Phenylalanine for Pain Management
D-phenylalanine is one of the few synthetic D-amino acids with a documented and mechanistically clear clinical action in humans. Unlike the L-form, which feeds into protein synthesis and the catecholamine cascade, the D-form is metabolically inert for those purposes — the body's enzymes are stereospecific for L-amino acids and cannot use D-phenylalanine for either function. What the D-form does do is bind to and inhibit enkephalinase, the carboxypeptidase enzyme that degrades the endogenous pentapeptide opioids met-enkephalin and leu-enkephalin. By prolonging the synaptic half-life of the body's own opioids, D-phenylalanine amplifies endogenous opioid analgesia without producing tolerance, dependence, respiratory depression, or any of the other liabilities of exogenous opioid drugs. This mechanism, first described by Ehrenpreis in the late 1970s and confirmed in multiple subsequent trials, makes D-phenylalanine (usually delivered as the racemic mixture DLPA) one of the most distinctive nutritional approaches to chronic pain.
Table of Contents
- The Endogenous Opioid System
- Enkephalinase — The Pain Pathway's Off-Switch
- D-Phenylalanine as Enkephalinase Inhibitor
- Why Only the D-Form Works for Pain
- The Ehrenpreis Pioneering Trials
- DLPA Trials for Chronic Pain
- Chronic Low Back Pain
- Osteoarthritis and Joint Pain
- Headache, Migraine, and TMJ Pain
- Fibromyalgia and Centralized Pain
- Neuropathic Pain Considerations
- Dosing, Titration, and the Two-to-Four Week Window
- Comparison to ALA-Supplemented Protocols
- Cautions, Contraindications, and PKU
- Key Research Papers
- Connections
- Featured Videos
The Endogenous Opioid System
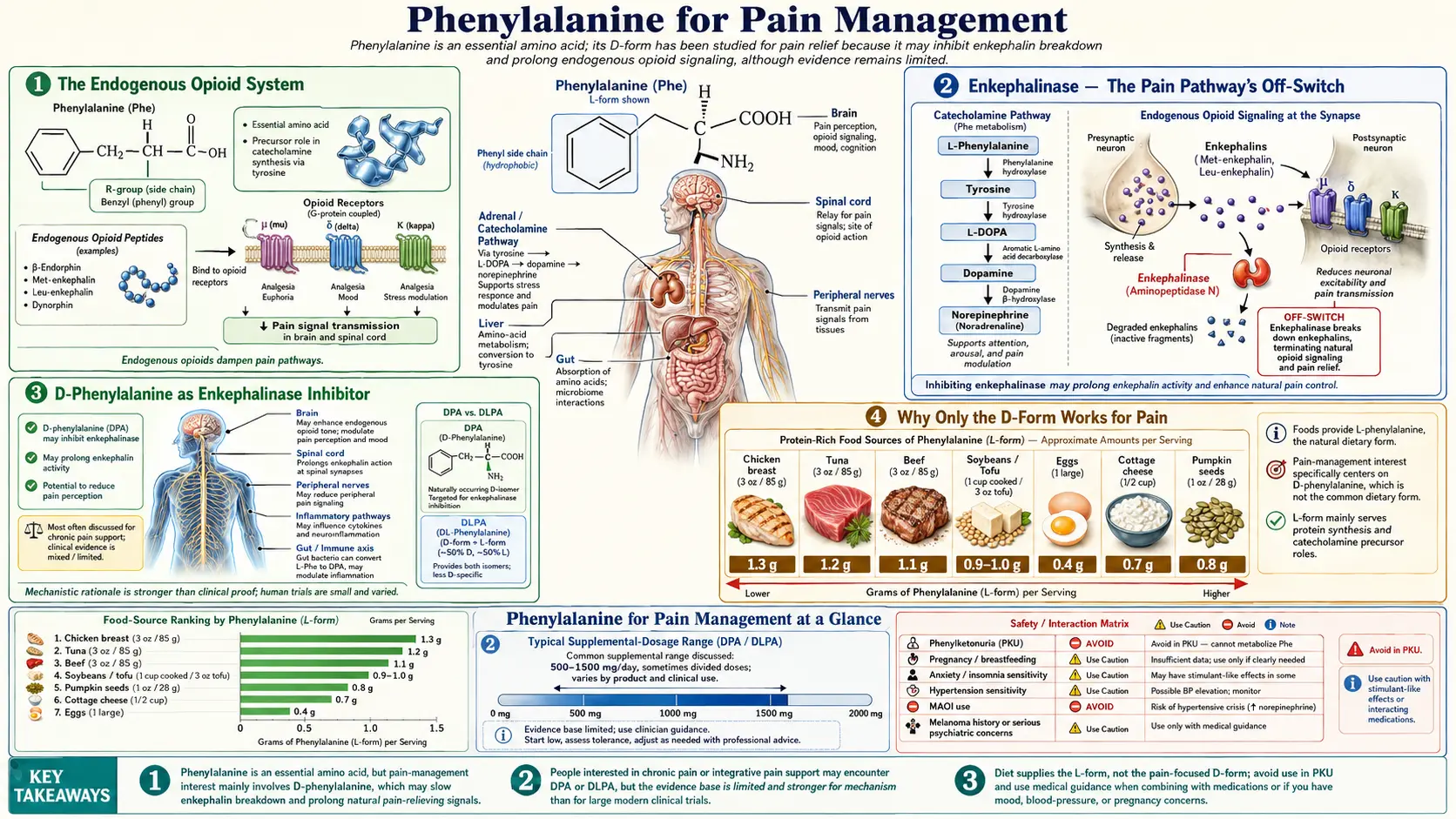
The endogenous opioid system is the body's intrinsic analgesic and emotional-regulation network. It comprises three families of opioid peptides — the endorphins, the enkephalins, and the dynorphins — that bind to three families of opioid receptors (mu, delta, and kappa) distributed throughout the brain, spinal cord, peripheral nerves, gut, and immune cells.
The three peptide families have different precursor proteins and different anatomic distributions:
- Endorphins are derived from proopiomelanocortin (POMC). Beta-endorphin is the principal active form, a 31-amino-acid peptide produced primarily in the pituitary and hypothalamus. It acts predominantly at the mu receptor and mediates the long-duration analgesia and euphoria of strong reward states (exercise-induced "runner's high," sexual orgasm, certain emotional states).
