Cysteine for Glutathione Synthesis
Glutathione (gamma-glutamyl-cysteinyl-glycine, or GSH) is the most abundant intracellular antioxidant in the human body, present at millimolar concentration inside virtually every cell. Cysteine is its rate-limiting precursor — not because cysteine is the only amino acid required, but because cysteine is the only one of the three (glutamate, cysteine, glycine) that the diet routinely fails to provide in sufficient quantity, and because the first enzyme in the synthetic pathway (glutamate-cysteine ligase, GCL) is feedback-inhibited by glutathione itself in a way that ties total cellular glutathione capacity directly to cysteine availability. Whole-body glutathione concentrations decline approximately 20-40% between young adulthood and old age — a deficit that the Sekhar GlyNAC trials at Baylor have shown can be reversed by oral supplementation of glycine + N-acetylcysteine, with measurable improvements in mitochondrial function, insulin resistance, oxidative stress markers, and clinical frailty scores in adults aged 70-80.
Table of Contents
- What Glutathione Is and Why It Matters
- The Two-Enzyme Synthesis Pathway (GCL, GSS)
- Why Cysteine Is the Rate-Limiting Amino Acid
- The Aging Decline in Glutathione
- The Sekhar GlyNAC Trials at Baylor
- NAC vs Free Cysteine vs Oral Glutathione
- Liposomal and Acetylated Glutathione Forms
- Whey Protein as a Cysteine Source
- Measuring Glutathione Status
- Clinical Applications by Condition
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
What Glutathione Is and Why It Matters
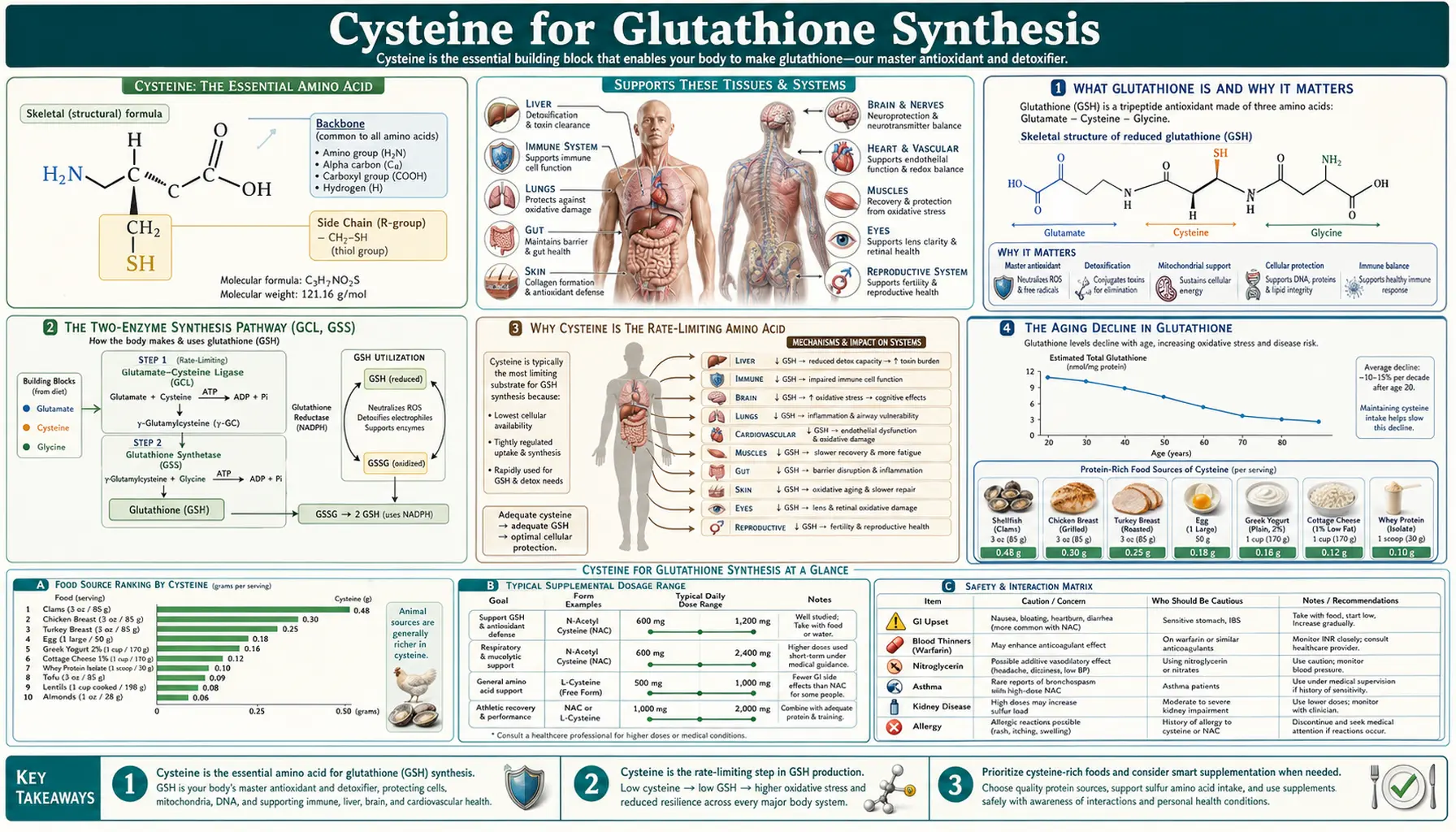
Glutathione is a tripeptide assembled from three amino acids in this specific order: glutamate, cysteine, and glycine. The peculiarity is that the bond between glutamate and cysteine is a gamma-peptide bond — formed between the side-chain carboxyl group of glutamate rather than its alpha-carboxyl — which is why glutathione cannot be assembled by the ribosome like an ordinary protein. It must be synthesized one amino acid at a time by two dedicated enzymes in the cytosol of every cell.
