N-acetyl-cysteine (NAC) and Lung Health (Cysteine Benefits)
N-acetylcysteine (NAC) was first synthesized in the 1950s as an acetylated prodrug of cysteine, originally developed as a mucolytic agent — an inhaled solution that could break disulfide bonds in airway mucus and thin the secretions of patients with chronic bronchitis and cystic fibrosis. Two unexpected clinical roles followed. In 1974 the Rumack-Matthew nomogram established oral and IV NAC as the definitive antidote for acetaminophen overdose, regenerating hepatic glutathione before the toxic metabolite NAPQI can destroy hepatocytes — this single use case made NAC one of the most widely stocked drugs in emergency medicine worldwide. Then in the 2000s the IFIGENIA trial in idiopathic pulmonary fibrosis re-opened the question of whether high-dose oral NAC (1800 mg/day) might slow lung scarring — an early positive signal that the larger PANTHER-IPF trial then complicated by finding no benefit in monotherapy and possible harm in combination with prednisone/azathioprine. This deep-dive walks through each lung-health application of NAC: its mucolytic mechanism, the COPD exacerbation literature (BRONCUS, PANTHEON), the IPF saga, the acetaminophen antidote protocol, and the more speculative inhaled-NAC and bronchiectasis evidence.
Table of Contents
- NAC: How an Acetylated Cysteine Becomes a Drug
- Mucolytic Action and Disulfide-Bond Cleavage
- COPD — BRONCUS, PANTHEON, HIACE
- Idiopathic Pulmonary Fibrosis — IFIGENIA and PANTHER
- Acetaminophen Overdose — Rumack-Matthew Protocol
- Bronchiectasis and Chronic Bronchitis
- Cystic Fibrosis
- Asthma (and the Bronchospasm Caution)
- Contrast-Induced Nephropathy
- Inhaled vs Oral NAC
- Practical Dosing for Lung Conditions
- Key Research Papers
- Connections
- Featured Videos
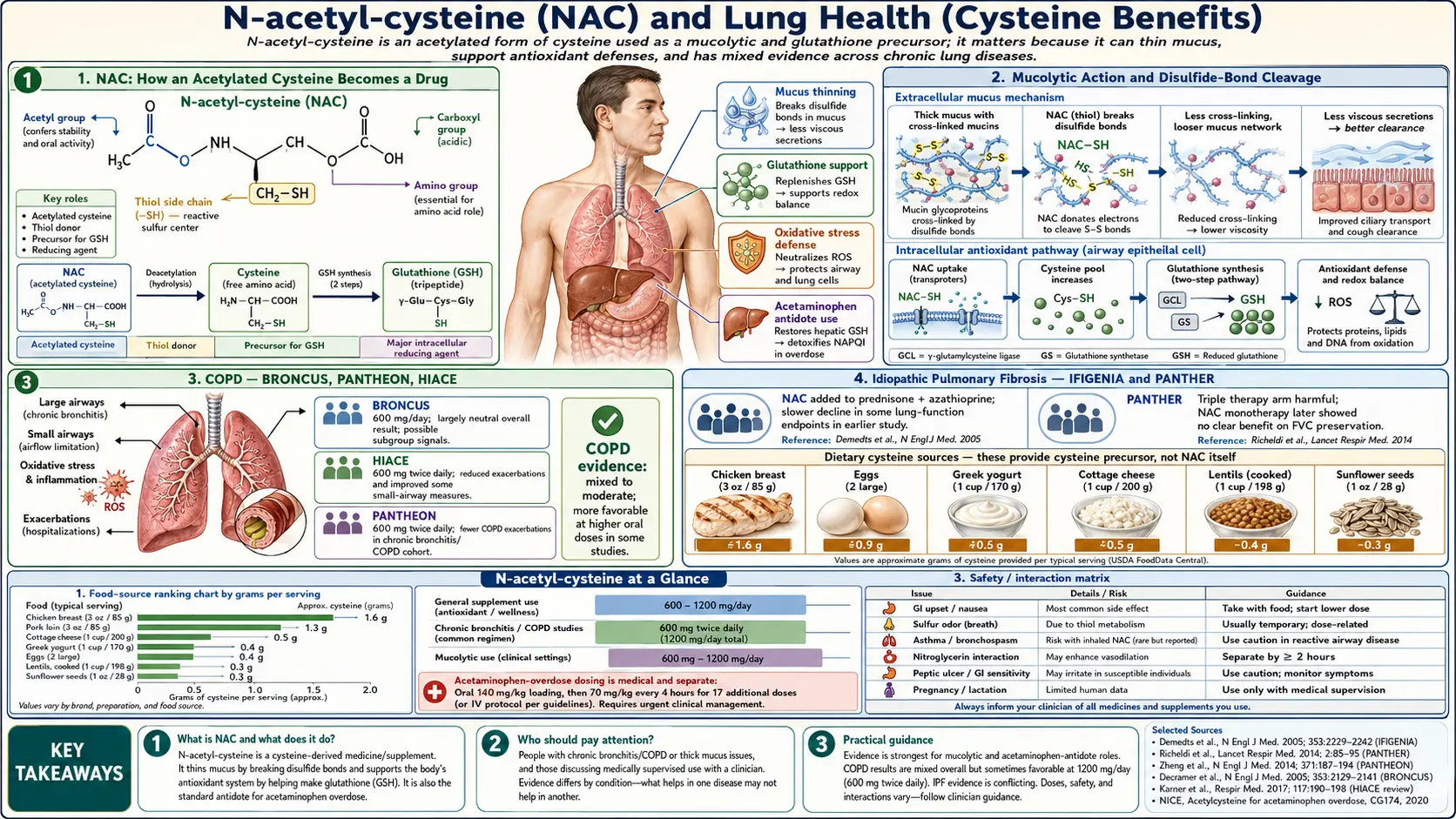
NAC: How an Acetylated Cysteine Becomes a Drug