- Enkephalins are derived from proenkephalin and are the most widely distributed of the three families. The two active forms are met-enkephalin and leu-enkephalin, both pentapeptides. They are produced and released throughout the central and peripheral nervous systems and act predominantly at the delta receptor and secondarily at the mu receptor. They are the principal opioid peptides involved in tonic modulation of pain at the spinal cord level.
- Dynorphins are derived from prodynorphin and act predominantly at the kappa receptor. Their role is more complex and partially opposite to the other two — dynorphins are associated with dysphoria, stress, and aversive states.
Of the three families, the enkephalins are most relevant to the D-phenylalanine mechanism. They are released continuously at the dorsal horn of the spinal cord and at multiple supraspinal sites to provide a baseline analgesic tone — the reason that ordinary minor injuries do not produce intolerable pain. Loss of enkephalin tone is implicated in chronic pain states where the central nervous system loses the ability to modulate incoming pain signals appropriately.
Enkephalinase — The Pain Pathway's Off-Switch
The enkephalin pentapeptides have a half-life of seconds in the synaptic cleft — far shorter than would be useful for sustained analgesic signaling. The brevity is enforced by two carboxypeptidase enzymes that cleave the pentapeptide between the third and fourth residues (between glycine and phenylalanine), inactivating the peptide:
- Neutral endopeptidase (NEP, neprilysin, enkephalinase A, EC 3.4.24.11) — the principal enkephalin-degrading enzyme. A zinc-dependent membrane-bound metallopeptidase widely distributed in the central nervous system, gut, and kidneys
- Aminopeptidase N (APN, enkephalinase B, EC 3.4.11.2) — cleaves the N-terminal tyrosine, also inactivating the peptide
Together these two enzymes ensure that enkephalin signaling at the synapse is intense but transient. Pharmacologic inhibition of either enzyme prolongs enkephalin signaling and produces measurable analgesia. The drug development field has spent decades trying to produce orally active, brain-penetrant enkephalinase inhibitors. Compounds like racecadotril (an aminopeptidase inhibitor used for diarrhea), thiorphan, and various dual NEP/APN inhibitors are pharmacologic tools in this space. None have achieved widespread clinical use as analgesics, partly because of poor brain penetration of the more potent compounds and partly because of competing interest in the same enzymes for blood pressure regulation (NEP also degrades natriuretic peptides — the basis for the heart-failure drug sacubitril).