The functional center of the glutathione molecule is the thiol (–SH) group on the cysteine residue. This thiol can give up an electron (or a hydrogen atom) to a reactive oxygen species, neutralizing the radical. Two oxidized glutathione molecules then pair via a disulfide bond to form GSSG (oxidized glutathione disulfide), which is subsequently reduced back to two GSH molecules by the NADPH-dependent enzyme glutathione reductase. The ratio of reduced glutathione (GSH) to oxidized glutathione (GSSG) inside a cell is one of the most fundamental indicators of cellular redox status — healthy resting cells maintain ratios above 100:1, while a drop toward 10:1 indicates significant oxidative stress.
Beyond direct radical scavenging, glutathione has at least four other essential functions. It is the cofactor for the entire glutathione-S-transferase (GST) family of Phase II detoxification enzymes, which conjugate glutathione to lipophilic toxins to render them water-soluble for excretion. It regenerates oxidized Vitamin C (ascorbate) and Vitamin E (tocopherol) back to their reduced antioxidant forms, multiplying the protective capacity of those vitamins. It maintains the reduced state of critical protein thiols (including the active-site cysteines on hundreds of enzymes), keeping them functional. And it is the substrate for the glutathione peroxidase family of enzymes that detoxify hydrogen peroxide and lipid peroxides, including the recently celebrated GPX4 that prevents the iron-dependent cell death pathway called ferroptosis.
The Two-Enzyme Synthesis Pathway (GCL, GSS)
Glutathione is built by exactly two enzymes acting sequentially in the cytosol. The first — and rate-limiting — enzyme is glutamate-cysteine ligase (GCL, also historically called gamma-glutamylcysteine synthetase, gamma-GCS). GCL is a heterodimer with a catalytic subunit (GCLC) and a modifier subunit (GCLM). It joins glutamate and cysteine via the unusual gamma-peptide bond to produce gamma-glutamylcysteine, consuming one ATP in the process.
GCL is feedback-inhibited by its own end product, glutathione, which binds at an allosteric site on GCLC and reduces enzyme activity when intracellular GSH is already high. This feedback loop is what makes glutathione synthesis self-limiting and keeps cellular concentrations within a healthy range (typically 1-10 mM depending on tissue). The dissociation constant for GSH feedback inhibition is approximately 2.3 mM — very close to typical resting cytosolic GSH concentration, meaning the enzyme is partially throttled essentially all the time.
