Phenylalanine for Cognitive Function
Phenylalanine is the precursor of the four molecules that drive sustained attention, working memory, and motivation in the human brain: dopamine, norepinephrine, epinephrine, and thyroid hormone. It is one of the very few molecules with this combined regulatory role, and the only one that the body must obtain entirely through diet. The cognitive consequences of phenylalanine availability are remarkably bidirectional — deficiency through restricted diet or acute depletion measurably impairs working memory and attention within hours, while the rare opposite condition of phenylalanine excess (untreated phenylketonuria) is one of the most catastrophic causes of acquired intellectual disability known to medicine. The narrow therapeutic window between these two extremes is enforced by the same precursor that, in adequate amounts, supports cognitive performance under stress. This deep-dive explores the neuroscience of phenylalanine's cognitive role, the rare opposite story of PKU toxicity, and the unresolved aspartame controversy that connects them.
Table of Contents
- The Four Cognitive Molecules Phenylalanine Builds
- Dopamine and Prefrontal Cortex Function
- Norepinephrine, Locus Coeruleus, and Attention
- Epinephrine and Thyroid Hormone in Energy Cognition
- The Blood-Brain Barrier and LAT1 Competition
- Acute Phenylalanine and Tyrosine Depletion Studies
- Cognitive Performance Under Stress
- ADHD, Focus, and the Limits of Catecholamine Loading
- Aging Cognition and Catecholamine Decline
- PKU — The Rare Opposite Story of Phenylalanine Toxicity
- The Aspartame Controversy
- Dosing for Cognitive Support and Cofactor Requirements
- Cautions, Drug Interactions, and Contraindications
- Key Research Papers
- Connections
- Featured Videos
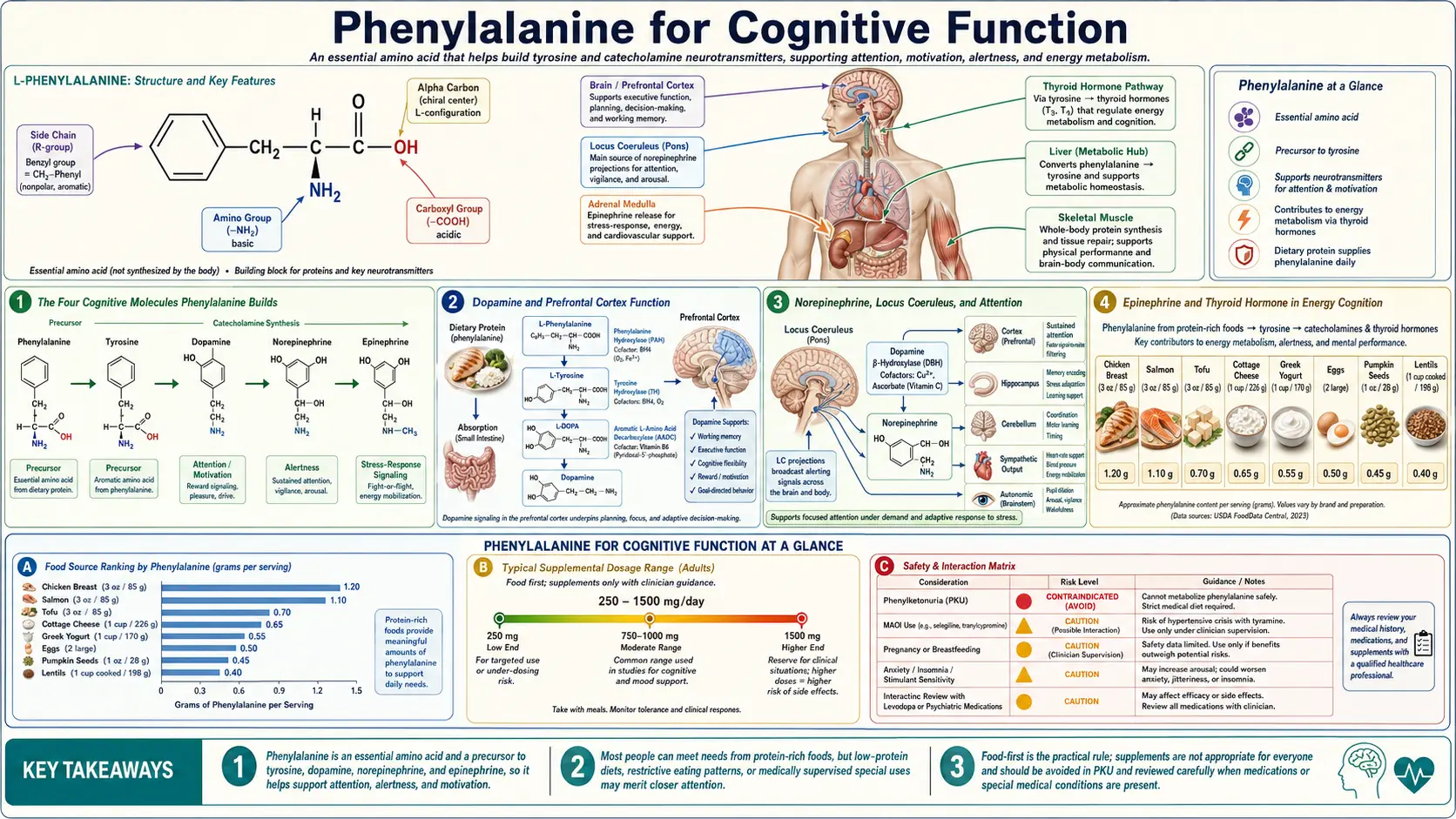
The Four Cognitive Molecules Phenylalanine Builds
Most amino acids have either a structural role (protein synthesis) or a single signaling role (precursor of one neurotransmitter or hormone). Phenylalanine is unusual in that it serves as the structural precursor for at least four distinct categories of cognitively important molecules:
- Dopamine — the principal catecholamine of the prefrontal cortex and the mesolimbic reward system. Drives motivation, reward processing, working memory, and the subjective sense of agency. Deficiency manifests as apathy, anhedonia, brain fog, and loss of cognitive flexibility.
- Norepinephrine — the principal catecholamine of the locus coeruleus and the dorsolateral prefrontal cortex. Drives sustained attention, signal-to-noise ratio in cortical processing, arousal, and alertness. Deficiency manifests as poor concentration, distractibility, mental fatigue, and inability to focus under stress.
- Epinephrine — the principal catecholamine of the adrenal medulla, with a smaller central nervous system role. Drives the acute stress response that mobilizes energy for cognitive performance under demanding conditions. Deficiency contributes to fatigue, hypotension, and inability to mount an alerting response.
- Thyroid hormone (T3 and T4) — iodinated tyrosine residues coupled in the thyroid gland to form thyroxine (T4) and triiodothyronine (T3). Regulates basal metabolic rate, brain energy supply, and broader cellular function. Thyroid deficiency produces profound cognitive slowing, memory impairment, depression, and apathy.
The thread that connects these four is that all are tyrosine-derived. Phenylalanine sits one step upstream of tyrosine, and the human body's primary route to tyrosine is hepatic hydroxylation of dietary phenylalanine by phenylalanine hydroxylase. Tyrosine is therefore considered a "conditionally essential" amino acid — not strictly required in the diet provided phenylalanine intake is adequate and the hydroxylation enzyme is functional. The cognitive effects of phenylalanine intake are largely (but not entirely) effects of the tyrosine pool that results.
The exception — and the reason phenylalanine itself has unique effects beyond what tyrosine provides — is that phenylalanine can also be decarboxylated to phenylethylamine (PEA), a trace amine with its own modest catecholamine-releasing and mood-elevating effects. The Sabelli school of thought treats PEA as part of the cognitive and mood effects of phenylalanine supplementation; the conventional view treats PEA as a minor pathway and focuses on the catecholamine cascade.