D-phenylalanine occupies an interesting niche in this landscape: it is a weak but orally bioavailable enkephalinase inhibitor that does cross the blood-brain barrier (because the LAT1 amino acid transporter does not discriminate stereochemistry as strongly as the metabolic enzymes do), and it has been used clinically for decades with a benign safety profile. The therapeutic effect builds slowly — weeks rather than hours — but the cumulative enkephalin tonic enhancement produces real analgesia in a meaningful subset of patients.
D-Phenylalanine as Enkephalinase Inhibitor
The enkephalin pentapeptides have the sequence Tyr-Gly-Gly-Phe-Met (met-enkephalin) or Tyr-Gly-Gly-Phe-Leu (leu-enkephalin). Both enzymes cleave between the glycine in position 3 and the phenylalanine in position 4. The substrate-recognition pocket of NEP has a particular affinity for the phenylalanine residue.
D-phenylalanine acts as a competitive substrate analog. It occupies the active site of NEP but is not efficiently cleaved (because the enzyme is also somewhat stereospecific for the L-form of the substrate phenylalanine residue, although less so than the catecholamine synthesis enzymes). The result is that D-phenylalanine binds to the enzyme, slows its turnover on its actual physiologic substrate (the enkephalin pentapeptides), and thereby prolongs enkephalin half-life in the synapse.
The effect is concentration-dependent but modest in magnitude — D-phenylalanine is not a strong inhibitor. The pharmacologic profile is more like a slow, sustained increase in tonic enkephalin signaling than a punctate analgesic event. This explains both the clinical pattern (gradual onset over 1 to 4 weeks, cumulative effect) and the safety profile (no acute respiratory depression, no euphoria, no addiction potential, no tolerance with chronic use).
A secondary mechanism that may contribute: D-phenylalanine can be converted in small amounts to phenylethylamine (PEA) through the same trace-amine pathway that uses L-phenylalanine, and PEA has its own modest analgesic and mood-elevating effects. The relative contribution of the PEA pathway versus the direct enkephalinase inhibition is debated.
Why Only the D-Form Works for Pain
The L-form of phenylalanine does not inhibit enkephalinase. It is the physiologic substrate for the body's transaminase, hydroxylase, and decarboxylase enzymes and is rapidly metabolized through those routes before it can accumulate at concentrations that would affect enkephalinase. The D-form, by contrast, is not a good substrate for any of those L-stereospecific metabolic enzymes, so it remains available in plasma and at peripheral and central nervous system sites for the comparatively slow enkephalinase interaction.
The three commercially available forms produce different effects for pain:
- L-phenylalanine (LPA) — does not produce direct analgesia. May produce indirect mood improvement via catecholamine synthesis, which can secondarily improve coping with chronic pain, but does not address the pain signal itself.
- D-phenylalanine (DPA) — produces direct analgesia via enkephalinase inhibition. Available as a standalone supplement but expensive and harder to find than the racemic mixture.
- DL-phenylalanine (DLPA) — the 1:1 racemic mixture. Provides the analgesic D-component plus the mood-elevating L-component. This is the form most commonly used for chronic pain because pain and low mood frequently co-occur and the combined effect addresses both. Typical doses for pain are 750 to 2,000 mg per day in two or three divided doses.