The second enzyme, glutathione synthetase (GSS), adds glycine to the C-terminus of gamma-glutamylcysteine to complete the tripeptide, again consuming one ATP. GSS is generally not rate-limiting because its activity in most tissues is several-fold higher than GCL activity, and because glycine intracellular concentration is generally adequate (though notably less so in elderly adults, the empirical basis for the Sekhar GlyNAC formulation discussed below).
Loss-of-function mutations in either enzyme cause rare inherited disorders. GCL deficiency produces hemolytic anemia and chronic neurologic symptoms due to chronically low glutathione, particularly in red blood cells which rely on glutathione to protect hemoglobin from oxidation. GSS deficiency produces a more severe phenotype called 5-oxoprolinuria, where the unused gamma-glutamylcysteine substrate is shunted into a pathway that overproduces 5-oxoproline (pyroglutamate), causing severe metabolic acidosis in addition to the same hemolysis.
Why Cysteine Is the Rate-Limiting Amino Acid
The phrase "rate-limiting" gets used loosely, but for glutathione synthesis it has a precise meaning: cellular glutathione concentration responds quantitatively to intracellular cysteine availability, and supplementing the other two precursors (glutamate, glycine) in isolation does not raise glutathione much, while supplementing cysteine alone does. Several biochemical facts converge to make this true.
- Cysteine is the least abundant of the three precursors in plasma and cytosol. Typical fasting plasma cysteine is around 50-200 µM (mostly as the oxidized disulfide cystine), while glutamate is 50-80 µM (intracellularly far higher, often 1-10 mM) and glycine is 200-300 µM. Glutamate and glycine are also synthesizable de novo from carbohydrate intermediates in essentially unlimited quantity. Cysteine is not — it requires either dietary intake or the methionine-fed transsulfuration pathway, both of which are constrained.
- The GCL Km for cysteine is at or above typical intracellular concentration. The half-saturating concentration of GCL for cysteine is approximately 100-300 µM depending on tissue, which means the enzyme is rarely operating at maximal velocity — raising cysteine concentration raises enzyme activity proportionally.
- Cysteine is metabolically expensive and toxic to accumulate. Free cysteine is auto-oxidizing and can generate hydrogen peroxide. Cells therefore actively maintain low intracellular free cysteine, storing most of their reduced sulfur as glutathione itself. The pool of available cysteine for new GSH synthesis is consequently very small and very responsive to intake.
- Methionine-to-cysteine conversion through the transsulfuration pathway is slow. Even with adequate methionine intake, the conversion of homocysteine to cysteine via cystathionine-beta-synthase (CBS) and cystathionine-gamma-lyase (CSE) is a slow steady-state pathway that cannot quickly respond to acute increases in glutathione demand. Direct cysteine intake (typically as NAC, which is rapidly deacetylated to cysteine inside cells) is required for rapid response.
The practical implication is that for any clinical intervention aimed at raising glutathione — in aging, in chronic disease, in acute toxic exposure — the dominant strategy is to increase cysteine availability. NAC is the standard pharmaceutical vehicle for this. The other approach is undenatured whey protein, which contains glutamyl-cysteine peptides that deliver cysteine across the gut wall in a more bioavailable form than free amino acid; see the whey protein section below.
The Aging Decline in Glutathione
Cellular glutathione concentration declines progressively with age across virtually all tissues studied. Erythrocyte (red blood cell) GSH falls approximately 20-25% between age 20 and age 80. Hepatic GSH falls roughly 30% over the same span. Brain tissue, lung, and skeletal muscle all show measurable decline. The drop is greater in individuals with chronic inflammatory or metabolic disease, particularly diabetes, NAFLD, COPD, and HIV.