Dopamine and Prefrontal Cortex Function
The prefrontal cortex is the seat of working memory, executive function, planning, cognitive flexibility, and the ability to maintain goal-directed behavior in the face of distraction. Its function is highly sensitive to dopamine concentration, and dopamine availability in the prefrontal cortex follows an inverted U-shaped curve: too little dopamine produces inattention, poor working memory, and impulsivity (the ADHD-like profile), while too much dopamine produces excessive distractibility, intrusive thoughts, and ultimately psychotic symptoms.
The healthy adult sits comfortably in the middle of this inverted U for most of the day, but the dopamine availability can shift in either direction under various conditions:
- Acute stress increases prefrontal dopamine release, initially improving performance but with excessive stress overshooting the optimum and degrading performance
- Chronic stress depletes catecholamine stores faster than they can be resynthesized, producing the executive dysfunction characteristic of chronic stress states
- Inadequate sleep reduces dopamine receptor sensitivity and effectively shifts the curve to the left, requiring more catecholamine to achieve the same effect
- Aging reduces tonic dopamine production and receptor density, producing a gradual leftward shift on the curve
- Dietary catecholamine precursor restriction (vegan or very-low-protein diets without supplementation) can produce subclinical insufficiency that manifests as reduced cognitive resilience
The phenylalanine precursor loading rationale for cognitive support targets the leftward shift — the situations where catecholamine availability is the limiting factor. In a well-rested, well-nourished, low-stress adult, adding phenylalanine produces little measurable cognitive effect because the catecholamine system is already operating near the top of the inverted U. In a stressed, sleep-deprived, cognitively-overloaded adult with marginal precursor intake, adding phenylalanine can produce a measurable cognitive benefit by replenishing the depleted precursor pool.
Norepinephrine, Locus Coeruleus, and Attention
Norepinephrine is produced primarily by the locus coeruleus, a small nucleus in the dorsal pons that sends projections throughout the cortex and provides the principal arousal and attention signal to the entire forebrain. The locus coeruleus fires tonically at a low baseline rate and phasically in response to salient stimuli, raising signal-to-noise ratio across cortical circuits and improving the detection of important information.
The cognitive effects of norepinephrine include:
- Sustained attention — the ability to maintain focus on a task over time without losing engagement
- Vigilance — the ability to detect a rare signal in a noisy background
- Working memory robustness — the ability to maintain information in working memory despite distraction
- Cognitive flexibility — the ability to switch between cognitive sets when task demands change
- Selective attention — the ability to filter relevant from irrelevant input
Norepinephrine availability follows the same inverted U as dopamine. The selective norepinephrine reuptake inhibitors used for ADHD (atomoxetine, viloxazine) work by raising synaptic norepinephrine in the prefrontal cortex into the optimal range for the patient. Phenylalanine and tyrosine precursor loading shifts the curve from the substrate-availability end rather than the reuptake end. The mechanism is mechanistically distinct but the cognitive effect is in the same direction.
An important practical caveat for cognitive supplementation: the norepinephrine cognitive enhancement window is narrow. A patient who responds well to 500 mg of L-phenylalanine for focus may find that 1,500 mg produces jitteriness, anxiety, and degraded performance. The therapeutic dose is the smallest dose that produces benefit, not the largest dose that is tolerated.
Epinephrine and Thyroid Hormone in Energy Cognition
Epinephrine (adrenaline) is produced predominantly in the adrenal medulla rather than the central nervous system, but it contributes to cognitive performance through its effects on cerebral blood flow, glucose mobilization, and the general "fight or flight" alerting response that improves cognitive performance under acute demand. The phenylalanine-tyrosine-dopamine-norepinephrine-epinephrine cascade ends with epinephrine, and adrenal epinephrine production draws on the same precursor pool that supplies central catecholamines.
Thyroid hormone is a separate but parallel branch of phenylalanine metabolism. In the thyroid gland, tyrosine residues within thyroglobulin are iodinated by thyroid peroxidase (TPO) in the presence of iodine and hydrogen peroxide. Pairs of iodinated tyrosines are then coupled to form T4 (two diiodotyrosines) or T3 (one monoiodotyrosine + one diiodotyrosine). The final products are released into circulation as T4 and T3.