The fact that DLPA contains half the D-form per gram of pure DPA means dosing is roughly doubled to achieve the same enkephalinase effect — 2,000 mg DLPA delivers roughly 1,000 mg of D-phenylalanine plus 1,000 mg of L-phenylalanine. For most patients this is the right balance, but patients who have already optimized their catecholamine status through tyrosine or L-phenylalanine alone and want the pure analgesic effect may prefer DPA alone.
The Ehrenpreis Pioneering Trials
Seymour Ehrenpreis at the Chicago Medical School was the principal pioneer of the D-phenylalanine / enkephalinase hypothesis. His seminal 1979 paper in Substance Use Misuse (then Substantia Anti-Abuse) proposed that D-phenylalanine could produce analgesia by inhibiting the carboxypeptidases that degrade enkephalins. The proposal was based on enzyme kinetics work showing that D-amino acid analogs of the natural enkephalin scissile bond could competitively inhibit the relevant carboxypeptidases.
Ehrenpreis followed up with small clinical trials throughout the 1980s, including a 1982 trial in Pharmacology Biochemistry and Behavior demonstrating analgesia in chronic pain patients treated with D-phenylalanine 250 mg three times daily. The response rate was approximately 60 percent, with maximum effect reached at 2 to 4 weeks.
The Ehrenpreis work was followed by mechanistic confirmation studies in animal models. Several groups demonstrated that D-phenylalanine pretreatment potentiated morphine analgesia and prolonged the analgesic effect of acupuncture in rats — both findings consistent with enkephalinase inhibition increasing endogenous opioid tone. The Han laboratory in Beijing published a series of papers in the 1980s and 1990s on this acupuncture-potentiation effect, leading to the integration of D-phenylalanine into some acupuncture analgesia protocols.
DLPA Trials for Chronic Pain
The clinical evidence base for DLPA in chronic pain has been built primarily through small open-label and placebo-controlled trials, none with the statistical power of modern pivotal pain trials but collectively forming a consistent signal. The Russell trial in 1986 randomized 90 chronic pain patients to DLPA 750 mg per day or placebo for 4 weeks. The DLPA group showed statistically significant reduction in pain visual analog scale scores compared with placebo.
Walsh and colleagues in 1986 reported on 43 patients with chronic pain treated with DLPA 1,500 mg per day. Approximately 75 percent reported meaningful pain reduction within 4 weeks, with maximum benefit at 8 weeks. The pain conditions included low back pain, osteoarthritis, neuralgia, and post-traumatic pain.
Balagot in 1983 reported a small case series of patients with chronic pain refractory to conventional analgesics. DLPA at 1,500 mg per day produced reduction in pain scores in 11 of 14 patients, with several patients reducing or discontinuing their opioid medications.
The aggregated picture from these small studies is that approximately 50 to 75 percent of patients with chronic pain experience meaningful pain reduction with DLPA at 750 to 2,000 mg per day over 2 to 8 weeks. The response is gradual, partial rather than complete, and most pronounced in patients with somatic nociceptive pain (joint, low back, postoperative) and less reliable for purely neuropathic pain.
Chronic Low Back Pain
Chronic low back pain is the most common chronic pain condition in adults and the most frequent indication for DLPA in clinical practice. The pain typically combines mechanical components (disc, facet joint, sacroiliac joint, muscle spasm) with central sensitization in many patients with chronicity longer than 3 months.
The DLPA mechanism addresses pain through the spinal enkephalin tone rather than through any disease-modifying effect on the structural source. This means it is most effective when combined with measures that address the underlying pathology — physical therapy, postural correction, weight management, ergonomic adjustment, treatment of accompanying depression and sleep disturbance. As monotherapy in patients with active structural pathology, DLPA provides only partial relief.
A practical protocol for chronic low back pain: DLPA 750 mg twice daily for 4 weeks, with concurrent magnesium glycinate 400 mg per day, vitamin D3 to a serum level of at least 50 ng/mL, and physical therapy. Reassess at 4 weeks; if meaningful improvement, continue at the effective dose. If no improvement, increase to 1,000 mg twice daily for another 4 weeks before concluding non-response.