The mechanism of this decline is multifactorial. GCL enzyme expression decreases with age, partially due to declining Nrf2 transcription factor activity (Nrf2 is the master regulator of antioxidant gene expression including GCLC and GCLM). Cysteine availability also drops in older adults — partly from reduced dietary protein intake, partly from slower transsulfuration. Glycine availability drops too, driven by reduced de novo glycine synthesis from serine and reduced dietary intake. And the chronic low-grade oxidative stress of aging continually consumes glutathione faster than the elderly body can replace it.
The clinical consequence of this decline is real. Lower glutathione status correlates with greater frailty, slower wound healing, reduced muscle protein synthesis, increased insulin resistance, increased risk of neurodegenerative disease, and reduced mitochondrial function. Some of this is correlation (oxidative stress and reduced glutathione both flow from the same upstream causes), but the Sekhar GlyNAC intervention trials discussed in the next section provide strong evidence that the deficit is also causal — reversing the glutathione drop with oral precursors produces measurable functional improvements.
The Sekhar GlyNAC Trials at Baylor
Rajagopal V. Sekhar at Baylor College of Medicine has run a series of clinical trials over the past 15 years showing that oral glycine + N-acetylcysteine (the combination he calls "GlyNAC") restores glutathione status and reverses multiple markers of biological aging in older adults. The pivotal recent trial (published 2022 in Clinical and Translational Medicine) randomized 24 older adults (mean age 75) and 12 younger controls (mean age 25) to receive 1.6 mmol/kg/day of glycine plus 0.81 mmol/kg/day of NAC for 16 weeks, then 16 more weeks off treatment to assess durability.
The findings were unusually clean for an aging-intervention trial. Compared to baseline and compared to matched controls, the GlyNAC-supplemented older adults showed:
- Restoration of erythrocyte GSH to young-adult levels within 4 weeks, sustained throughout the treatment period
- Reduction in oxidative stress markers (F2-isoprostanes, 8-OHdG, malondialdehyde) to levels comparable to young controls
- Improved mitochondrial fatty acid oxidation measured by isotope-tracer techniques
- Improved insulin sensitivity on hyperinsulinemic-euglycemic clamp
- Reduced systemic inflammation (IL-6, TNF-alpha, CRP)
- Improved cognitive function on standard test batteries
- Improved muscle strength (handgrip, knee extension)
- Improved gait speed and walking endurance
- Reduction in clinical frailty scores
After the washout period, almost all of these benefits regressed back toward baseline — suggesting that the intervention works through ongoing glutathione restoration rather than producing some durable structural change.
The implications are substantial but should not be overstated. This was a small trial, single-center, without a placebo-controlled GlyNAC arm in older adults — the comparison was within-subject before-and-after, with younger controls used to define the target. A larger, multicenter, placebo-controlled trial is now underway. The trial also did not test cysteine-alone vs glycine-alone vs combination, so the relative contribution of each precursor is not perfectly clean (though prior single-agent trials suggest both contribute, with the combination being substantially more effective than either alone in the elderly).
The practical translation, pending larger trials: for adults over approximately 65 interested in aging-mitigation supplementation, the GlyNAC combination at the Sekhar doses (approximately 100 mg/kg/day of glycine and 50 mg/kg/day of NAC, or roughly 7 g glycine + 3.5 g NAC for a 70-kg adult, divided across the day) is currently the most clinically-supported intervention for restoring glutathione status. Lower maintenance doses (1-2 g glycine + 600-1200 mg NAC daily) are reasonable for general antioxidant support.
NAC vs Free Cysteine vs Oral Glutathione
Three supplemental strategies exist for raising intracellular glutathione: N-acetylcysteine (NAC), free L-cysteine, and oral glutathione itself. They are not interchangeable.
N-acetylcysteine (NAC) is the dominant clinical and supplemental form for several reasons. The acetyl group on the amino nitrogen protects the molecule from auto-oxidation during shelf storage and during the trip through the upper gastrointestinal tract, dramatically improving stability and oral bioavailability compared to free cysteine. Once inside cells (especially hepatocytes and enterocytes), endogenous acylases cleave the acetyl group to release free cysteine, which feeds directly into glutathione synthesis. NAC has 60+ years of clinical use behind it (initially as a mucolytic), an excellent safety profile, and well-characterized pharmacokinetics. Typical doses are 600-1800 mg/day divided. See the dedicated NAC page and the NAC and Lung Health deep-dive for more.
