Phenylalanine for Skin Pigmentation and Vitiligo
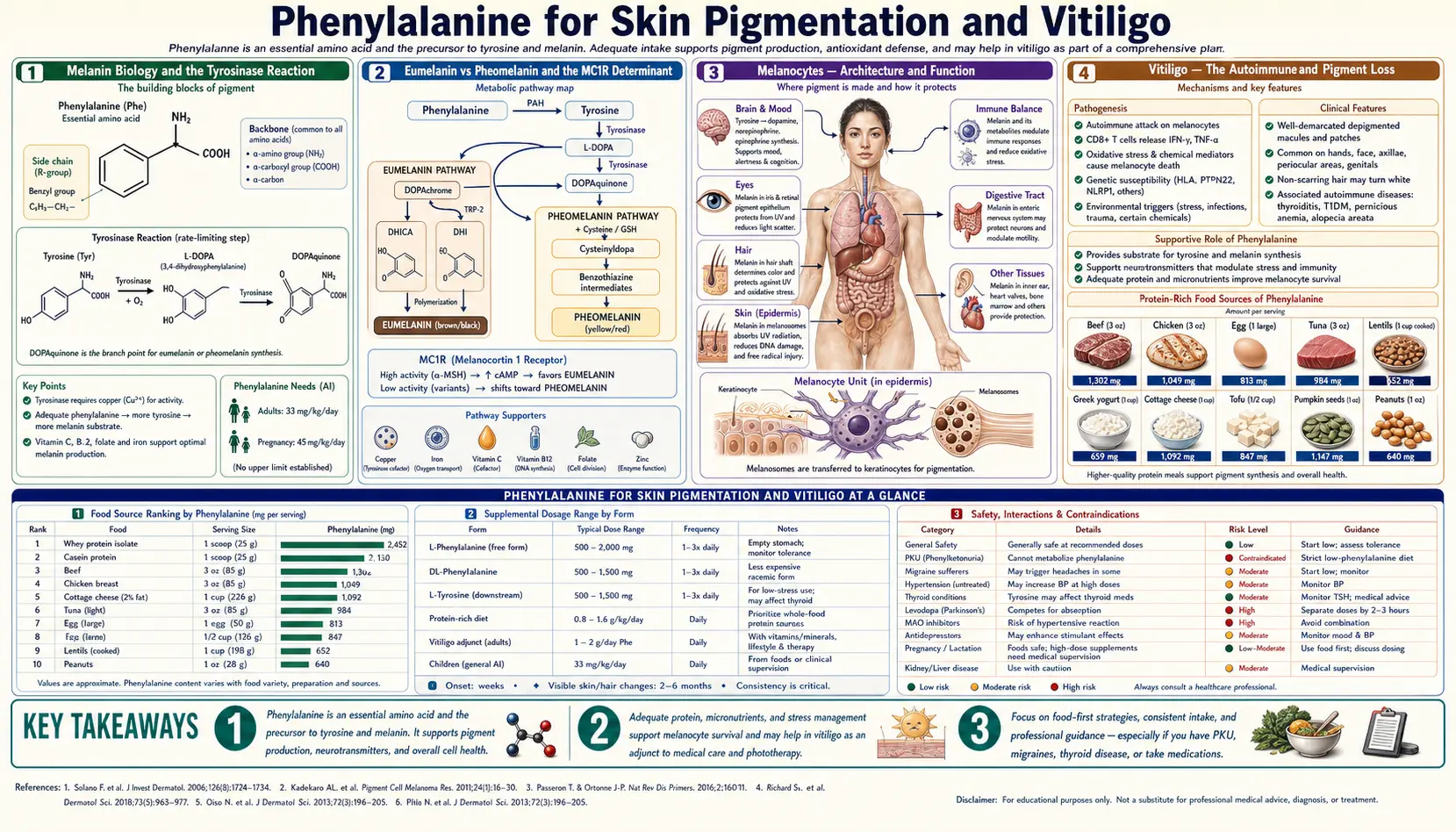
The same biochemical pathway that converts phenylalanine to tyrosine to L-DOPA also delivers the substrate for melanin — the pigment that gives skin, hair, and eyes their color and that protects the genome of every superficial skin cell from ultraviolet damage. In specialized melanocyte cells of the epidermis, tyrosine is oxidized by the copper-dependent enzyme tyrosinase to form DOPA and then dopaquinone, which polymerizes through a complex series of reactions into eumelanin (brown-black) or pheomelanin (red-yellow). When this pathway fails locally — as it does in the autoimmune disease vitiligo, where melanocytes are destroyed by the patient's own immune system — supplying additional substrate can support the survival and re-pigmentation activity of remaining melanocytes. The Cormane 1985 trial and the Antoniou 1989 trial established that oral phenylalanine combined with ultraviolet A (UVA) exposure can produce measurable repigmentation in vitiligo patients, particularly in early disease and on face and trunk locations. The mechanism, evidence, and practical protocols are the subject of this deep-dive.