The cognitive consequences of thyroid hormone status are profound. Hypothyroidism (low T4 and T3) produces:
- Slowed cognitive processing speed
- Word-finding difficulty
- Impaired short-term memory
- Daytime fatigue and mental fog
- Depressed mood with low motivation
- Reduced exercise tolerance and physical fatigue
The cognitive impairment of hypothyroidism is reversible with thyroid hormone replacement, although recovery can take weeks to months. While iodine deficiency is the most common nutritional cause of insufficient thyroid hormone production worldwide, in iodine-replete populations the substrate availability question shifts to tyrosine. A patient with adequate iodine but marginal protein intake can have suboptimal thyroid hormone synthesis, and phenylalanine or tyrosine supplementation can support thyroid function as part of comprehensive thyroid optimization. See our Hypothyroidism page for the broader thyroid context.
The Blood-Brain Barrier and LAT1 Competition
The cognitive effects of orally administered phenylalanine depend on the amino acid reaching the brain in adequate concentrations. The route is not trivial. Phenylalanine crosses the blood-brain barrier (BBB) via the LAT1 transporter (system L), which also transports the other large neutral amino acids: leucine, isoleucine, valine, methionine, tryptophan, histidine, and tyrosine. The transporter has limited capacity and the LNAAs compete with each other for transport.
The practical implication is that taking phenylalanine with a protein-rich meal substantially reduces brain delivery. The other LNAAs released by digestion of the protein compete with phenylalanine for LAT1 binding sites, and the net brain phenylalanine concentration may not rise much above baseline. Taking phenylalanine 30 to 60 minutes before a meal, or 90 to 120 minutes after a meal, when other LNAA concentrations are at their lowest, optimizes brain delivery.
A complementary insight is that high carbohydrate meals can increase the ratio of phenylalanine and tyrosine to other LNAAs because the insulin released in response to the carbohydrate preferentially shifts BCAAs (leucine, isoleucine, valine) into skeletal muscle for protein synthesis, reducing the competing pool. This is the same mechanism that underlies the serotonin / tryptophan / carbohydrate cognitive effect — high-carb meals favor tryptophan transport and serotonin synthesis. The same mechanism, applied to phenylalanine, means a moderate carbohydrate meal taken about 30 minutes before phenylalanine supplementation can improve brain delivery.
Acute Phenylalanine and Tyrosine Depletion Studies
One of the cleanest experimental approaches to demonstrating the cognitive role of phenylalanine and tyrosine is acute amino acid depletion. The protocol involves administering a balanced amino acid mixture that excludes phenylalanine and tyrosine. The resulting protein synthesis in the liver consumes the body's plasma pool of these amino acids without replenishment, transiently lowering plasma and brain concentrations within 4 to 6 hours. The cognitive effects can then be measured against a control mixture that includes all amino acids.
The acute phenylalanine/tyrosine depletion literature has consistently demonstrated:
- Reduced spatial working memory performance
- Slower reaction times on attention tasks
- Impaired cognitive flexibility on set-shifting tasks
- Reduced motivation for effortful cognitive tasks
- Subjective reports of fatigue and reduced mental sharpness
- Reduced striatal dopamine synthesis confirmed by PET imaging
These effects are typically modest in magnitude but consistent across studies. The depletion is also reversible — reintroducing phenylalanine and tyrosine restores baseline cognitive performance within hours. The effects are most pronounced on tasks that depend on prefrontal cortex function (working memory, set-shifting, decision-making) and less pronounced on tasks that depend on other brain regions (declarative memory, language).
The depletion paradigm is the closest the cognitive neuroscience literature comes to a controlled experimental demonstration that catecholamine precursor availability causally affects human cognitive function. The complementary supplementation paradigm (giving extra phenylalanine or tyrosine to baseline-normal subjects) shows much smaller effects because most subjects are operating near the top of the inverted U at baseline.
Cognitive Performance Under Stress
The most compelling cases for phenylalanine or tyrosine supplementation for cognitive enhancement come from situations of sustained cognitive load combined with acute stress: military operations, extended cognitive demand under sleep deprivation, cold exposure, hypoxia at altitude, and the prolonged demand of complex skilled tasks under emotional pressure.