Free L-cysteine is available as a supplement but is significantly less stable than NAC and is more likely to cause gastrointestinal irritation and, paradoxically, to generate some hydrogen peroxide from auto-oxidation in the gut. It also tastes terrible. The one situation where free cysteine has been used clinically is in pediatric parenteral nutrition formulations — premature infants have very immature transsulfuration capacity and benefit from direct cysteine supply in their IV nutrition. For oral use, NAC is almost always preferred over free cysteine.
Oral glutathione is widely sold but has historically been considered poorly bioavailable because glutathione is rapidly hydrolyzed by intestinal gamma-glutamyltransferase (GGT) into its component amino acids before crossing the gut wall — meaning oral GSH effectively delivers cysteine, glutamate, and glycine to the body in roughly the same proportion as eating the equivalent free amino acids. Some recent trials suggest that very high doses of standard oral glutathione (1 g/day for 6 months) can modestly raise erythrocyte GSH, but the cost-effectiveness compared to NAC is poor. Liposomal and acetylated glutathione formulations (discussed below) attempt to address the bioavailability problem more effectively.
Liposomal and Acetylated Glutathione Forms
Two newer oral glutathione formulations attempt to deliver intact glutathione past the digestive enzymes that destroy ordinary GSH supplements.
Liposomal glutathione packages GSH inside phosphatidylcholine liposomes that survive the stomach and small intestine, releasing their cargo for absorption in the lower small intestine or distal gut. A 2018 trial by Sinha et al. showed that 6 weeks of 500 mg/day liposomal GSH raised whole blood GSH by 25-50% in adults, with improvements in NK cell function and lymphocyte parameters. The product is several times more expensive per gram of GSH delivered than NAC, but the convenience of getting glutathione in its final form is appealing to some patients.
S-acetyl glutathione (acetyl-glutathione) places an acetyl group on the cysteine sulfur, blocking the cysteine thiol from oxidation during digestion. Once inside cells the acetyl group is cleaved by intracellular thioesterases, releasing functional glutathione. Pharmacokinetic studies show meaningful oral bioavailability and intracellular GSH rises with doses of 100-300 mg/day. Cost is intermediate between standard oral GSH and liposomal GSH.
For most patients, NAC remains the most cost-effective glutathione-raising strategy. Liposomal or S-acetyl glutathione may be worth considering in patients with poor NAC tolerance, with significant gut malabsorption, or with conditions where direct delivery of finished glutathione (rather than precursors) appears clinically advantageous.
Whey Protein as a Cysteine Source
Undenatured whey protein concentrate (specifically, products processed at low temperature to preserve the native structure of beta-lactoglobulin and the cysteine-rich glycopeptides) has been shown in multiple controlled trials to raise intracellular glutathione in immune and hepatic cells more effectively than equivalent amounts of free amino acids. The proposed mechanism is that whey delivers cysteine in the form of small glutamyl-cysteine dipeptides and serum-albumin-like peptides that are absorbed intact across the gut wall and cleaved to release cysteine directly inside cells, bypassing the auto-oxidation problem of free cysteine in plasma.
The Bounous undenatured whey protein concentrate trials in HIV patients in the 1990s established the principle. More recent trials in elderly populations, athletes, and chemotherapy patients have replicated the glutathione-raising effect. Typical dose is 20-40 g/day of undenatured whey protein concentrate, taken on an empty stomach or 30+ minutes before exercise.
Whey-derived alpha-lactalbumin and serum albumin fractions are the most cysteine-dense components and are sometimes sold as concentrated "cysteine peptide" products. The simpler approach for most users is a high-quality undenatured whey concentrate (not isolate or hydrolysate, both of which damage the cysteine peptides). Heat-treated whey (the common low-cost variety used in mass-market protein powders) does not provide the same glutathione benefit.
Measuring Glutathione Status
Glutathione status can be assessed in three principal ways, each with limitations.