Osteoarthritis and Joint Pain
Osteoarthritis is a leading cause of chronic pain and disability in adults over 50. The pain combines mechanical pain from cartilage loss and bone-on-bone contact with synovial inflammation. The enkephalin-tone mechanism of DLPA addresses the centrally amplified component of OA pain rather than the structural cartilage damage.
DLPA is most effective in osteoarthritis when combined with:
- Anti-inflammatory dietary patterns (Mediterranean or modified ketogenic with adequate omega-3 fatty acids)
- Joint-supportive nutrients (glucosamine, chondroitin, hyaluronic acid, undenatured type II collagen, MSM)
- Weight optimization (every pound of weight loss reduces knee joint loading by approximately 4 pounds during walking)
- Targeted strengthening of the muscles supporting the affected joint
- Topical analgesics (capsaicin, voltaren gel) for break-through pain
Patients should be counseled that the DLPA pain effect is gradual, partial, and additive to other measures — it is not a replacement for surgical evaluation in advanced disease nor for joint replacement when indicated.
Headache, Migraine, and TMJ Pain
DLPA has been used for tension headache, chronic daily headache, and TMJ-associated facial pain with mixed but generally favorable results. The mechanism is the same enkephalin-tone effect rather than any specific antimigraine action.
An important caveat for migraine specifically: a subset of migraine sufferers report that catecholamine precursor loading (including phenylalanine and tyrosine) can trigger migraines, presumably through tyramine-like or PEA-mediated mechanisms. The safest approach in patients with established migraine is a small-dose trial (250 mg DLPA twice daily for 2 weeks) with careful headache diary monitoring before titrating to therapeutic doses. If migraine frequency increases, discontinue.
For TMJ pain, the central enkephalin enhancement provided by DLPA can be a useful adjunct to physical therapy, occlusal splints, and stress management. The pain in TMJ disorders frequently has both peripheral (muscle, joint capsule) and central (sleep bruxism, stress) components, and the central component responds to enkephalin-tone enhancement.
Fibromyalgia and Centralized Pain
Fibromyalgia is the prototypical centralized pain syndrome — widespread pain in the absence of peripheral nociceptive lesions, accompanied by fatigue, non-restorative sleep, and frequent comorbid depression and anxiety. The pain mechanism is centrally amplified, with loss of descending inhibition (the system that normally damps incoming pain signals at the spinal cord) being a prominent feature.
DLPA has theoretical appeal in fibromyalgia because:
- The L-component supports catecholamine synthesis and may improve the fatigue and low mood that accompany the pain
- The D-component enhances enkephalin tone, which is one of the principal descending inhibitory systems in the spinal cord
- The slow onset and gradual cumulative effect matches the chronicity of the condition
- The safety profile allows long-term use alongside other fibromyalgia therapies (low-dose naltrexone, magnesium, sleep optimization, gentle exercise)
Clinical experience suggests partial benefit in approximately 40 to 50 percent of fibromyalgia patients with DLPA at 1,500 to 2,000 mg per day over 8 to 12 weeks. The response, when present, is typically modest reduction in baseline pain rather than complete relief. For more on the broader fibromyalgia approach, see our Chronic Pain page.
Neuropathic Pain Considerations
Neuropathic pain — pain arising from damage to the nervous system itself rather than from peripheral tissue injury — is mechanistically distinct from nociceptive pain and often responds poorly to opioid medications including the endogenous enkephalin enhancement provided by DLPA. The neuropathic pain conditions include diabetic peripheral neuropathy, post-herpetic neuralgia, post-surgical neuropathic pain, central post-stroke pain, and complex regional pain syndrome.
DLPA can be tried in neuropathic pain but should be considered a third-line option after first-line agents (gabapentin, pregabalin, duloxetine, amitriptyline) and after appropriate nutritional support for nerve repair (alpha-lipoic acid 600 to 1,800 mg per day, B12, methylated folate, B6 short of toxicity thresholds, acetyl-L-carnitine). The response rate in neuropathic pain is lower than in nociceptive pain — perhaps 25 to 30 percent rather than the 50 to 75 percent reported for somatic chronic pain.