N-acetylcysteine is L-cysteine with an acetyl group (–COCH3) attached to the alpha-amino nitrogen. The molecular weight is 163 Da. The acetyl group is a simple protecting group: it prevents the free cysteine thiol from auto-oxidizing in the bottle, in the upper gastrointestinal tract, and in plasma. Without it, free cysteine has the storage stability of a wet sparkler and the oral bioavailability of a sugar cube in the rain.
Once NAC reaches the intracellular environment (especially hepatocytes and pulmonary epithelial cells, which express high levels of aminoacylase-1 and other deacylating enzymes), the acetyl group is cleaved to release free L-cysteine. This freed cysteine then enters the glutathione synthesis pathway in the cytosol, where it is joined to glutamate by glutamate-cysteine ligase to form gamma-glutamylcysteine, then to glycine by glutathione synthetase to complete the GSH tripeptide. The released acetic acid is harmlessly oxidized in the citric acid cycle. The net effect of an oral NAC dose is therefore equivalent to delivering a pulse of cysteine to the intracellular GSH-synthesis machinery — with much better stability and absorption than swallowing the same amount of free L-cysteine.
Oral NAC has a complicated pharmacokinetic story. Bioavailability of an oral dose is only about 6-10%, largely because of extensive first-pass hepatic metabolism — the liver grabs and processes most of the absorbed NAC before it reaches systemic circulation. This sounds bad but is actually advantageous for the dominant clinical use of NAC, because the liver is the principal target organ. Pulmonary delivery (inhaled NAC) and IV delivery achieve much higher systemic bioavailability when systemic exposure is needed. Plasma half-life of free cysteine derived from NAC is about 6 hours, which is why oral NAC dosing is typically twice or three times daily.
Beyond its prodrug-to-cysteine role, NAC has a second direct pharmacological effect: the free thiol on cysteine can directly cleave disulfide bonds in extracellular proteins. This is the basis of NAC's mucolytic action, discussed in the next section, and also of its biofilm-disrupting properties used in chronic infection work.