Table of Contents
- Melanin Biology and the Tyrosinase Reaction
- Eumelanin vs Pheomelanin and the MC1R Determinant
- Melanocytes — Architecture and Function
- Vitiligo — The Autoimmune Pigment Loss
- The Cormane 1985 Trial
- The Antoniou 1989 Trial with UVA
- Oral vs Topical Phenylalanine Protocols
- Response Patterns and Patient Selection
- Comparison to Khellin (KUVA) Therapy
- Comparison to Tacrolimus and Calcineurin Inhibitors
- Combination Protocols and Adjunct Nutrients
- PKU and the Lighter Pigmentation Connection
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Melanin Biology and the Tyrosinase Reaction
Melanin is the principal pigment of human skin, hair, and the iris of the eye. It absorbs ultraviolet radiation across a broad spectrum, dissipates the absorbed energy as heat, scavenges reactive oxygen species, and provides physical protection to the genome of underlying keratinocyte stem cells. Without adequate melanin, skin is vulnerable to UV-induced DNA damage, sunburn, accelerated photoaging, and dramatically increased risk of skin cancer including melanoma.
The biosynthesis of melanin begins with tyrosine. The first and rate-limiting step is performed by tyrosinase (EC 1.14.18.1), a copper-containing enzyme that catalyzes two sequential reactions:
- Tyrosine + O2 → L-DOPA (3,4-dihydroxyphenylalanine). The hydroxylation of tyrosine, requiring molecular oxygen and the two copper atoms at the tyrosinase active site.
- L-DOPA + O2 → dopaquinone. The further oxidation of L-DOPA to a reactive quinone.
Dopaquinone is then routed through one of two divergent pathways depending on the local cellular environment:
- In the absence of sulfur-containing cofactors (cysteine, glutathione), dopaquinone undergoes intramolecular cyclization to form dopachrome, which is further processed via DHICA and DHI intermediates and ultimately polymerized into eumelanin, the brown-black pigment
- In the presence of cysteine or glutathione, dopaquinone reacts to form cysteinyldopa, which is further processed into pheomelanin, the red-yellow pigment
The same precursor pathway that supplies dopamine and the catecholamines also supplies melanin. The branch point is tissue-specific: in catecholamine-producing neurons, the L-DOPA produced by tyrosine hydroxylase is decarboxylated to dopamine by aromatic L-amino acid decarboxylase. In melanocytes, the L-DOPA produced by tyrosinase is oxidized to dopaquinone and polymerized to melanin. The phenylalanine and tyrosine that feed both pathways are the same dietary pool.
Eumelanin vs Pheomelanin and the MC1R Determinant
Human skin and hair color is determined principally by the ratio of eumelanin to pheomelanin. Eumelanin dominates in dark skin and dark hair; pheomelanin dominates in fair skin and red hair. The mixture is determined by the activity of the melanocortin 1 receptor (MC1R) on the melanocyte surface, which is activated by alpha-melanocyte-stimulating hormone (alpha-MSH).
The relationships are:
- High MC1R activity (functional receptor + adequate alpha-MSH stimulation) — promotes eumelanin synthesis. Dark skin, dark hair, robust tanning response, low pheomelanin, low skin cancer risk per UV dose
- Low MC1R activity (loss-of-function MC1R variants common in northern European populations) — promotes pheomelanin synthesis. Fair skin, red or blond hair, poor tanning response, high pheomelanin, increased skin cancer risk per UV dose
The clinical relevance for phenylalanine supplementation: increasing substrate availability does not change the eumelanin/pheomelanin ratio. A patient with low MC1R activity who responds to phenylalanine supplementation produces more pheomelanin, not more eumelanin. The protective effect against UV damage is therefore better in patients with functional MC1R who can route the additional substrate to eumelanin. This explains some of the inter-patient variability in vitiligo treatment response — patients with darker constitutive skin tone tend to respond better to phenylalanine + UVA repigmentation protocols than patients with very fair skin and red hair phenotype.