- Erythrocyte GSH — the most commonly used clinical test, measures glutathione concentration in red blood cells. Easy to obtain (heparinized blood draw) and reasonably reflective of whole-body glutathione status because red cells have no nucleus and depend entirely on glutathione for protection. Normal range is approximately 1100-1900 µmol/L of packed red cells; levels below 1000 suggest depletion. Available through several specialty labs (Genova, Doctor's Data, SpectraCell).
- Whole-blood total glutathione (GSH + GSSG) and reduced-to-oxidized ratio — more informative than erythrocyte GSH alone because it captures both the absolute pool and the redox state. A low GSH:GSSG ratio (under 50:1) indicates significant ongoing oxidative stress even if total GSH is in the normal range. Less widely available, more expensive, and requires careful sample handling to prevent ex vivo oxidation.
- Plasma cysteine and cystine — not a direct glutathione measure, but plasma cysteine availability is so tightly coupled to intracellular GSH synthesis capacity that it is a useful proxy. Total plasma cysteine (free + cystine + protein-bound) below 200 µM suggests cysteine-limited glutathione synthesis.
Routine glutathione monitoring is not necessary for most patients on supportive NAC or GlyNAC supplementation — the doses involved are well within the safety margin, and clinical response is usually obvious. Measurement becomes more useful in research settings, in patients with poor response to supplementation (raising the question of underlying transsulfuration defects), and in patients on long-term high-dose protocols where occasional checking confirms that the intervention is producing the intended biological effect.
Clinical Applications by Condition
Clinical use of cysteine and glutathione precursors centers on conditions where glutathione depletion plays a documented role in disease pathophysiology or where antioxidant restoration produces measurable clinical benefit. Major applications include:
- Aging and frailty — the Sekhar GlyNAC protocol discussed above, supported by mechanistic and small-trial evidence. Reasonable to consider in any adult over approximately 65 with frailty, sarcopenia, or chronic inflammatory load.
- Acetaminophen toxicity — the canonical clinical use, where IV NAC restores hepatic glutathione before NAPQI destroys hepatocytes. Covered in detail on the NAC and Lung Health page.
- Non-alcoholic fatty liver disease (NAFLD) — NAFLD is characterized by hepatic glutathione depletion and oxidative liver injury. Trials of NAC 1200-1800 mg/day show improvement in liver enzymes and steatosis on imaging.
- COPD and chronic bronchitis — NAC reduces exacerbation frequency through both mucolytic action and lung-glutathione restoration. See the NAC and Lung Health page.
- Polycystic ovary syndrome (PCOS) — NAC improves insulin sensitivity and ovulation, with effect sizes comparable to metformin in some head-to-head trials. The NAC Fertility and PCOS page has details.
- Psychiatric conditions — NAC at 1200-2400 mg/day has positive trial data in OCD, trichotillomania, bipolar depression, and adjunctive treatment of schizophrenia, working partly through modulation of brain glutamate via the cystine-glutamate antiporter and partly through cortical glutathione restoration.
- HIV — HIV is associated with profound glutathione depletion that correlates with disease progression. NAC and whey protein supplementation slow CD4 decline and improve immune parameters.
- Cystic fibrosis — both inhaled and oral NAC are used to thin airway mucus and restore lung-epithelial glutathione.
Cautions and Drug Interactions
- Nitroglycerin and other organic nitrates — NAC potentiates the vasodilator effect, theoretically risking hypotension. Cardiac patients on nitrates should clear NAC use with their prescriber.
- Asthma — nebulized NAC can trigger bronchospasm in some asthmatic patients and should be co-administered with a bronchodilator. Oral NAC is generally well tolerated in asthma.
- Active peptic ulcer disease — NAC can mildly increase gastric acid output and irritate gastric mucosa; use with caution.
- Cystinuria — the inherited disorder of cystine transport. Supplemental cysteine is contraindicated as it worsens kidney stone risk.
- Anticoagulants — NAC has mild antiplatelet effects and may potentiate warfarin or DOACs at high doses; monitor INR if combining.