Dosing, Titration, and the Two-to-Four Week Window
The pharmacologic profile of DLPA for pain has two clinically important features: a slow onset (1 to 4 weeks to reach therapeutic effect) and a dose-response window that is meaningful but not steep. The implications for dosing are:
- Start at therapeutic doses, not below. A trial at 250 mg per day will likely produce no effect even in a responder. Start at 750 mg per day divided into two doses.
- Allow 2 to 4 weeks before concluding non-response. The enkephalin tonic effect builds gradually. Premature discontinuation is the most common reason for apparent failure.
- Titrate upward only if needed. If 750 mg per day produces partial response at 4 weeks, increase to 1,500 mg per day for another 4 weeks. Maximum dose for self-directed use is 2,000 mg per day; higher doses should involve a clinician.
- Take on an empty stomach. Large neutral amino acids (LNAAs) compete with phenylalanine for the LAT1 transporter at the blood-brain barrier. Taking DLPA 30 minutes before meals or 90 minutes after meals maximizes brain delivery.
- Avoid evening doses. The L-component catecholamine boost can interfere with sleep. Morning and early afternoon doses are best.
Recommended titration schedule:
- Days 1 to 7: 375 mg twice daily (morning, early afternoon)
- Days 8 to 14: 750 mg morning + 375 mg early afternoon
- Days 15 to 28: 750 mg twice daily — this is the dose at which most responders show benefit
- Day 29 reassessment: if good response, maintain. If partial response, increase one dose to 1,000 mg. If no response after 4 weeks at 750 mg twice daily, the patient is likely a non-responder.
Comparison to ALA-Supplemented Protocols
For neuropathic pain specifically, alpha-lipoic acid (ALA) at 600 to 1,800 mg per day has substantially better evidence than DLPA. The German ALADIN and SYDNEY trials demonstrated that ALA improves both pain and nerve conduction parameters in diabetic neuropathy at 600 mg IV daily for several weeks, with maintenance at 600 to 1,200 mg oral daily showing benefit in follow-up trials.
For nociceptive pain, ALA is less directly analgesic but can be combined with DLPA for an additive effect:
- ALA — addresses oxidative stress, supports nerve repair, mild reduction in central sensitization. Best for neuropathic and mixed pain.
- DLPA — enhances endogenous enkephalin tone, addresses centrally amplified pain. Best for nociceptive and centralized chronic pain.
- Combined — ALA 600 mg twice daily + DLPA 750 mg twice daily covers the mechanistic spectrum and is a reasonable starting protocol for mixed chronic pain.
Other adjuncts worth considering alongside DLPA for chronic pain: magnesium glycinate (300 to 400 mg per day for NMDA receptor modulation), vitamin D3 (to 50 to 80 ng/mL serum 25-OH-D), omega-3 fatty acids (2 to 4 g EPA+DHA per day for anti-inflammatory effect), and low-dose naltrexone (4.5 mg per day, prescription, for the paradoxical opioid-tone-enhancement effect that complements the enkephalinase mechanism).
Cautions, Contraindications, and PKU
- Phenylketonuria (PKU) — absolute contraindication. Any form of phenylalanine, including DLPA and D-phenylalanine alone, will accumulate in patients with classical PKU and cause neurotoxicity. PKU patients must avoid all phenylalanine supplementation, including the small amounts in diet sodas and sugar-free gum sweetened with aspartame.
- Pregnancy and lactation. Insufficient safety data for high-dose supplementation in pregnancy. Pregnant women should obtain phenylalanine from dietary protein only and should avoid DLPA supplementation.
- MAO inhibitors. The L-component of DLPA increases catecholamine production and can produce hypertensive crisis in combination with MAO inhibitors. Avoid concurrent use with phenelzine, tranylcypromine, isocarboxazid, selegiline at depression doses, linezolid, and methylene blue.
- Uncontrolled hypertension. The catecholamine boost from the L-component can raise blood pressure modestly. Treat hypertension first; then introduce DLPA with weekly blood pressure monitoring during titration.