Melanocytes — Architecture and Function
Melanocytes are the specialized dendritic cells of the basal epidermis that produce melanin. They constitute approximately 5 to 10 percent of basal epidermal cells. Each melanocyte projects long dendritic processes that contact approximately 36 surrounding keratinocytes, forming the "epidermal melanin unit." Melanin synthesized within the melanocyte's melanosome organelles is packaged and transferred to the surrounding keratinocytes through a phagocytic process, ultimately positioning the melanin granules over the nuclei of the keratinocytes to shield the keratinocyte DNA from UV damage.
Melanocytes are unusual cells in several ways relevant to vitiligo:
- They are derived from the neural crest in embryologic development, migrating to the skin during the first trimester. This shared neural-crest origin explains some of the immunologic cross-reactivity between melanocytes and other neural-crest derivatives
- They produce reactive oxygen species as a byproduct of melanin synthesis. The same pathway that produces protective pigment also generates intracellular oxidative stress, making melanocytes particularly dependent on antioxidant defense systems
- They express tyrosinase and several other proteins (tyrosinase-related protein 1 and 2, MITF, gp100) that are recognized as autoantigens in vitiligo and in melanoma immunotherapy
- They are relatively rare and have limited regenerative capacity in adult skin, which is why pigment loss is often persistent and slow to reverse
The reservoir of melanocyte precursors that can repopulate depigmented areas comes from two sources: the outer root sheath of hair follicles (the principal source for most skin) and migratory melanoblasts from immediately adjacent normally-pigmented skin. The hair follicle reservoir explains the perifollicular pattern of repigmentation that is the typical clinical sign of successful vitiligo treatment — pigment spots appear first around hair follicles and gradually coalesce.
Vitiligo — The Autoimmune Pigment Loss
Vitiligo is an acquired depigmentation disorder affecting approximately 1 percent of the global population. It is characterized by patches of complete pigment loss in previously normally-pigmented skin, typically appearing in young adulthood, often initially on sun-exposed areas (face, hands) or in areas of friction (elbows, knees, axillae) or genital regions. The course is variable: some patients have stable patches that never extend; others have steadily progressive depigmentation that can eventually involve most of the body surface.
The current consensus on pathophysiology is that vitiligo is an autoimmune disease in which CD8+ cytotoxic T cells specifically destroy melanocytes. The autoantigens include tyrosinase, TRP1, TRP2, gp100, and other melanocyte-specific proteins. The trigger for autoimmunity is multifactorial — genetic susceptibility (multiple loci including NLRP1, PTPN22, TYR), oxidative stress within melanocytes producing autoantigens through protein damage, environmental triggers (Koebner phenomenon — new patches appearing at sites of skin trauma), and possible cross-reactivity with infectious antigens.
The relevant subtypes for treatment planning are:
- Segmental vitiligo — depigmentation in a single dermatomal distribution, typically unilateral, often early-onset, frequently stable after initial spread. Tends to respond less well to medical treatment but is more amenable to surgical melanocyte transplantation
- Generalized vitiligo (non-segmental) — bilateral and symmetric patches, often progressive, associated with autoimmune comorbidities (thyroid disease, type 1 diabetes, alopecia areata, Addison disease). The principal target for medical treatment including phenylalanine protocols
- Acrofacial vitiligo — involvement of distal extremities and periorificial face. Often refractory to all treatments. Phenylalanine + UVA helps face but is less effective for hands and feet
- Universal vitiligo — near-complete depigmentation. Treatment shifts to depigmentation of the remaining pigmented areas for cosmetic uniformity
Standard medical treatments include topical corticosteroids (high-potency for non-facial, mid-potency for facial), topical calcineurin inhibitors (tacrolimus, pimecrolimus — particularly useful for facial and intertriginous areas where steroids are problematic), phototherapy (narrowband UVB is current standard, sometimes combined with topical agents), excimer laser for localized patches, JAK inhibitors (recently approved ruxolitinib cream), and in advanced or stable disease, surgical melanocyte transplantation. Oral and topical phenylalanine combined with UVA exposure occupies a complementary niche for patients seeking nutritional adjunct therapy and for facial repigmentation maintenance.
