Glycine for Glutathione Synthesis
Glutathione (gamma-glutamyl-cysteinyl-glycine, abbreviated GSH) is the body's master intracellular antioxidant, a tripeptide synthesized in nearly every cell from three amino acids: glutamate, cysteine, and glycine. For decades, cysteine was treated as the sole rate-limiting precursor — the basis for the widespread use of N-acetylcysteine (NAC) as a glutathione precursor in clinical and supplement settings. The Sekhar laboratory at Baylor College of Medicine has dismantled that simpler view across a sequence of trials from 2011 through 2023, demonstrating that both cysteine and glycine become rate-limiting in older adults, in diabetics, in HIV-positive patients, and in others with chronic glutathione deficits — and that the combined "GlyNAC" supplementation of glycine plus N-acetylcysteine restores glutathione levels, reduces oxidative stress markers, improves mitochondrial function, lowers inflammation, improves insulin sensitivity, increases muscle strength, and improves cognitive function in ways that cysteine alone does not match. This deep-dive walks through the biochemistry, the trial sequence, the mitochondrial connection, and the practical dosing.
Table of Contents
- Three Amino Acids, Two Rate-Limiting Steps
- Why Glycine Was Overlooked for So Long
- The Sekhar GlyNAC Research Program (2011–2023)
- The Aging Glutathione Deficit
- Mitochondrial Dysfunction and Oxidative Stress
- GlyNAC and the Hallmarks of Aging
- Diabetes, HIV, and Other Chronic-Disease Populations
- NAC Alone vs Glycine Alone vs GlyNAC Combined
- Dose, Form, and Protocol
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
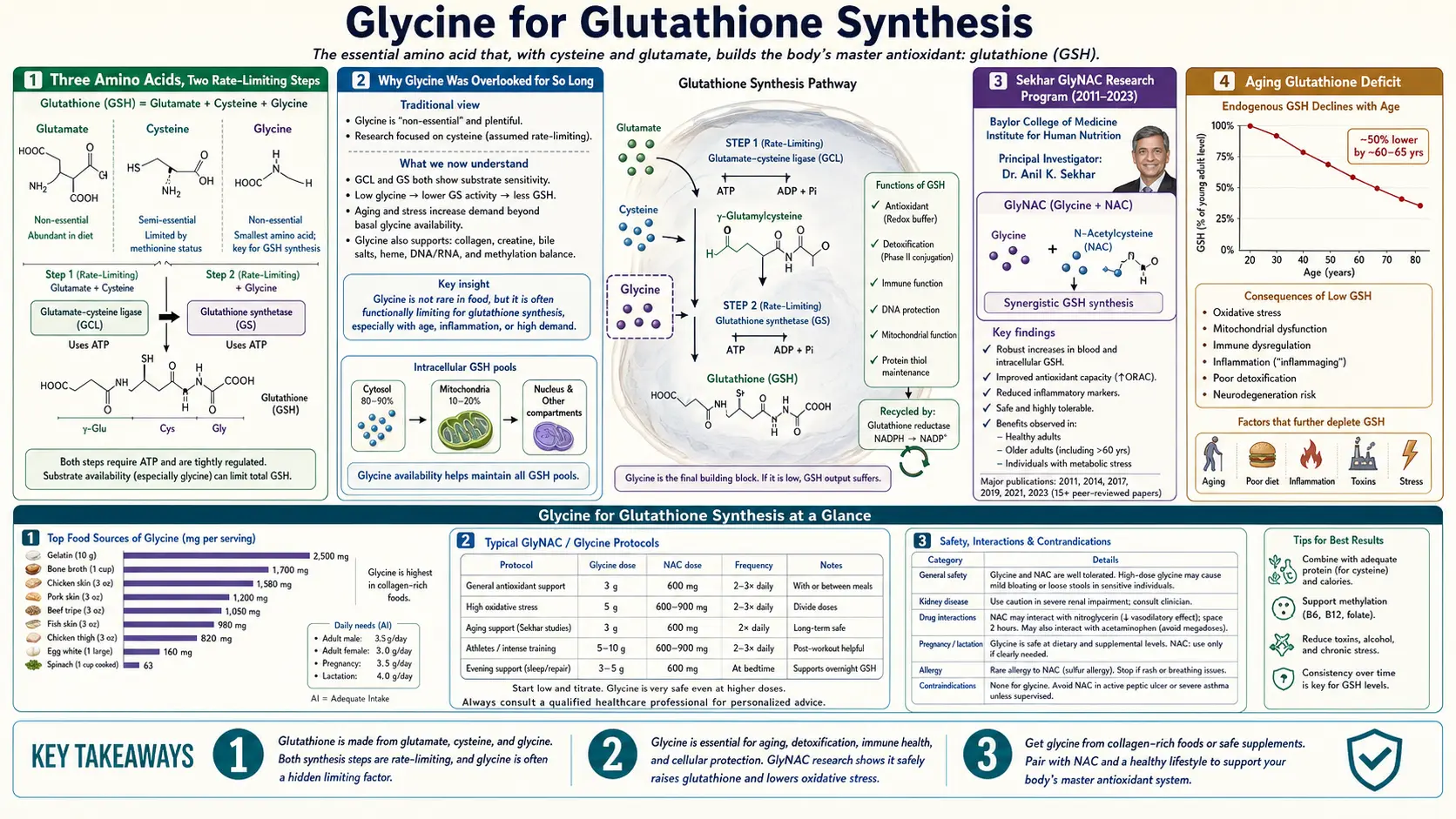
Three Amino Acids, Two Rate-Limiting Steps
Glutathione (GSH) is synthesized intracellularly in a two-step ATP-dependent process:
- Step 1. Glutamate-cysteine ligase (GCL, also called gamma-glutamylcysteine synthetase) joins glutamate to cysteine via an unusual gamma-peptide bond, producing gamma-glutamyl-cysteine (gamma-GC). This is the canonical rate-limiting step and the target of feedback inhibition by GSH itself. GCL has high affinity for both glutamate and cysteine but is normally substrate-limited by cysteine, which is the least abundant of the three amino acids in most tissues.