The mechanism: acute stress accelerates catecholamine release and turnover at a rate that exceeds the resynthesis capacity of the catecholamine neurons. Over hours to days of sustained stress, the precursor pool can become depleted, and the catecholamine system shifts from acute mobilization to exhaustion. Cognitive performance, which initially improves under modest stress, eventually deteriorates as the catecholamine reserves are spent.
The Banderet and Lieberman 1989 trial at the US Army Research Institute of Environmental Medicine is the most-cited demonstration of this effect. Soldiers were given tyrosine 100 mg/kg (approximately 7 grams in a 70 kg adult) before extended cold exposure at altitude. The tyrosine-supplemented group showed measurably better performance on cognitive tasks under the dual stress compared with placebo. Subsequent military research has consistently replicated this finding in stressors that combine cognitive demand with physiologic stress.
Translation to civilian cognitive demand: the same principle applies, at a much smaller magnitude, to demanding professional work under pressure. A patient facing an unusually demanding cognitive task (extended exam preparation, intensive problem-solving sprint, high-stakes public speaking, demanding professional examination) may benefit from a single dose of L-phenylalanine 500 to 1,000 mg or L-tyrosine 1 to 2 grams on the morning of the event, taken 30 to 60 minutes before the cognitive demand begins.
ADHD, Focus, and the Limits of Catecholamine Loading
ADHD (Attention Deficit Hyperactivity Disorder) is the prototypical disorder of insufficient prefrontal catecholamine signaling. The first-line pharmacologic treatments (methylphenidate, mixed amphetamine salts) work primarily by increasing synaptic dopamine and norepinephrine in the prefrontal cortex. The second-line treatments (atomoxetine, viloxazine) work through norepinephrine reuptake inhibition. All work by raising catecholamine signaling.
The natural question is whether phenylalanine or tyrosine precursor loading could approach the same effect through substrate availability rather than reuptake inhibition. The answer from the limited research base is: partial and inconsistent.
The Wood 1985 trial in Psychiatry Research reported DLPA at 1,200 mg per day produced modest improvement in adult ADHD symptoms in 11 of 19 patients over 4 weeks, with benefits lost during a subsequent washout. This is consistent with the general inverted U principle — patients with truly low baseline catecholamine availability can benefit from precursor loading, but the effect ceiling is lower than what stimulant medication can achieve.
Practical reality: phenylalanine and tyrosine should not be considered substitutes for properly indicated stimulant medication for moderate to severe ADHD. They can be useful as adjuncts, particularly for patients who experience medication "crashes" as the stimulant wears off (the crash is partly catecholamine depletion, which precursor loading can ameliorate). They can also be useful for adults with mild attentional difficulties who do not meet full ADHD criteria but who would benefit from modest catecholamine support without controlled-substance prescriptions.
The dose-response curve for ADHD-like indications is narrow. Start at 500 mg L-phenylalanine in the morning. Increase weekly by 250 mg if needed and tolerated. Most responders find their effective dose between 750 and 1,500 mg per day. Doses above 2,000 mg per day commonly produce jitteriness and decreased focus without additional benefit.
Aging Cognition and Catecholamine Decline
Aging brings a progressive decline in catecholamine availability through multiple mechanisms: reduced tyrosine hydroxylase activity in catecholamine-producing neurons, gradual loss of catecholamine-producing neurons themselves (most prominently the substantia nigra dopaminergic neurons, the locus coeruleus norepinephrine neurons, and the ventral tegmental area dopaminergic neurons), reduced receptor density, and altered receptor function.
The cognitive manifestations of normal aging that map to catecholamine decline include:
- Slower processing speed
- Reduced working memory capacity
- Increased distractibility
- Reduced cognitive flexibility on set-shifting tasks
- Subjective reduction in motivation and "drive"
- Mild but real decline in sustained attention
Whether precursor loading can meaningfully counter this age-related decline is not well established. The few clinical trials of phenylalanine or tyrosine in healthy older adults have shown modest effects on selected cognitive measures but nothing approaching the dramatic effects sometimes claimed in popular nutritional literature. The mechanistic limitation is that the age-related decline involves loss of catecholamine-producing neurons themselves, not just precursor availability — providing more substrate cannot rebuild lost cells.
