roughly half the time in high-income countries and more than three-quarters of the time in some parts of Asia and the Middle East.
The Resistance Numbers
- European Union average fluoroquinolone resistance in C. jejuni: approximately 58–62% (ECDC surveillance data, 2019–2022)
- United States: approximately 25–30% by CDC National Antimicrobial Resistance Monitoring System (NARMS) — lower than Europe but rising steadily
- Southeast Asia, China, India: commonly >70–80%
- Even at 25% resistance, empiric ciprofloxacin means 1 in 4 patients gets an antibiotic that won't work
The Mechanism
The dominant resistance mechanism is a single point mutation at codon 86 of the gyrA gene (the quinolone resistance-determining region, QRDR), converting threonine to isoleucine (Thr-86-Ile). This mutation changes the DNA gyrase enzyme so that fluoroquinolones can no longer bind tightly to their target. The mutation arises readily and confers high-level resistance (MIC jumps from <0.5 mg/L to >32 mg/L in one step). There is no intermediate-susceptibility category — organisms are either fully susceptible or fully resistant.
What This Means in Practice
Do not use ciprofloxacin or other fluoroquinolones (levofloxacin, moxifloxacin) empirically for Campylobacter without recent local susceptibility data or individual susceptibility results. If susceptibility testing confirms sensitivity, ciprofloxacin remains effective and is a reasonable choice. The resistance crisis is directly linked to fluoroquinolone use in poultry production — a story covered in detail in the Antibiotic Resistance sub-article.
Treatment Duration
The length of antibiotic treatment depends on the clinical scenario:
- Uncomplicated gastroenteritis in a healthy adult: 3 days of azithromycin is the standard. Some guidelines allow a single 1 g dose.
- Severe illness or immunocompromised patients: 5 days of azithromycin; some clinicians extend to 7 days for very immunosuppressed patients.
- Bacteremia: typically 14 days of IV or oral therapy, depending on organism, source control, and clinical response. Gentamicin IV is used for hospitalized patients who cannot take oral medication.
- Relapsing infection in HIV: some patients require prolonged suppressive therapy; this is less of an issue with modern antiretroviral therapy but still encountered.
Test of Cure — Not Needed
Routine follow-up stool cultures after treatment are not recommended. Campylobacter is commonly shed asymptomatically in stool for 2 to 4 weeks after clinical recovery — even after effective antibiotic treatment. A positive stool culture at day 10 does not mean treatment failed; it just means the organism is still being cleared. Repeat testing is appropriate only if symptoms return, persist unexpectedly, or the patient is a food handler or healthcare worker subject to return-to-work policies.
Gentamicin and Carbapenem for Invasive Disease
Most people with Campylobacter never need IV antibiotics, but a subset of patients — particularly the immunocompromised and the very ill — develop bacteremia or focal infections (endovascular infection, cholecystitis, meningitis in neonates) that require parenteral therapy.
Gentamicin
Gentamicin, an aminoglycoside, is the IV antibiotic of choice for hospitalized Campylobacter bacteremia when oral therapy is not feasible. It is active against both fluoroquinolone-resistant and fluoroquinolone-susceptible strains, making it valuable precisely because you often don't know the resistance pattern when a patient is critically ill. Standard dosing uses extended-interval (once-daily) dosing to maximize the concentration-dependent killing while minimizing nephrotoxicity. Renal function must be monitored closely.
Carbapenems
Imipenem-cilastatin and meropenem are broad-spectrum beta-lactams used for severe invasive disease or when first-line agents fail. C. jejuni carries beta-lactamases that make it resistant to many penicillins, but carbapenems remain reliably active. These are reserved for life-threatening situations given their cost, side effects, and the importance of preserving carbapenem activity against other organisms.
Campylobacter fetus — A Different Species
C. fetus (distinct from C. jejuni) causes bacteremia in immunocompromised and elderly patients. It is less common in the gut but more likely to seed the bloodstream and cause endovascular infections. Fortunately, C. fetus is typically susceptible to ampicillin, amoxicillin-clavulanate, gentamicin, and imipenem. Treatment is usually 2 weeks minimum for bacteremia, longer for endovascular disease.
Oral Rehydration Therapy
Fluid replacement is the cornerstone of Campylobacter treatment regardless of whether antibiotics are needed. Diarrhea causes rapid losses of water, sodium, potassium, and bicarbonate. For most people, oral rehydration is safe, effective, and far preferable to IV fluids — provided the patient can drink and keep fluids down.
The WHO ORS Formula
The World Health Organization's oral rehydration solution (ORS) is the gold standard, designed around the sodium-glucose co-transport mechanism in the intestinal wall. Even in active diarrhea, this co-transport system works well — sipping ORS is absorbed even when plain water is not retained. The WHO low-osmolarity formula (2002) contains:
- Sodium: 75 mmol/L
- Potassium: 20 mmol/L
- Chloride: 65 mmol/L
- Citrate: 10 mmol/L (bicarbonate equivalent for acidosis)
- Glucose: 75 mmol/L
- Total osmolarity: 245 mOsm/L
Commercial products: Pedialyte (US), Gastrolyte (Australia/UK), Dioralyte (UK), WHO ORS sachets (developing world). Sports drinks like Gatorade are not equivalent — they are much higher in sugar and lower in sodium and potassium than clinical ORS.
How Much to Drink
- Adults: 200–400 mL of ORS after each loose stool, plus enough to quench thirst
- Children: 10 mL/kg after each loose stool (approximately half a cup for a toddler)
- General rule: drink more than you're losing
When IV Fluids Are Needed
Seek emergency care if you: cannot keep any fluid down due to vomiting, have signs of severe dehydration (dizziness on standing, very dark urine or none at all, confusion), or have lost more than 10% of body weight from fluid loss. Hospitalization for IV normal saline or Ringer's lactate is appropriate in these cases.