- Acetaminophen toxicity — ironically, casual NAC use does not protect against an acute acetaminophen overdose if the overdose occurs while taking oral NAC, because the antidotal effect requires the high IV doses and timed administration of the Rumack-Matthew protocol. NAC supplementation is not a license to exceed acetaminophen dose limits.
- Excessive doses — sustained oral NAC above 3 g/day can produce nausea, diarrhea, headache, and rarely rashes. Stay within the 600-1800 mg/day therapeutic window for chronic use, with higher doses (2400 mg/day) reserved for specific indications under clinical supervision.
- Pregnancy — oral NAC has been used safely in pregnancy (including in PCOS protocols extending into early pregnancy) but high-dose regimens should be supervised.
Key Research Papers
- Kumar P, Liu C, Hsu JW, Chacko S, Minard C, Jahoor F, Sekhar RV (2021). Glycine and N-acetylcysteine (GlyNAC) supplementation in older adults improves glutathione deficiency, oxidative stress, mitochondrial dysfunction, inflammation, insulin resistance, endothelial dysfunction, genotoxicity, muscle strength, and cognition. Clinical and Translational Medicine. — PubMed
- Sekhar RV et al. (2011). Glutathione synthesis is diminished in patients with uncontrolled diabetes and restored by dietary supplementation with cysteine and glycine. Diabetes Care. — PubMed
- Sekhar RV et al. (2011). Deficient synthesis of glutathione underlies oxidative stress in aging and can be corrected by dietary cysteine and glycine supplementation. American Journal of Clinical Nutrition. — PubMed
- Atkuri KR, Mantovani JJ, Herzenberg LA, Herzenberg LA (2007). N-Acetylcysteine — a safe antidote for cysteine/glutathione deficiency. Current Opinion in Pharmacology. — PubMed
- Wu G, Fang YZ, Yang S, Lupton JR, Turner ND (2004). Glutathione metabolism and its implications for health. Journal of Nutrition. — PubMed
- Lu SC (2013). Glutathione synthesis. Biochimica et Biophysica Acta. — PubMed
- Richie JP Jr et al. (2015). Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. European Journal of Nutrition. — PubMed
- Sinha R et al. (2018). Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. European Journal of Clinical Nutrition. — PubMed
- Bounous G (2000). Whey protein concentrate (WPC) and glutathione modulation in cancer treatment. Anticancer Research. — PubMed
- Lyons J, Rauh-Pfeiffer A, Yu YM et al. (2000). Blood glutathione synthesis rates in healthy adults receiving a sulfur amino acid-free diet. Proceedings of the National Academy of Sciences. — PubMed
- Townsend DM, Tew KD, Tapiero H (2003). The importance of glutathione in human disease. Biomedicine and Pharmacotherapy. — PubMed
- Forman HJ, Zhang H, Rinna A (2009). Glutathione: overview of its protective roles, measurement, and biosynthesis. Molecular Aspects of Medicine. — PubMed
- Sastre J, Pallardo FV, Vina J (2003). The role of mitochondrial oxidative stress in aging. Free Radical Biology and Medicine. — PubMed
- Kerksick C, Willoughby D (2005). The antioxidant role of glutathione and N-acetyl-cysteine supplements and exercise-induced oxidative stress. Journal of the International Society of Sports Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Glutathione synthesis cysteine rate-limiting
- PubMed: GlyNAC older adults
- PubMed: NAC and intracellular glutathione
- PubMed: GCL enzyme regulation
- PubMed: Whey protein and glutathione
Connections
- Cysteine Overview
- Cysteine Benefits Hub
- NAC and Lung Health
- Cysteine for Hair and Nails
- Cysteine for Detoxification
- NAC (N-Acetylcysteine)
- NAC and Glutathione
- NAC for Fertility and PCOS
- Glycine (GlyNAC Partner)
- Methionine (Transsulfuration)
- Glutamic Acid (GSH Precursor)
- Taurine (Cysteine Downstream)
- Selenium (GPX Cofactor)
- Sulfur
- Oxidative Stress
- Fatty Liver (NAFLD)
- Homocysteine