What may be more meaningful in aging cognition is the cluster of related interventions: phenylalanine or tyrosine 500 to 1,500 mg per day plus methylated B vitamins (B6, B9, B12) to support BH4 recycling, plus magnesium for NMDA receptor modulation, plus omega-3 fatty acids for neuronal membrane fluidity, plus regular aerobic exercise to support BDNF and neurogenesis. The bundled effect is probably greater than any single intervention.
PKU — The Rare Opposite Story of Phenylalanine Toxicity
Phenylketonuria (PKU) is the most famous inborn error of amino acid metabolism and one of the most catastrophic. It is caused by loss-of-function mutations in the gene encoding phenylalanine hydroxylase (PAH), the hepatic enzyme that converts phenylalanine to tyrosine. In classical PKU, PAH activity is essentially absent, and dietary phenylalanine accumulates progressively in plasma and brain to neurotoxic levels.
The natural history of untreated PKU is severe: infants appear normal at birth, develop progressive intellectual disability over the first months of life, show growth retardation and eczematous skin changes, and reach adulthood with severe intellectual disability (typical IQ < 50), seizures, autistic features, and a characteristic musty body odor from urinary phenylketones. Without treatment, life expectancy is shortened and quality of life is profoundly impaired.
The introduction of newborn screening for PKU in the 1960s (the Guthrie test) was one of the great preventive medicine successes of the 20th century. All US states and virtually all developed countries now screen every newborn for elevated phenylalanine in heel-stick blood within the first 48 hours of life. Infants identified with elevated phenylalanine are immediately started on a phenylalanine-restricted diet using specially formulated medical foods that provide all essential amino acids except phenylalanine. With early diagnosis and lifelong dietary management, intellectual outcome can be near-normal.
The dietary management is demanding. Natural protein intake must be severely restricted — essentially no meat, fish, eggs, dairy, soy, nuts, or wheat products. The protein needs are met by amino acid mixtures that exclude phenylalanine. Blood phenylalanine levels must be monitored regularly and maintained between 120 and 360 micromoles per liter. Maternal PKU during pregnancy carries particular risk because elevated maternal phenylalanine produces severe fetal damage even if the fetus is heterozygous (one normal PAH allele); women with PKU must achieve strict control before conception and maintain it throughout pregnancy.
The cognitive lesson from PKU: phenylalanine in excess is profoundly neurotoxic, presumably through multiple mechanisms including competition with other LNAAs for the LAT1 transporter (depleting brain tryptophan and tyrosine), direct interference with myelin synthesis, and disruption of energy metabolism. The same molecule that supports normal cognitive function within the normal range becomes a neurotoxin at the levels seen in untreated PKU.
The Aspartame Controversy
Aspartame is an artificial sweetener used in tens of thousands of food and beverage products, including most diet sodas, many sugar-free gums and candies, and some pharmaceutical formulations. Chemically, aspartame is a dipeptide composed of L-aspartic acid + L-phenylalanine methyl ester. In the gastrointestinal tract it is hydrolyzed to its three components: aspartic acid, phenylalanine, and methanol.
The aspartame controversy in cognitive function has several distinct components:
- PKU contraindication. Aspartame is unambiguously contraindicated in classical PKU. Every aspartame-containing product carries a regulatory warning ("Phenylketonurics: Contains phenylalanine") because the phenylalanine released from aspartame metabolism is identical to dietary phenylalanine and contributes to the plasma phenylalanine load that PKU patients must restrict. This is settled science.
- Phenylalanine-induced cognitive effects in non-PKU. The phenylalanine dose delivered by typical aspartame consumption is small compared with normal dietary protein intake. A 355 mL can of diet soda sweetened with aspartame contains approximately 100 mg of aspartame, releasing about 40 mg of phenylalanine. A typical chicken breast delivers about 1,500 mg of phenylalanine. The pharmacologic argument for aspartame producing cognitive effects in non-PKU patients through phenylalanine specifically is weak on dose-magnitude grounds alone.