- Step 2. Glutathione synthetase (GS) joins gamma-GC to glycine via a conventional alpha-peptide bond, producing the final tripeptide glutathione. Glutathione synthetase has high Vmax and is not typically considered rate-limiting under normal conditions.
The conventional textbook account stops there: cysteine is rate-limiting, glycine is "abundant," and the way to support GSH synthesis is to provide cysteine in a stable bioavailable form — usually N-acetylcysteine (NAC), the acetylated derivative that survives oral absorption and is rapidly deacetylated to cysteine intracellularly.
The Sekhar work showed that the textbook account is incomplete for a large and important subset of patients. In older adults, in type 2 diabetics, in HIV-positive patients, and in other chronic-disease states characterized by glutathione deficiency, plasma and red-blood-cell glycine concentrations are also reduced, and supplying cysteine alone does not fully restore GSH because the second step of synthesis is then operating below its glycine Km. Providing both substrates together restores GSH; providing either alone provides only a partial restoration.
Why Glycine Was Overlooked for So Long
The historical neglect of glycine as a glutathione precursor traces to two assumptions, both reasonable in the era they were made and both partially wrong:
Assumption 1: Glycine is abundant. Glycine is the smallest amino acid, is present in almost all dietary proteins to some degree, and the body can synthesize it from serine, threonine, and choline. The textbook conclusion was that glycine supply could not realistically become rate-limiting under normal physiological conditions. As the Meléndez-Hevia and McCarty analysis (covered on the Collagen Synthesis page) demonstrated, the abundance assumption fails when one totals the demand from collagen turnover, glutathione synthesis, creatine synthesis, heme synthesis, bile-acid conjugation, and phase II detoxification — the sum is well above what dietary plus endogenous supply can deliver.
Assumption 2: The second enzyme is not rate-limiting. In vitro, glutathione synthetase has higher Vmax than glutamate-cysteine ligase, which by classical analysis means the first enzyme is rate-limiting. But this analysis assumes both substrates are saturating. When cellular glycine drops below the Km of glutathione synthetase (~1 mM), the second enzyme's effective rate falls and it can become co-rate-limiting with the first.