Mucolytic Action and Disulfide-Bond Cleavage
Airway mucus is not just goo — it is a structured gel built around two enormous glycoproteins called MUC5AC and MUC5B (mucins), which assemble into long polymeric chains held together by intermolecular disulfide bonds between cysteine residues in their C-terminal cysteine-rich domains. This disulfide-bonded mucin gel is what gives healthy airway mucus its elasticity (allowing ciliary beat to transport it) and what becomes pathologically thick and immobile in chronic bronchitis, COPD, cystic fibrosis, and severe bronchiectasis.
NAC's free thiol group attacks these mucin disulfide bonds through a thiol-disulfide exchange reaction, breaking the cross-links between mucin polymers and reducing the viscoelasticity of the mucus gel. Thinner, less elastic mucus is more easily cleared by ciliary action and by cough. The mucolytic effect can be demonstrated in vitro within seconds of NAC exposure on sputum samples, and clinically within hours of oral or inhaled administration.
The original inhaled NAC product (Mucomyst, 10% or 20% solution delivered via nebulizer) was approved for this exact purpose — mucolytic adjunct for patients with thick airway secretions. It remains in clinical use, particularly in cystic fibrosis and in post-surgical patients with mucus plugging, though it has been partially displaced in CF by dornase alfa (recombinant DNase, which cleaves the extracellular DNA from dead neutrophils that accumulates in CF mucus and contributes to its viscosity by a different mechanism). The two drugs are complementary — NAC cleaves the mucin disulfide bonds, dornase alfa cleaves the inflammatory DNA — and both are sometimes used together.
Oral NAC also has mucolytic effect, presumably because the delivered cysteine raises pulmonary epithelial-lining-fluid glutathione concentration, which in turn participates in mucin disulfide-bond cycling. The clinical magnitude of oral-NAC mucolytic effect is smaller than direct inhalation but is still measurable as reductions in sputum viscosity, easier expectoration, and reduced cough scores in chronic bronchitis trials.
COPD — BRONCUS, PANTHEON, HIACE
The clinical question in COPD is whether oral NAC reduces exacerbation frequency — the acute symptomatic worsenings that drive hospital admissions, antibiotic use, and steroid courses, and that accelerate the underlying lung-function decline of the disease. Three large trials anchor the evidence.
BRONCUS (Bronchitis Randomized on NAC Cost-Utility Study, 2005) randomized 523 European COPD patients to 600 mg/day NAC or placebo for 3 years. The primary outcome (rate of FEV1 decline) was not different, and the secondary outcome of exacerbation rate showed only a small, non-significant reduction. This was widely interpreted as a negative trial, and Cochrane reviews at the time concluded NAC had no role in COPD prevention.
PANTHEON (Effect of N-acetylcysteine on COPD Exacerbations in China, 2014) challenged that conclusion. PANTHEON randomized 1006 Chinese moderate-to-severe COPD patients to 600 mg twice daily (i.e., 1200 mg/day, double the BRONCUS dose) or placebo for 1 year. The higher-dose group had a 22% reduction in exacerbation rate (1.16 vs 1.49 per patient-year, P<0.001), with the benefit concentrated in patients with more severe baseline disease and more frequent prior exacerbations. The take-away was that 600 mg/day was likely under-dosed and 1200 mg/day was the meaningful dose for COPD exacerbation prevention.
HIACE (High Dose Acetylcysteine in Stable COPD, 2013) separately showed that 600 mg twice daily improved small-airway function (reduced air trapping on lung function testing) compared to placebo in stable COPD over 1 year.
The current GOLD COPD guideline (Global Initiative for Chronic Obstructive Lung Disease) lists NAC as an "add-on therapy in selected patients with moderate-severe COPD and a history of exacerbations" with the qualifier that benefit is most likely in patients not on inhaled corticosteroids. NAC's safety profile, oral availability, and low cost make it a reasonable adjunct in this patient population, particularly for patients on a budget who are still having more than one exacerbation per year despite inhaler therapy.
The mechanistic explanation for NAC's exacerbation-reducing effect is dual: the mucolytic effect improves baseline mucus clearance, reducing bacterial colonization and the trigger for exacerbations; and the GSH-restoring effect reduces the oxidative stress in airway epithelium that potentiates inflammatory cascade activation when an irritant (viral infection, pollution exposure) triggers an exacerbation.