What Not to Take
Several commonly used over-the-counter medications are either harmful or unhelpful in Campylobacter infection. Knowing what to avoid is as important as knowing what to take.
Loperamide (Imodium) — Avoid in Bloody Diarrhea
Loperamide slows intestinal motility, which sounds desirable when you have diarrhea. In non-invasive secretory diarrhea (like traveler's diarrhea caused by ETEC), it provides real symptom relief. But in invasive bacterial infections like Campylobacter, stopping gut movement traps the bacteria and their toxins in contact with the intestinal wall for longer, worsening mucosal damage. More dangerously, impaired motility may facilitate bacterial spread across the gut wall into the bloodstream. The rule: if there is any blood in the stool, do not use loperamide. If you are unsure whether your infection is invasive, contact a doctor before taking it.
Anti-Emetics — Generally Safe
Ondansetron (Zofran), promethazine, and similar anti-emetics are generally safe in Campylobacter illness if vomiting is preventing you from keeping fluids down. They do not worsen the infection. Use short-term as needed.
NSAIDs — Use With Caution
Ibuprofen and naproxen can reduce fever and relieve the significant abdominal cramping of Campylobacter infection, but they also reduce prostaglandin-mediated gut mucosal protection and can impair renal blood flow in someone already dehydrated. If you're going to use them, take with food and drink extra fluids. Acetaminophen (paracetamol) is a safer choice for fever and pain in the context of active GI illness.
Antibiotics Without Clear Indication
Taking antibiotics that aren't needed is not a neutral act. Unnecessary antibiotic exposure kills commensal gut bacteria that normally compete with resistant organisms, leaving you temporarily more vulnerable to C. difficile and resistant-organism colonization. At the population level, unnecessary prescriptions drive the resistance crisis that has already rendered ciprofloxacin unreliable against Campylobacter in much of the world. If your doctor says you don't need antibiotics, that is a medically sound and responsible recommendation.
Key Research Papers
- Ternhag A, Asikainen T, Giesecke J, Ekdahl K. Short- and long-term effects of bacterial gastrointestinal infections. Emerg Infect Dis. 2008;14(1):143–8. — Search PubMed — Meta-analysis establishing the 1.3-day average benefit of antibiotics in bacterial gastroenteritis.
- Engberg J, Aarestrup FM, Taylor DE, Gerner-Smidt P, Nachamkin I. Quinolone and macrolide resistance in Campylobacter jejuni and C. coli: resistance mechanisms and trends in human isolates. Emerg Infect Dis. 2001;7(1):24–34. — Search PubMed — Seminal review of gyrA Thr-86-Ile mutation and macrolide resistance mechanisms.
- Allos BM. Campylobacter jejuni infections: update on emerging issues and trends. Clin Infect Dis. 2001;32(8):1201–6. — Search PubMed — Clinical overview of Campylobacter epidemiology, treatment, and complications including GBS.
- Wieczorek K, Osek J. Antimicrobial resistance mechanisms among Campylobacter. Biomed Res Int. 2013;2013:340605. — Search PubMed — Comprehensive review of resistance genes, mechanisms, and surveillance data across species.
- Kaakoush NO, Castaño-Rodríguez N, Mitchell HM, Man SM. Global epidemiology of Campylobacter infection. Clin Microbiol Rev. 2015;28(3):687–720. — Search PubMed — Global burden, risk factors, and geographic variation in antibiotic resistance rates.
- Gupta A, Nelson JM, Barrett TJ, et al. Antimicrobial resistance among Campylobacter strains, United States, 1997–2001. Emerg Infect Dis. 2004;10(6):1102–9. — Search PubMed — NARMS data showing the trajectory of fluoroquinolone resistance in the US food supply.
- Smith KE, Besser JM, Hedberg CW, et al. Quinolone-resistant Campylobacter jejuni infections in Minnesota, 1992–1998: investigation of patient risk factors and sources. N Engl J Med. 1999;340(20):1525–32. — Search PubMed — Landmark epidemiological study linking fluoroquinolone-resistant Campylobacter directly to poultry consumption.
- van Boeckel TP, Gandra S, Ashok A, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis. 2014;14(8):742–50. PMID 25022435 — Context for global antibiotic consumption driving resistance across bacterial pathogens.
- Luber P. Cross-contamination versus undercooking of poultry meat or eggs — which risks more Campylobacterioses or Salmonelloses? Int J Food Microbiol. 2009;129(3):257–62. — Search PubMed — Quantitative risk assessment of kitchen transmission routes relevant to prevention.
- Scallan E, Hoekstra RM, Angulo FJ, et al. Foodborne illness acquired in the United States — major pathogens. Emerg Infect Dis. 2011;17(1):7–15. PMID 21192848 — CDC burden-of-illness estimate placing Campylobacter among the most common US foodborne pathogens.
PubMed Topic Searches
- Campylobacter jejuni azithromycin treatment
- Campylobacter fluoroquinolone resistance
- Campylobacter bacteremia antibiotics
- Oral rehydration therapy gastroenteritis
- Loperamide invasive diarrhea risk
Connections
- Campylobacter Jejuni — Main Page
- Treatment & Prevention Hub
- Diarrhea & GI Symptoms
- Diagnosis: Stool Culture and PCR
- Food Safety and Prevention
- Fluoroquinolone Resistance
- Guillain-Barré Syndrome and Complications
- Gastroenterology
- All Bacteria