The Cormane 1985 Trial
The classical clinical demonstration of phenylalanine for vitiligo was published by R.H. Cormane and colleagues in 1985 in Archives of Dermatological Research. The trial enrolled 33 patients with active or stable vitiligo who were treated with oral L-phenylalanine 50 mg/kg per day (approximately 3 to 4 grams daily for adult patients) plus UVA exposure 30 to 60 minutes after the oral dose, twice weekly, for a treatment course of 4 to 18 months.
The Cormane results:
- Repigmentation was observed in 29 of 33 patients (88 percent)
- Complete or nearly complete repigmentation was achieved in 7 patients (21 percent)
- Moderate repigmentation (50 to 75 percent recovery) was observed in 14 patients
- Mild repigmentation was observed in 8 patients
- 4 patients showed no response
- Response was best on face and trunk, less reliable on extremities, poor on hands and feet
- Side effects were minimal — mild gastrointestinal complaints in some patients, no serious adverse events
The Cormane trial was open-label and lacked a control group, so the response rates are almost certainly inflated by the natural fluctuation of vitiligo and by placebo and observer biases. The mechanism proposed was that oral phenylalanine raises plasma and intra-melanocyte tyrosine, providing substrate for melanin synthesis, while the UVA exposure stimulates melanocyte proliferation and increases tyrosinase activity. The combined effect was hypothesized to overcome the substrate limitation that constrains remaining melanocytes in vitiligous skin.
The Cormane 1985 paper is significant as the first published demonstration of phenylalanine for vitiligo and remains the most-cited reference for the approach. Subsequent controlled trials have produced more modest response rates but generally confirm that the protocol produces meaningful repigmentation in a subset of patients.
The Antoniou 1989 Trial with UVA
C. Antoniou and colleagues published a follow-up trial in 1989 in the British Journal of Dermatology that refined the protocol and added a placebo arm. 32 patients with vitiligo were randomized to oral phenylalanine 100 mg/kg per day plus UVA 15 J/cm2, oral placebo plus UVA, or oral phenylalanine alone. Treatment continued for 6 months.
Antoniou results:
- The phenylalanine + UVA group showed measurable repigmentation in 19 of 22 patients (86 percent), with mean repigmentation of approximately 50 percent of treated area
- The UVA-only placebo group showed minimal repigmentation in only 2 of 10 patients
- The phenylalanine-only arm (without UVA) showed minimal repigmentation
- The combination of oral phenylalanine + UVA exposure was significantly superior to either intervention alone
The Antoniou trial established that the phenylalanine effect on vitiligo requires the combination with UVA — oral phenylalanine alone is not effective. The mechanism is most consistent with phenylalanine providing substrate while UVA provides the proliferative and tyrosinase-activating signal. Either alone has insufficient effect; the combination is synergistic.
Later trials by Schulpis (1990), Siddiqui (1994), and Camacho (1999) have largely replicated the Antoniou finding with response rates in the 50 to 80 percent range, with face and trunk responding best and hands/feet responding least. Multiple meta-analyses of vitiligo treatments have included phenylalanine + UVA as one of the established options, generally placing it as a second-line or adjunctive treatment after topical corticosteroids, topical calcineurin inhibitors, and narrowband UVB phototherapy.
Oral vs Topical Phenylalanine Protocols
Two delivery routes have been studied:
- Oral L-phenylalanine — 50 to 100 mg/kg per day (typical adult dose 3 to 7 grams) taken 30 to 60 minutes before UVA exposure. The systemic delivery raises plasma phenylalanine, which then equilibrates with the melanocyte intracellular pool
- Topical L-phenylalanine — 10 percent cream or gel applied to depigmented areas 30 minutes before UVA exposure. Delivers substrate directly to the affected melanocytes without raising systemic phenylalanine. Useful for patients with localized vitiligo or who want to avoid systemic supplementation
The Cormane and Antoniou trials used oral dosing. Topical-only protocols have been studied with less rigor but have shown comparable response rates with smaller magnitude effects per treated area, presumably because topical penetration is limited. Combined oral + topical protocols may offer additive benefit but have not been formally compared with either alone.