The Sekhar 2011 Diabetes Care paper was the first to demonstrate the implication directly in patients: type 2 diabetics had reduced red-blood-cell glutathione, reduced GCL and GS enzyme activity, and reduced plasma glycine. Supplementation with cysteine plus glycine for 14 days restored both enzyme activities and restored RBC glutathione to healthy-control levels. Cysteine alone in earlier studies had not produced equivalent restoration. The conclusion was that both precursors were rate-limited in the diabetic state, not just cysteine.
The Sekhar GlyNAC Research Program (2011–2023)
Rajagopal V. Sekhar at Baylor College of Medicine has led a decade-plus research program on glutathione restoration in aging and chronic disease. The signature contribution is the "GlyNAC" combination — oral glycine plus N-acetylcysteine in approximately equimolar doses, administered daily for weeks to months. The major published studies, in roughly chronological order:
- Sekhar et al. 2011, Diabetes Care. 12 type 2 diabetic patients vs 8 healthy controls. Cysteine + glycine supplementation for 2 weeks restored RBC glutathione, reduced oxidative stress markers (TBARS, F2-isoprostanes), and restored GCL and GS enzyme activities.
- Nguyen et al. 2013, Aging Cell. 8 older adults (60–75 years) vs 8 young controls (21–30 years). 2 weeks of cysteine + glycine supplementation in older adults restored RBC glutathione to young-control levels and reduced oxidative stress markers.
- Sekhar et al. 2015, AIDS. HIV-positive patients on suppressive antiretroviral therapy showed glutathione deficiency that was corrected with 14 days of cysteine + glycine supplementation, with improvements in mitochondrial fuel oxidation and physical function.
- Kumar et al. 2018 / 2020, Clinical and Translational Medicine. Pilot trial extending GlyNAC supplementation in older adults to 24 weeks, demonstrating improvements in muscle strength, exercise capacity, cognition, mitochondrial fuel oxidation, gait speed, glucose metabolism, insulin sensitivity, and waist circumference, alongside the expected glutathione restoration and oxidative-stress reduction.
- Kumar et al. 2021, Clinical and Translational Medicine. Open-label confirmation in additional older adults; reported improvements in 9 of 9 measured hallmarks of aging.
- Sekhar 2022, Nutrients. Comprehensive review of the GlyNAC mechanism and clinical outcomes across the trial program.
- Kumar et al. 2023, Clinical and Translational Medicine (RCT). The largest and most rigorous study to date — a 16-week randomized placebo-controlled trial in older adults demonstrating significant improvements in oxidative stress markers, mitochondrial function, insulin resistance, endothelial function, genotoxicity (DNA damage), inflammation, muscle strength, gait speed, exercise capacity, and cognitive function on a battery of standard tests, compared to placebo.
The 2023 RCT is the keystone — the first formally randomized placebo-controlled trial of GlyNAC in aging, and the first to demonstrate the broad multi-system improvements that the earlier open-label and crossover work had hinted at. It also established the broader clinical relevance of the approach beyond proof-of-concept biochemistry.
The Aging Glutathione Deficit
Glutathione concentrations decline with age across multiple tissues. In red blood cells, glutathione concentrations in a typical 70-year-old are roughly 40–50% lower than in a typical 25-year-old. Liver and brain show parallel reductions, although these are harder to measure directly in living humans. The decline tracks with rising markers of oxidative damage to lipids, proteins, and DNA, and with the mitochondrial dysfunction that contributes to age-related sarcopenia, neurodegeneration, and metabolic decline.
The Sekhar Nguyen 2013 paper measured the upstream substrate flows directly. Older adults had:
- Reduced plasma cysteine (~30% lower than young controls)
- Reduced plasma glycine (~25% lower than young controls)
- Reduced GCL and GS enzyme activities in red blood cells
- Reduced glutathione synthesis rate measured by isotope dilution
Two weeks of cysteine + glycine supplementation restored the synthesis rate to young-control levels and restored absolute RBC glutathione to within 10% of young-control levels. Either nutrient alone in earlier work had not produced this magnitude of restoration.
The interpretation is that aging produces a coordinated substrate-deficit state — not simply lower antioxidant defense, but lower precursor availability for the antioxidant defense system. Correcting the substrate deficit is sufficient to restore the antioxidant capacity, at least over the months of intervention studied.