Idiopathic Pulmonary Fibrosis — IFIGENIA and PANTHER
Idiopathic pulmonary fibrosis (IPF) is a progressive, lethal interstitial lung disease in which the alveolar walls fibrose and stiffen, eventually preventing gas exchange. The pathophysiology involves repeated micro-injuries to alveolar epithelium, aberrant repair with fibroblast-myofibroblast activation, and excess collagen deposition. Oxidative stress has been implicated as one of the upstream injury mechanisms, and lung glutathione concentrations in IPF patients are substantially reduced compared to controls — making NAC a mechanistically plausible candidate therapy.
IFIGENIA (2005) was the first large NAC-in-IPF trial. 155 patients were randomized to high-dose oral NAC (600 mg three times daily, 1800 mg/day) plus standard "triple therapy" (prednisone + azathioprine) versus standard triple therapy alone. After 1 year, the NAC arm showed significantly less decline in vital capacity (VC) and diffusion capacity (DLCO). The trial was widely interpreted as positive for NAC, and high-dose NAC entered routine IPF care at many centers.
PANTHER-IPF (2012/2014) was the definitive 3-arm follow-up trial: prednisone + azathioprine + NAC (the IFIGENIA combination) vs NAC monotherapy vs placebo. The first arm (the triple combination) was stopped early in 2011 due to increased mortality and hospitalizations — the combination was actively harmful. This effectively retired prednisone + azathioprine from IPF care. The remaining two arms continued for 60 weeks, and the published results in 2014 showed no benefit of NAC monotherapy on lung function decline or any clinical endpoint compared to placebo.
The current IPF treatment guideline (ATS/ERS/JRS/ALAT) lists NAC monotherapy as a conditional against recommendation — it should not be routinely used. The two FDA-approved IPF drugs are pirfenidone and nintedanib, both anti-fibrotic agents that slow lung-function decline by 50% or so. Some clinicians still use NAC as adjunct to pirfenidone or nintedanib for patients with rapidly progressive disease or significant oxidative-stress signature, but evidence is weak and the practice is not protocol-recommended.
There is one important caveat in the NAC-IPF story. A small subgroup analysis of PANTHER suggested that NAC monotherapy might benefit patients with a specific TOLLIP rs5743890 genotype, a polymorphism affecting Toll-like receptor signaling. This has not been independently confirmed and is not in routine clinical use, but it is an area of active research and represents the kind of pharmacogenomic stratification that may yet rescue NAC in a defined IPF subpopulation.
Acetaminophen Overdose — Rumack-Matthew Protocol
Acetaminophen (paracetamol) is one of the most widely used over-the-counter analgesics. At therapeutic doses, it is metabolized in the liver primarily by sulfation and glucuronidation, with a small fraction (about 5-10%) shunted through the cytochrome P450 (mainly CYP2E1) pathway that produces a highly reactive intermediate called N-acetyl-p-benzoquinone imine (NAPQI). Hepatic glutathione rapidly conjugates NAPQI to a harmless mercapturic acid that is excreted in urine.
At an overdose — classically defined as over 7.5 g in adults or 150 mg/kg in a single ingestion, though significant toxicity can occur at lower doses with chronic dosing, malnutrition, or alcoholism — the sulfation and glucuronidation pathways saturate, more drug is shunted through CYP2E1, NAPQI production overwhelms the available hepatic glutathione, and the unconjugated NAPQI binds covalently to hepatocyte proteins, killing cells in zone 3 (centrilobular) of the liver lobule. Without treatment, this produces fulminant hepatic failure within 3-5 days, with mortality of 30-50% in untreated severe cases.
The antidote is NAC. The mechanism is direct cysteine repletion to the depleted hepatic glutathione synthesis pathway, plus some direct NAPQI scavenging by NAC's free thiol. The Rumack-Matthew nomogram, published in 1975, is the clinical decision tool: a plasma acetaminophen level drawn 4 hours after a known acute ingestion is plotted against the nomogram line, and any patient above the treatment line receives a full course of NAC.