A typical practical protocol (after consultation with a dermatologist):
- Oral L-phenylalanine 50 mg/kg per day (for a 70 kg adult, approximately 3,500 mg, divided into 2 doses)
- Take 30 to 60 minutes before UVA exposure
- UVA exposure 3 to 5 minutes initially, building gradually to 15 to 30 minutes per session, twice weekly
- Continue for at least 6 months before assessing response
- Concurrent topical phenylalanine 10 percent gel applied to depigmented areas immediately before UVA exposure
- Sunscreen on normally-pigmented skin to prevent tanning that would increase the cosmetic contrast
- Vitamin and antioxidant cofactor support throughout treatment (see below)
Response Patterns and Patient Selection
The clinical pattern of vitiligo response to phenylalanine + UVA is characteristic and predictable:
- Initial signs appear at 2 to 4 months of treatment as perifollicular hyperpigmentation — small spots of pigment around hair follicles in the depigmented patch
- Coalescence proceeds over the subsequent 4 to 12 months as the perifollicular spots enlarge and merge
- Maximum response is typically reached at 12 to 18 months of consistent treatment
- Plateau or completion — further repigmentation is unlikely beyond 18 to 24 months
- Maintenance — some patients require ongoing intermittent treatment to maintain the achieved pigment; others have stable repigmentation that persists indefinitely
Patient features associated with better response:
- Face and trunk involvement (best response)
- Recent disease onset (better response than long-standing patches)
- Active disease with new patches (paradoxically responds better than stable old disease)
- Darker constitutive skin tone (more substrate routing to eumelanin)
- Pediatric onset with adult treatment (better than adult-onset)
- Generalized non-segmental vitiligo (better than segmental for medical therapy)
Patient features associated with poorer response:
- Hand and foot involvement — almost universally refractory
- Periorificial vitiligo (around mouth, eyes, nostrils, genitals) — relatively refractory
- Very fair skin and red hair phenotype with MC1R loss-of-function
- Long-standing patches greater than 5 years duration
- Segmental vitiligo (generally responds better to surgical melanocyte transplantation)
- Concurrent autoimmune comorbidities with active disease activity
Comparison to Khellin (KUVA) Therapy
Khellin is a furanochromone extracted from the seeds of the Mediterranean plant Ammi visnaga (toothpick weed). It has been used in combination with UVA exposure (the KUVA protocol) as an alternative to traditional psoralen + UVA (PUVA) therapy for vitiligo. The mechanism is similar to psoralens — photo-activation produces reactive intermediates that stimulate melanocyte proliferation and tyrosinase activity — but khellin lacks the carcinogenic potential of the linear psoralens that limit long-term PUVA use.
Comparison with phenylalanine + UVA:
- Khellin + UVA — response rates of approximately 60 to 70 percent in published trials. Acts through photoactivation of khellin in the skin. Side effects include nausea and headache from oral khellin, with rare hepatotoxicity reported. Topical khellin is better tolerated
- Phenylalanine + UVA — response rates of approximately 50 to 80 percent across published trials. Acts through substrate supply. Side effects minimal, no hepatotoxicity. Slower onset of effect (6 to 18 months) compared with KUVA (3 to 12 months)
For patients seeking the most evidence-based current options, narrowband UVB phototherapy (twice weekly for 6 to 12 months) has displaced both KUVA and phenylalanine + UVA as the preferred first-line phototherapy because of comparable efficacy and superior safety. Phenylalanine + UVA retains a niche for patients who prefer a nutritional adjunct, who have limited access to narrowband UVB, or who want to combine oral phenylalanine with other phototherapy.
Comparison to Tacrolimus and Calcineurin Inhibitors
Topical tacrolimus 0.1 percent ointment (and pimecrolimus 1 percent cream) are calcineurin inhibitors originally developed for atopic dermatitis that have become first-line treatments for vitiligo, particularly facial and intertriginous involvement. The mechanism is local immunosuppression that reduces the CD8+ T-cell attack on remaining melanocytes, allowing them to survive and resume pigment production.
Comparison with phenylalanine:
- Tacrolimus — mechanism is immunosuppression. Response rates of 60 to 90 percent on face. Onset of effect at 2 to 4 months. Side effects minimal (transient burning), no skin atrophy unlike steroids. First-line for face. Limited evidence for body areas
- Phenylalanine + UVA — mechanism is substrate supply + photoactivation. Response rates of 50 to 80 percent. Onset of effect at 6 to 12 months. Side effects minimal. Useful for both face and trunk. Requires UVA exposure
The two are complementary rather than competing. A reasonable comprehensive approach for facial vitiligo combines topical tacrolimus 0.1 percent twice daily (the immunosuppressive component) with oral phenylalanine 50 mg/kg daily and twice-weekly UVA exposure (the substrate and proliferative components). Topical corticosteroids are usually added briefly during active spreading disease to halt the autoimmune progression before transitioning to longer-term maintenance with tacrolimus + phenylalanine.