Mitochondrial Dysfunction and Oxidative Stress
Mitochondria are the primary intracellular source of reactive oxygen species. The electron transport chain leaks roughly 1–3% of the electrons passing through complex I and complex III directly to molecular oxygen, generating superoxide that is dismutated to hydrogen peroxide. Hydrogen peroxide is then detoxified by the catalase or glutathione peroxidase systems — the latter using reduced glutathione as the electron donor.
When intracellular glutathione drops, hydrogen peroxide and its downstream products (hydroxyl radical, lipid peroxides, oxidized proteins) accumulate. The mitochondrial inner membrane itself becomes a target — oxidation of cardiolipin disrupts respiratory-chain organization, and oxidation of mitochondrial DNA accumulates damage that the limited mitochondrial repair machinery cannot fully address. The result is a feed-forward cycle: lower glutathione → more oxidative damage → impaired mitochondrial function → more electron leak → more oxidative damage.
The GlyNAC trials measured mitochondrial function with isotope-dilution glucose and palmitate oxidation, and reported significant improvements in fuel oxidation following 16–24 weeks of supplementation in older adults. The 2023 RCT also documented:
- Reduced 8-hydroxy-2'-deoxyguanosine (a marker of oxidative DNA damage)
- Reduced F2-isoprostanes (a marker of lipid peroxidation)
- Reduced TBARS (thiobarbituric-acid-reactive substances)
- Reduced markers of inflammation (TNF-alpha, IL-6, hs-CRP)
- Improved insulin sensitivity by HOMA-IR
- Improved endothelial function (flow-mediated dilation)
- Improved muscle strength (grip strength, leg extension)
- Improved gait speed and 6-minute walk distance
- Improvements on cognitive tests
The breadth of the improvements supports the hypothesis that mitochondrial oxidative stress is upstream of many of the apparent independent declines of aging — correcting the antioxidant substrate deficit improves all of them in parallel.
GlyNAC and the Hallmarks of Aging
In the now-classic "Hallmarks of Aging" framework first proposed by Lopez-Otin and colleagues in 2013 (updated 2023), nine to twelve interrelated cellular and molecular processes are proposed as the core drivers of aging:
- Genomic instability
- Telomere attrition
- Epigenetic alterations
- Loss of proteostasis
- Disabled macroautophagy
- Deregulated nutrient sensing
- Mitochondrial dysfunction
- Cellular senescence
- Stem cell exhaustion
- Altered intercellular communication
- Chronic inflammation
- Dysbiosis
The Kumar 2021 paper argued that GlyNAC supplementation in older adults measurably improved markers across 9 of these hallmarks in their cohort — particularly the directly oxidative-stress-related ones (genomic instability via DNA-damage markers, mitochondrial dysfunction, chronic inflammation, deregulated nutrient sensing via insulin sensitivity), but extending to others through downstream effects. The claim should be read with appropriate caution — the trial cohorts are small, the markers used are imperfect, and "hallmark improvement" can be defined more or less inclusively — but the framework is consistent with the broad multi-system improvements documented in the 2023 RCT.
Whether this translates into longer healthspan or lifespan in humans cannot be demonstrated in any 16- or 24-week trial. The mechanistic story and the biomarker improvements are strong; the hard outcome data on hospitalization, disability, or mortality will require multi-year or decade-long follow-up.
Diabetes, HIV, and Other Chronic-Disease Populations
Beyond the aging cohort, the Sekhar group has documented glutathione deficiency and GlyNAC response in several specific patient populations:
- Type 2 diabetes (Sekhar 2011). Diabetics had reduced RBC glutathione, increased oxidative stress, and lower plasma glycine and cysteine compared to healthy controls. 2 weeks of cysteine + glycine restored glutathione and reduced oxidative stress markers. This is consistent with the broader epidemiologic finding of low circulating glycine in metabolic syndrome and type 2 diabetes (covered on the main Glycine page).
- HIV infection on suppressive ART (Sekhar 2015, Nguyen 2014). HIV-positive patients on effective antiretroviral therapy have persistent glutathione deficiency despite undetectable viral load. GlyNAC supplementation restored glutathione and improved mitochondrial fuel oxidation and physical performance. The mechanism likely combines chronic immune activation, mitochondrial toxicity of older ART regimens, and the broader inflammatory state.
- Obesity. Several studies have documented reduced glutathione and elevated oxidative stress in obesity, with response to GlyNAC paralleling the diabetic data.