The standard treatment protocols are:
- IV NAC (Prescott protocol, used in most countries) — loading dose 150 mg/kg over 60 minutes, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours (total 300 mg/kg over 21 hours). Modern hospital protocols increasingly use a 20-hour total infusion. This is the standard for any presentation within the first 24 hours of ingestion.
- Oral NAC (Smilkstein protocol, traditional US protocol) — loading dose 140 mg/kg, then 70 mg/kg every 4 hours for 17 doses (total 1330 mg/kg over 72 hours). The taste is appalling, vomiting is common, and the oral protocol has been largely displaced by IV.
Outcomes with timely NAC are excellent — mortality drops to under 5% if treatment is started within 8 hours of overdose, and is still substantially improved up to 24 hours post-ingestion. NAC is also given (with less robust evidence but no harm) to patients presenting beyond 24 hours and to patients with chronic acetaminophen exposure complicated by liver injury.
The clinical point for general patients: oral NAC supplementation does not pre-protect against an acetaminophen overdose at the dose levels used for supplementation (600-1800 mg/day). The antidotal effect requires the very high IV doses of the Rumack-Matthew protocol. Casual NAC use is not a license to exceed the 3 g/day acetaminophen ceiling.
Bronchiectasis and Chronic Bronchitis
Bronchiectasis is permanent dilation of the bronchi, typically caused by repeated airway infection and resulting in chronic productive cough, recurrent bacterial colonization, and progressive lung function decline. The pathophysiology overlaps significantly with COPD and CF — thick, immobile mucus, neutrophilic airway inflammation, and chronic bacterial infection (often Pseudomonas aeruginosa or Haemophilus influenzae) cooperate to perpetuate the disease.
The Qi 2017 meta-analysis pooled 6 trials of high-dose NAC (1200-1800 mg/day) in non-CF bronchiectasis and found a significant reduction in exacerbation frequency and in 24-hour sputum volume, with improved quality of life on the St. George Respiratory Questionnaire. The BRONCH trial (2018) separately showed that 600 mg twice daily NAC over 1 year reduced exacerbations and improved quality of life in a Chinese bronchiectasis cohort. Mechanism is the same dual mucolytic + glutathione-restoring effect operating in COPD.
Chronic bronchitis without bronchiectasis (the productive-cough phenotype of COPD) also shows NAC benefit. The Decramer 2005 BRONCUS analysis suggested that NAC's benefit on exacerbation rate was most pronounced in the chronic-bronchitis subgroup. The Sutherland Cochrane review of NAC in chronic bronchitis specifically (2006) concluded that 400-600 mg/day reduces exacerbations and days of disability.
For practical use: in a non-CF bronchiectasis patient with chronic mucus production and frequent exacerbations, NAC 600 mg twice or three times daily is a reasonable adjunct to airway clearance techniques and standard antibiotics. The drug is well-tolerated, inexpensive, and can be combined with macrolide prophylaxis (azithromycin three days a week) and hypertonic saline nebulization for additive benefit.
Cystic Fibrosis
Cystic fibrosis is a genetic disorder caused by mutations in the CFTR chloride channel, producing thick, dehydrated airway mucus and progressive bronchiectatic lung disease. NAC has two distinct roles in CF care.
The traditional role is inhaled NAC as a mucolytic. Inhaled NAC has been used in CF since the 1960s and is still used in some centers, particularly for patients with thick, sticky secretions that respond poorly to dornase alfa alone. The CFTR-driven mucin abnormality in CF is one of the cleanest examples of disulfide-bond cross-linking pathology in airway disease.
The newer role is oral high-dose NAC for systemic antioxidant restoration. CF patients have significantly lower whole-body glutathione due to chronic neutrophilic airway inflammation, repeated antibiotic courses, and CFTR's underappreciated role as a glutathione transporter (CFTR moves glutathione from the cytosol to the airway lumen, and loss of CFTR function reduces airway-surface glutathione). Trials of oral NAC 600-1800 mg/day in CF have shown improved lung function and reduced sputum inflammation, though no current CF guideline mandates routine oral NAC.