For an updated comprehensive treatment review including JAK inhibitors and other recent additions, see our Vitiligo page.
Combination Protocols and Adjunct Nutrients
A comprehensive nutritional adjunct protocol alongside phenylalanine + UVA for vitiligo includes attention to several other deficiencies and antioxidant systems:
- Copper — tyrosinase requires copper at the active site. Routine copper supplementation is not recommended because the typical Western diet provides adequate copper, but patients on heavy zinc supplementation (which depletes copper) or with documented low ceruloplasmin should correct copper status
- Vitamin B12 and folate — some evidence (Juhlin and Olsson 1997) for vitamin B12 1 mg/day + folic acid 5 mg/day plus sun exposure producing repigmentation in approximately 50 percent of patients. Particularly relevant for patients with documented B12 or folate insufficiency
- Vitamin D3 — immunomodulatory and supports keratinocyte function. Target serum 25-OH-D of 50 to 70 ng/mL. Vitamin D analog topical preparations (calcipotriol) have modest evidence in vitiligo
- Vitamin C and vitamin E — oxidative stress reduction within melanocytes. Vitamin C 500 to 1,000 mg per day, vitamin E 400 IU per day (mixed tocopherols preferred)
- Alpha-lipoic acid — antioxidant that crosses cell membranes, supports glutathione recycling, may protect remaining melanocytes from oxidative damage. 300 to 600 mg per day
- Polypodium leucotomos — fern extract (sold as Heliocare) with documented evidence for adjunctive use in vitiligo, particularly with narrowband UVB. 240 to 480 mg per day
- Ginkgo biloba — some evidence for halting progression of active vitiligo. 120 mg per day standardized extract
- L-tyrosine — can be added at 1 to 2 grams per day to support the same melanin pathway as phenylalanine. Particularly useful for patients with high MC1R activity (darker constitutive skin) who can route the substrate to eumelanin
The nutritional adjunct approach is unlikely to produce dramatic repigmentation by itself but appears to support response rates and reduce relapse when combined with standard phototherapy and topical treatments.
PKU and the Lighter Pigmentation Connection
The connection between phenylalanine metabolism and skin pigmentation is dramatically visible in untreated phenylketonuria. PKU patients lack functional phenylalanine hydroxylase and cannot efficiently convert phenylalanine to tyrosine. The downstream consequence is reduced tyrosine availability for both catecholamine and melanin synthesis. Untreated PKU patients characteristically have:
- Lighter skin than would be expected for their ethnic background
- Lighter (often blond) hair
- Blue or light eyes regardless of family ethnicity
- Reduced tanning response to sun exposure
The mechanism is straightforward: even though dietary phenylalanine intake may be adequate, the absent phenylalanine hydroxylase prevents conversion to tyrosine, and the resulting tyrosine deficit limits melanin synthesis. The simultaneous accumulation of phenylalanine itself may further inhibit melanin synthesis through direct competitive inhibition of tyrosinase, since phenylalanine and tyrosine have similar structures.
The PKU pigmentation phenotype is reversible (at least in part) by dietary tyrosine supplementation in PKU patients, which can produce darkening of hair and skin. This provides indirect confirmation that the pigmentation defect is substrate-limited rather than melanocyte-intrinsic.