- Genetic disorders of glutathione metabolism. Patients with hereditary deficiency of glutathione synthetase have used glycine supplementation as part of management. Patients with other rare disorders of sulfur amino acid metabolism may benefit from individualized protocols.
- Pulmonary fibrosis and COPD. NAC is used as a glutathione precursor in some lung disease settings; whether adding glycine improves the response has not been definitively tested but is biologically plausible.
The cross-population pattern is consistent: chronic-disease and aging states produce a substrate-deficient glutathione system, and replacing both glycine and cysteine substrates is the most effective restoration strategy.
NAC Alone vs Glycine Alone vs GlyNAC Combined
The practical question for patients and clinicians: if the goal is to restore glutathione, is the GlyNAC combination meaningfully better than NAC alone (which has decades of clinical history) or glycine alone (which is cheap and well-tolerated)?
NAC alone raises intracellular cysteine, which raises GCL flux and produces some increase in glutathione — particularly in acute settings where cysteine is the dominant rate-limiting factor (acetaminophen overdose, where NAC remains the standard antidote, exploits exactly this). In chronic aging and chronic-disease settings, however, NAC alone produces a partial response that plateaus below the level achievable with the combination.
Glycine alone raises intracellular glycine, which provides substrate for the second enzymatic step. But without simultaneous cysteine supply, the first step remains rate-limited and the second step has nothing to act on. Glycine alone therefore produces little change in glutathione in cysteine-replete subjects, and modest improvement in subjects whose primary deficit is glycine.
GlyNAC combination simultaneously addresses both rate-limiting steps. The Sekhar trials consistently show that the combination produces glutathione restoration that exceeds what either nutrient alone delivers.
The pragmatic implication: for an older adult, a diabetic, or anyone in a chronic-oxidative-stress state, the combination is the rational choice. For a young healthy adult with no specific glutathione concern, supplementation may be unnecessary entirely. For acute acetaminophen overdose, NAC alone remains the standard.
Dose, Form, and Protocol
The Sekhar trial doses were calculated by body weight:
- Glycine: 100 mg per kg body weight per day
- N-acetylcysteine: 100 mg per kg body weight per day
For a 70 kg (155 lb) adult, this works out to approximately 7 g of glycine plus 7 g of NAC daily. The standard protocol was to split the dose — half in the morning and half in the evening, taken with food — to maintain more consistent plasma levels through the day. Capsule form is the most studied; powder form mixed in water is equivalent for absorption but requires accurate scale measurement.
The intervention duration in the most successful trials was 16–24 weeks. Some biomarker improvements (glutathione level, oxidative stress markers, insulin sensitivity) appear within 2–4 weeks. Other improvements (muscle strength, cognitive measures, mitochondrial fuel oxidation) take longer to develop and continue to improve through the trial duration. There is no published evidence on what happens after the intervention is discontinued, but parallel data from collagen and other amino-acid interventions suggest the benefits regress within months of stopping.
Some practitioners use modified, lower-dose protocols (e.g., 3 g glycine plus 1.2 g NAC daily) as long-term maintenance for older adults who tolerate the full-dose protocol initially but want a sustainable dose for chronic use. There is no rigorous trial data on the lower doses but the substrate logic suggests at least some sustained benefit.
NAC is well-absorbed but has a sulfurous smell and taste. Some users prefer "NACET" (N-acetylcysteine ethyl ester) for better tolerance, though there is less clinical data on the ester form. Liposomal NAC formulations are marketed as having higher bioavailability but the trial evidence is limited.
Glycine is sweet-tasting and very well tolerated. Powder is the cheapest form. The combined GlyNAC dose at 7 g + 7 g is approximately 14 g of powder daily, which is sizable but manageable in two split doses dissolved in water with juice to mask the NAC sulfur note.
Cautions and Drug Interactions
- Clozapine. The one clinically important drug interaction with glycine. Glycine antagonizes the antipsychotic effect of clozapine specifically. Patients on clozapine should not supplement glycine.
- NAC and nitroglycerin. NAC potentiates the vasodilatory effect of nitroglycerin and may cause headache or hypotension if combined.