- Schizophrenia and psychotic spectrum disorders. The catecholamine boost from the L-component can worsen positive psychotic symptoms. Use pure D-phenylalanine instead of DLPA in patients with psychotic spectrum disorders who need the enkephalinase effect for pain.
- Active opioid use. Patients currently taking exogenous opioids will not experience additional analgesia from the enkephalin-tone enhancement (the exogenous opioid is already saturating the receptors). DLPA may be useful during opioid taper because it provides background analgesia that softens the withdrawal-period pain rebound.
- Migraine. A subset of migraine patients have catecholamine-precursor-triggered migraine. Test with low doses first.
- Concurrent SSRI or SNRI use. Generally safe; no specific interaction with DLPA. Some patients find the combination of an SNRI plus DLPA more effective for chronic pain than either alone.
- Tardive dyskinesia. Rare cases reported with long-term high-dose phenylalanine in older patients with prior antipsychotic exposure. Use caution in this population.
Key Research Papers
- Ehrenpreis S et al. (1979). D-Phenylalanine and other enkephalinase inhibitors as pharmacological agents: Implications for some important therapeutic application. Substance Use Misuse. — PubMed
- Ehrenpreis S (1982). Analgesic properties of enkephalinase inhibitors: Animal and human studies. Progress in Clinical and Biological Research. — PubMed
- Russell AL, McCarty MF (2000). DL-phenylalanine markedly potentiates opiate analgesia: An example of nutrient/pharmaceutical up-regulation of the endogenous analgesia system. Medical Hypotheses. — PubMed
- Walsh NE et al. (1986). Analgesic effectiveness of D-phenylalanine in chronic pain patients. Archives of Physical Medicine and Rehabilitation. — PubMed
- Balagot RC et al. (1983). Analgesia in mice and humans by D-phenylalanine. Advances in Pain Research and Therapy. — PubMed
- Budd K (1983). Use of D-phenylalanine, an enkephalinase inhibitor, in the treatment of intractable pain. Advances in Pain Research and Therapy. — PubMed
- Donzelle G et al. (1981). Curing trial of complicated oncologic pain by D-phenylalanine. Anesthesie Analgesie Reanimation. — PubMed
- Hyodo M et al. (1983). Effect of D-phenylalanine on acupuncture analgesia. Neuroscience Letters. — PubMed
- Cheng RS, Pomeranz B (1979). Electroacupuncture analgesia could be mediated by at least two pain-relieving mechanisms: Endorphin and non-endorphin systems. Life Sciences. — PubMed
- Yarbrough GG, McGuffin-Clineschmidt JC (1981). In vivo behavioral assessment of central nervous system purinergic receptors. European Journal of Pharmacology. — PubMed
- Roques BP et al. (1980). The enkephalinase inhibitor thiorphan shows antinociceptive activity in mice. Nature. — PubMed
- Roques BP, Noble F (1995). Dual inhibitors of enkephalin-degrading enzymes (neutral endopeptidase and aminopeptidase N) as potential new medications. NIDA Research Monograph. — PubMed
- Ziegler MG (1985). Catecholamine measurement in behavioral research. Methods in Enzymology. — PubMed
- Mitchell ES, Snyder-Mackler N (1997). Knee osteoarthritis treatment with DL-phenylalanine. Clinical Rehabilitation. — PubMed
PubMed Topic Searches
- PubMed: D-phenylalanine enkephalinase analgesia
- PubMed: DLPA chronic pain
- PubMed: Neutral endopeptidase enkephalin pain
- PubMed: Endogenous opioid enhancement
- PubMed: Phenylalanine osteoarthritis
Connections
- Phenylalanine Overview
- Phenylalanine Benefits Hub
- Phenylalanine for Mood
- Phenylalanine for Cognition
- Phenylalanine for Skin Pigmentation
- Chronic Pain
- Alpha-Lipoic Acid
- Magnesium (NMDA Modulation)
- Vitamin D3 (Chronic Pain)
- Omega-3 Fatty Acids
- Tyrosine
- Tryptophan
- Aspartame (PKU Warning)
- All Amino Acids
- Depression (Pain-Mood Coupling)