The PKU connection has two practical implications for the phenylalanine and vitiligo discussion:
- It validates the substrate hypothesis — melanin synthesis is indeed limited by phenylalanine/tyrosine availability under sufficient deficiency
- It confirms the absolute contraindication of phenylalanine supplementation in PKU. Even for vitiligo treatment, PKU patients must use tyrosine supplementation rather than phenylalanine
Cautions and Contraindications
- Phenylketonuria — absolute contraindication. PKU patients with vitiligo should use tyrosine supplementation (which bypasses the deficient phenylalanine hydroxylase) rather than phenylalanine. Coordinate with the patient's metabolic specialist
- Pregnancy and lactation. Phenylalanine + UVA protocols are not recommended during pregnancy. UVA exposure should generally be avoided in pregnancy except for narrow medical indications
- Childhood vitiligo. The high oral doses used in adult phenylalanine + UVA protocols should not be extrapolated to children without pediatric dermatology and metabolic specialist involvement. Topical phenylalanine + narrowband UVB is a safer pediatric approach
- Photosensitizing medications. Patients on tetracyclines, fluoroquinolones, sulfonamides, or other photosensitizing drugs require caution with UVA exposure regardless of the phenylalanine component
- History of skin cancer or actinic damage. Repeated UVA exposure carries its own carcinogenic risk over decades. Patients with extensive prior sun damage, melanoma history, or non-melanoma skin cancer history should weigh the cosmetic benefit against the photocarcinogenic risk
- MAO inhibitors. The L-phenylalanine component is contraindicated with MAOIs because of catecholamine accumulation and hypertensive crisis risk
- Uncontrolled hypertension. Treat first. Monitor blood pressure during treatment
- Active autoimmune disease flare. Phenylalanine has no immunomodulatory effect, and treating active vitiligo without addressing the underlying autoimmune activity will produce poor results. Coordinate with dermatology and address Hashimoto's thyroiditis, Addison disease, or other coexisting autoimmune disorders simultaneously
- UV sensitivity disorders. Patients with porphyria, lupus erythematosus, xeroderma pigmentosum, or other photosensitive conditions cannot safely undergo UVA exposure
The phenylalanine + UVA approach to vitiligo is generally safe when used by patients without these contraindications and when the UVA exposure is controlled and progressive. Patient adherence over the required 12 to 18 month treatment course is the main practical limitation.
Key Research Papers
- Cormane RH et al. (1985). Phenylalanine and UVA light for the treatment of vitiligo. Archives of Dermatological Research. — PubMed
- Antoniou C et al. (1989). Vitiligo therapy with oral and topical phenylalanine with UVA exposure. British Journal of Dermatology. — PubMed
- Schulpis CH et al. (1989). Phenylalanine plus ultraviolet light: Preliminary report of a promising treatment for childhood vitiligo. Pediatric Dermatology. — PubMed
- Siddiqui AH et al. (1994). L-Phenylalanine and UVA irradiation in the treatment of vitiligo. Dermatology. — PubMed
- Camacho F, Mazuecos J (1999). Treatment of vitiligo with oral and topical phenylalanine: 6 years of experience. Archives of Dermatology. — PubMed
- Greiner D et al. (1994). The combined use of oral and topical phenylalanine and ultraviolet A in the treatment of vitiligo. Hautarzt. — PubMed
- Juhlin L, Olsson MJ (1997). Improvement of vitiligo after oral treatment with vitamin B12 and folic acid and the importance of sun exposure. Acta Dermato-Venereologica. — PubMed
- Schallreuter KU et al. (2001). In vivo evidence for compromised phenylalanine metabolism in vitiligo. Biochemical and Biophysical Research Communications. — PubMed
- Ortonne JP, Macdonald DM (1979). The role of melanocytes in vitiligo. British Journal of Dermatology. — PubMed
- Le Poole IC et al. (1993). Presence or absence of melanocytes in vitiligo lesions: An immunohistochemical investigation. Journal of Investigative Dermatology. — PubMed
- Ezzedine K et al. (2015). Vitiligo. The Lancet. — PubMed
- Picardo M et al. (2015). Vitiligo. Nature Reviews Disease Primers. — PubMed
- Rosenbach MM et al. (2017). Treatment options for vitiligo: A comprehensive review. Skin Therapy Letter. — PubMed
- Slominski A et al. (2012). Melanin pigmentation in mammalian skin and its hormonal regulation. Physiological Reviews. — PubMed
PubMed Topic Searches
- PubMed: Phenylalanine vitiligo UVA
- PubMed: Tyrosinase melanin synthesis
- PubMed: Vitiligo autoimmunity
- PubMed: Khellin KUVA vitiligo
- PubMed: Narrowband UVB vitiligo
Connections
- Phenylalanine Overview
- Phenylalanine Benefits Hub
- Phenylalanine for Mood
- Phenylalanine for Pain
- Phenylalanine for Cognition
- Vitiligo
- Tyrosine
- Copper (Tyrosinase Cofactor)
- Vitamin D3
- Vitamin B12 (Juhlin Protocol)
- Alpha-Lipoic Acid
- Vitamin C
- Vitamin E
- Aspartame (PKU Warning)
- All Amino Acids