- NAC and certain chemotherapy. NAC has been used to reduce ototoxicity of cisplatin and other chemotherapy regimens, but in some experimental settings it may attenuate the anti-tumor effect of pro-oxidant chemotherapy or radiation. Patients on active cancer treatment should discuss NAC timing with their oncologist.
- Anticoagulants. NAC has mild antiplatelet effects; patients on warfarin or DOACs should be aware but the effect is small.
- Severe asthma. Bronchospasm has been reported rarely with high-dose IV NAC; oral NAC is generally safe in asthmatics but caution at high doses.
- Pregnancy. Glycine is safe in pregnancy at dietary doses. The high-dose Sekhar protocol has not been studied in pregnancy and conservative practice avoids it.
- GI tolerance. Loose stools or mild nausea at the upper end of the dose range; usually resolves by splitting the dose or taking with food.
- Hereditary glycine encephalopathy. Contraindicated as discussed elsewhere on the site.
Key Research Papers
- Sekhar RV, McKay SV, Patel SG, et al. (2011). Glutathione synthesis is diminished in patients with uncontrolled diabetes and restored by dietary supplementation with cysteine and glycine. Diabetes Care. — PubMed
- Nguyen D, Hsu JW, Jahoor F, Sekhar RV (2013). Effect of increasing glutathione with cysteine and glycine supplementation on mitochondrial fuel oxidation, insulin sensitivity, and body composition in older HIV-infected patients. Journal of Clinical Endocrinology and Metabolism. — PubMed
- Sekhar RV, Patel SG, Guthikonda AP, et al. (2011). Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. American Journal of Clinical Nutrition. — PubMed
- Kumar P, Liu C, Hsu JW, et al. (2021). GlyNAC supplementation improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition in older adults: a randomized clinical trial. Clinical and Translational Medicine. — PubMed
- Kumar P, Osahon OW, Sekhar RV (2022). GlyNAC (Glycine and N-Acetylcysteine) supplementation in old mice improves brain glutathione deficiency, oxidative stress, glucose uptake, mitochondrial dysfunction, and cognitive impairment. Antioxidants. — PubMed
- Kumar P, Osahon OW, Sekhar RV (2023). Reversing aged hallmarks in older humans with GlyNAC supplementation. Clinical and Translational Medicine. — PubMed
- Sekhar RV (2022). GlyNAC supplementation improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, aging hallmarks, metabolic defects, muscle strength, cognitive decline, and body composition: implications for healthy aging. Journal of Nutrition. — PubMed
- McCarty MF, O'Keefe JH, DiNicolantonio JJ (2018). Dietary glycine is rate-limiting for glutathione synthesis and may have broad potential for health protection. Ochsner Journal. — PubMed
- Meléndez-Hevia E, De Paz-Lugo P, Cornish-Bowden A, Cárdenas ML (2009). A weak link in metabolism: the metabolic capacity for glycine biosynthesis does not satisfy the need for collagen synthesis. Journal of Biosciences. — PubMed
- Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G (2013). The hallmarks of aging. Cell. — PubMed
- Lopez-Otin C, Blasco MA, Partridge L, Serrano M, Kroemer G (2023). Hallmarks of aging: an expanding universe. Cell. — PubMed
- Mosharov E, Cranford MR, Banerjee R (2000). The quantitatively important relationship between homocysteine metabolism and glutathione synthesis by the transsulfuration pathway and its regulation by redox changes. Biochemistry. — PubMed
- Lu SC (2013). Glutathione synthesis. Biochimica et Biophysica Acta. — PubMed
PubMed Topic Searches
- PubMed: GlyNAC clinical trials
- PubMed: glutathione and aging
- PubMed: cysteine + glycine in diabetes
- PubMed: NAC as glutathione precursor
- PubMed: mitochondrial oxidative stress
Connections
- Glycine Overview
- Glycine Benefits Hub
- Glycine for Sleep and Relaxation
- Glycine for Collagen Synthesis
- Glycine and Aspirin Metabolism
- Cysteine
- Methionine
- Glutamic Acid
- NAC (N-Acetylcysteine)
- NAC and Glutathione
- Glutathione
- Oxidative Stress
- Anti-Aging
- Type 2 Diabetes
- Metabolic Syndrome
- Bone Broth
- Collagen
- Vitamin B6 (P5P)
- Folate
- Selenium (GPX cofactor)
- All Amino Acids