- Excitotoxicity concerns from the aspartic acid component. The aspartic acid released from aspartame metabolism is identical to dietary aspartic acid (found in many foods), and the dose from aspartame is small relative to dietary intake. The excitotoxicity argument applied to aspartame has not held up in controlled human studies.
- Methanol concern. Aspartame metabolism releases methanol. The dose per serving is small (about 10 mg from a can of diet soda, compared with the larger natural methanol content of fruits and fruit juices), but cumulative chronic intake is a recurring concern in popular nutritional literature. Formal toxicology assessment has consistently concluded the methanol release from aspartame at typical intakes is well below the threshold for measurable toxicity.
- Broader cognitive and behavioral claims. Anecdotal reports and small uncontrolled studies have linked aspartame consumption to headache, mood changes, mental fog, and various behavioral symptoms in some sensitive individuals. The controlled study evidence is mixed, with several blinded challenge studies finding no consistent effects and others finding modest effects in subsets of self-identified aspartame-sensitive individuals.
The pragmatic clinical position: PKU patients must avoid aspartame (settled). Non-PKU patients who notice consistent cognitive or symptomatic effects from aspartame consumption can reasonably avoid it without medical risk — the population of artificial sweeteners offers alternatives (stevia, monk fruit, erythritol), and water remains the optimal beverage for most consumption occasions. The broader debate over aspartame safety in non-PKU adults remains unresolved and is unlikely to be resolved by additional research given the methodological difficulty of detecting small effects against large dietary background variation. See our Aspartame page for the detailed toxicology discussion.
Dosing for Cognitive Support and Cofactor Requirements
For acute cognitive demand (single-event use):
- L-phenylalanine 500 to 1,000 mg OR L-tyrosine 1 to 2 grams
- Take 30 to 60 minutes before the cognitive demand begins
- Best taken on an empty stomach or with a small carbohydrate snack (not with a protein meal)
- Do not exceed once-daily use for this indication — tolerance develops with frequent use
For chronic cognitive support:
- Starting dose: 500 mg L-phenylalanine in the morning
- Titrate weekly by 250 mg if needed and tolerated
- Typical maintenance: 750 to 1,500 mg per day
- Maximum self-directed dose: 2,000 mg per day
- Take in morning and (if divided) early afternoon — avoid evening dosing
- Take on an empty stomach, 30 minutes before meals
Essential cofactors:
- Pyridoxal-5-phosphate (active B6) — 25 to 50 mg per day. Required for the L-DOPA to dopamine decarboxylation
- Vitamin C — 500 to 1,000 mg per day. Required for the dopamine to norepinephrine hydroxylation by dopamine beta-hydroxylase
- Iron (if ferritin < 50 ng/mL) — required at the tyrosine hydroxylase active site. Excess iron can be harmful; correct deficiency rather than dose blindly
- Methylated folate and methylated B12 — support the methylenetetrahydrofolate (MTHF) recycling that regenerates tetrahydrobiopterin (BH4), the cofactor for both phenylalanine hydroxylase and tyrosine hydroxylase. Particularly important in patients with MTHFR polymorphisms
- Magnesium — 300 to 400 mg per day. Supports the broader stress-response axis and NMDA receptor modulation
Adequate sleep, regular exercise, and stress management are non-negotiable. Catecholamine precursor loading layered on top of severe sleep deprivation produces jittery cognitive impairment, not cognitive enhancement.
Cautions, Drug Interactions, and Contraindications
- Phenylketonuria — absolute contraindication. Any supplemental phenylalanine, plus aspartame in food and beverages, must be strictly avoided.
- MAO inhibitors. Hypertensive crisis risk. Avoid concurrent use with phenelzine, tranylcypromine, isocarboxazid, selegiline at depression doses, linezolid, and methylene blue.