With the advent of CFTR modulators (ivacaftor, lumacaftor-ivacaftor, elexacaftor-tezacaftor-ivacaftor) that partially restore CFTR function, the clinical landscape of CF has changed dramatically. Modern modulator-treated CF patients have much milder lung disease than their pre-modulator predecessors. The role of NAC in modulator-era CF is being reassessed; it remains useful as adjunct mucolytic therapy and may have residual antioxidant benefit, but it is no longer a centerpiece of CF care.
Asthma (and the Bronchospasm Caution)
NAC's role in asthma is more nuanced. Oral NAC is generally well tolerated in asthmatic patients and may have small antioxidant benefits, but the evidence for clinical benefit in asthma control is weak compared to COPD or bronchiectasis. The dominant treatments in asthma are inhaled corticosteroids and bronchodilators, and NAC is not a substitute.
The important caution is with nebulized (inhaled) NAC. Direct delivery of NAC to the airway can trigger paradoxical bronchospasm in some asthmatic patients, presumably through direct irritation of hyperreactive airway epithelium. The bronchospasm can be severe. Standard practice when nebulizing NAC in any patient with asthmatic phenotype is to co-administer a short-acting beta-agonist (albuterol) immediately before the NAC nebulization. Oral NAC does not carry this risk.
The other historical concern was that NAC, by reducing airway mucus, might worsen asthma by removing protective mucus that traps inhaled allergens. This concern has not been borne out in clinical trials of oral NAC.
Contrast-Induced Nephropathy
For two decades, oral and IV NAC was widely used as prophylaxis against contrast-induced acute kidney injury in patients undergoing CT scans and coronary angiography with iodinated contrast. The Tepel 2000 trial and several subsequent small trials suggested that NAC 600 mg twice daily on the day before and the day of contrast administration reduced the rise in serum creatinine after the procedure. The proposed mechanism was free-radical scavenging in the renal medulla, where contrast-induced osmotic stress generates ischemia and reactive oxygen species.
The PRESERVE trial (2018), an 8-center, 4993-patient definitive randomized comparison of NAC + bicarbonate vs placebo + saline, found no benefit of NAC for contrast nephropathy prevention. This effectively retired NAC from the contrast-nephropathy prophylaxis indication in most US institutions. Some interventional cardiology and IR practices still use the protocol because it is harmless and inexpensive, but it is no longer guideline-recommended. The active intervention that does work is volume expansion with isotonic saline before and after contrast administration.
Mentioning this here because it is a useful illustration of the broader truth about NAC research: small early trials sometimes show effects that do not replicate in larger trials, and the literature on NAC is full of both confirmed wins (acetaminophen overdose, COPD exacerbations) and confirmed failures (contrast nephropathy, IPF monotherapy). Clinicians and patients should weight large multi-center evidence over small early-phase trials.
Inhaled vs Oral NAC
Inhaled (nebulized) NAC delivers the active drug directly to the airway, achieving high local concentrations for mucolytic action with minimal systemic absorption. Typical regimen is 3-5 mL of 10% solution nebulized 2-4 times daily, often combined with albuterol to prevent bronchospasm. The smell is sulfur-like and unpleasant for patients and their families.
Oral NAC achieves much lower local airway concentrations but provides systemic glutathione restoration that the inhaled route does not. For chronic management of COPD, bronchiectasis, and chronic bronchitis, oral NAC is the standard approach. Inhaled NAC is reserved for acute mucus plugging, cystic fibrosis, and specific surgical contexts (e.g., post-thoracotomy retained secretions).
Some integrative-medicine clinics offer nebulized glutathione (rather than nebulized NAC) for various pulmonary indications including asthma, COPD, and chronic sinusitis. Evidence is weaker than for NAC, but the underlying logic (direct epithelial glutathione delivery) is similar. Glutathione is more expensive per dose than NAC and is generally not covered by insurance.
Practical Dosing for Lung Conditions
- COPD exacerbation prevention — 600 mg twice daily (1200 mg/day total), based on PANTHEON.
- Chronic bronchitis — 600 mg once or twice daily.
- Bronchiectasis — 600 mg twice or three times daily (1200-1800 mg/day).
- Cystic fibrosis (adjunct) — 600-1800 mg/day oral plus nebulized 10% NAC as needed.
- IPF — not routinely recommended after PANTHER; some clinicians still use 600 mg three times daily as adjunct.
- Acetaminophen overdose — IV under emergency protocol (150 mg/kg loading; not self-treatable).
- General respiratory antioxidant support — 600 mg once daily.
Oral NAC is best taken on an empty stomach, ideally with vitamin C (which helps maintain cysteine in its reduced active form) and a B-complex for transsulfuration pathway support. Side effects are typically limited to mild GI discomfort, sulfur-tinged taste/burp, and rare rash. Patients on nitroglycerin or anticoagulants should clear NAC use with their prescriber.
Key Research Papers
- Decramer M et al. (2005). Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost-Utility Study, BRONCUS): a randomised placebo-controlled trial. The Lancet. — PubMed
- Zheng JP et al. (2014). Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respiratory Medicine. — PubMed
- Tse HN et al. (2013). High-dose N-acetylcysteine in stable COPD: the 1-year, double-blind, randomized, placebo-controlled HIACE study. Chest. — PubMed
- Demedts M et al. (2005). High-dose acetylcysteine in idiopathic pulmonary fibrosis (IFIGENIA). NEJM. — PubMed
- Idiopathic Pulmonary Fibrosis Clinical Research Network (2014). Randomized trial of acetylcysteine in idiopathic pulmonary fibrosis (PANTHER-IPF). NEJM. — PubMed
- Rumack BH, Matthew H (1975). Acetaminophen poisoning and toxicity. Pediatrics. — PubMed
- Prescott LF et al. (1979). Intravenous N-acetylcystine: the treatment of choice for paracetamol poisoning. BMJ. — PubMed
- Smilkstein MJ et al. (1988). Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. NEJM. — PubMed
- Qi Q et al. (2017). N-acetylcysteine treatment for non-cystic-fibrosis bronchiectasis: a meta-analysis. Respirology. — PubMed
- Sutherland ER et al. (2006). N-acetylcysteine for chronic bronchitis: a Cochrane systematic review. Cochrane Database. — PubMed
- Weinreb O, Mandel S, Bar-Am O et al. (2006). Multifunctional neuroprotective derivatives of rasagiline as anti-Alzheimer drug candidates. Frontiers in Bioscience. (NAC mechanism context) — PubMed
- PRESERVE Investigators (2018). Outcomes after angiography with sodium bicarbonate and acetylcysteine. NEJM. — PubMed
- Tepel M et al. (2000). Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. NEJM. — PubMed
- Cazzola M, Calzetta L, Page C, Jardim J et al. (2015). Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: a meta-analysis. European Respiratory Review. — PubMed
PubMed Topic Searches
- PubMed: NAC and COPD exacerbations
- PubMed: NAC in IPF
- PubMed: NAC for acetaminophen overdose
- PubMed: NAC for bronchiectasis
- PubMed: NAC in cystic fibrosis
Connections
- NAC and Kidney Health — the renal half of the NAC evidence base — contrast-induced nephropathy from Tepel 2000 through the PRESERVE and ACT trials, chronic kidney disease, hemodialysis, and cystine stone prevention.
- NAC and Glutathione Precursors — NAC as a glutathione-raising supplement rather than an organ therapy — the hepatocyte synthesis pathway, the psychiatric and PCOS trials, dosing, and the glycine and selenium cofactors.
- Cysteine Overview
- Cysteine Benefits Hub
- Cysteine for Glutathione Synthesis
- Cysteine for Hair and Nails
- Cysteine for Detoxification
- NAC (N-Acetylcysteine)
- NAC and Respiratory Health
- NAC and Glutathione
- COPD
- Pulmonary Fibrosis
- ARDS
- Pneumonia
- Bronchitis
- All Pulmonology
- Acetaminophen Toxicity
- Acetaminophen (Tylenol) Toxin Profile
- Glycine
- Vitamin C