- Stimulant medications (methylphenidate, amphetamines). Concurrent use can produce excessive catecholaminergic stimulation. Reduce phenylalanine dose or avoid in patients on stimulants for ADHD.
- Levodopa for Parkinson disease. Phenylalanine competes with levodopa for LAT1 transport and DOPA decarboxylase. Reduces levodopa effect. Do not combine without neurologist involvement.
- Antipsychotic medications. The dopamine D2 receptor blockade of antipsychotics blunts the catecholamine cognitive effect. May still be useful for the indirect mood support but the cognitive effect will be attenuated.
- Uncontrolled hypertension. Treat first; monitor blood pressure weekly during titration.
- Hyperthyroidism. Additional thyroid precursor availability may worsen hyperthyroid symptoms. Avoid until thyroid status is controlled.
- Schizophrenia and psychotic spectrum. Catecholamine boost can worsen positive psychotic symptoms.
- Pregnancy and lactation. Insufficient safety data for high-dose supplementation. Dietary protein only.
- Migraine. Subset of migraine patients have catecholamine-triggered migraine. Test at low dose first.
Key Research Papers
- Banderet LE, Lieberman HR (1989). Treatment with tyrosine, a neurotransmitter precursor, reduces environmental stress in humans. Brain Research Bulletin. — PubMed
- Lieberman HR et al. (2015). The catecholamine neurotransmitter precursor tyrosine increases anger during exposure to severe psychological stress. Psychopharmacology. — PubMed
- Jongkees BJ et al. (2015). Effect of tyrosine supplementation on clinical and healthy populations under stress or cognitive demands — A review. Journal of Psychiatric Research. — PubMed
- Harmer CJ et al. (2001). Effects of acute tyrosine depletion on subjective state and gambling in recently abstinent users of MDMA. Psychopharmacology. — PubMed
- McTavish SF et al. (1999). Effect of acute dopamine depletion on attention and decision-making in healthy volunteers. Psychopharmacology. — PubMed
- Mehta MA et al. (2000). Mnemonic effects of methylphenidate, with and without a working memory cost. Psychopharmacology. — PubMed
- Wood DR et al. (1985). Treatment of attention deficit disorder with DL-phenylalanine. Psychiatry Research. — PubMed
- Magnusson I et al. (1989). Plasma amino acid concentration profile in PKU patients and healthy controls. Acta Paediatrica Scandinavica. — PubMed
- Diamond A (2001). A model for the neural basis of motor and cognitive dysfunction following phenylalanine elevation in PKU. Mental Retardation and Developmental Disabilities Research Reviews. — PubMed
- van Spronsen FJ et al. (2017). Key European guidelines for the diagnosis and management of patients with phenylketonuria. Lancet Diabetes and Endocrinology. — PubMed
- Magnuson BA et al. (2007). Aspartame: A safety evaluation based on current use levels, regulations, and toxicological and epidemiological studies. Critical Reviews in Toxicology. — PubMed
- Humphries P et al. (2008). Direct and indirect cellular effects of aspartame on the brain. European Journal of Clinical Nutrition. — PubMed
- Rampersaud GC et al. (2003). Reduced folate, vitamin B-12, and homocysteine in older adults. American Journal of Clinical Nutrition. — PubMed
- Fernstrom JD, Fernstrom MH (2007). Tyrosine, phenylalanine, and catecholamine synthesis and function in the brain. Journal of Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Tyrosine cognitive performance under stress
- PubMed: Phenylalanine working memory
- PubMed: Acute APT depletion cognition
- PubMed: PKU cognitive outcomes
- PubMed: Aspartame cognition
Connections
- Phenylalanine Overview
- Phenylalanine Benefits Hub
- Phenylalanine for Mood
- Phenylalanine for Pain
- Phenylalanine for Skin Pigmentation
- Tyrosine
- Tryptophan (Cognitive Comparison)
- Vitamin B6 (PLP Cofactor)
- Vitamin C (DBH Cofactor)
- Iron (TH Cofactor)
- Iodine (Thyroid Hormone)
- Hypothyroidism
- Aspartame
- Artificial Sweeteners
- All Amino Acids