N-acetyl-cysteine (NAC) and Glutathione Precursors
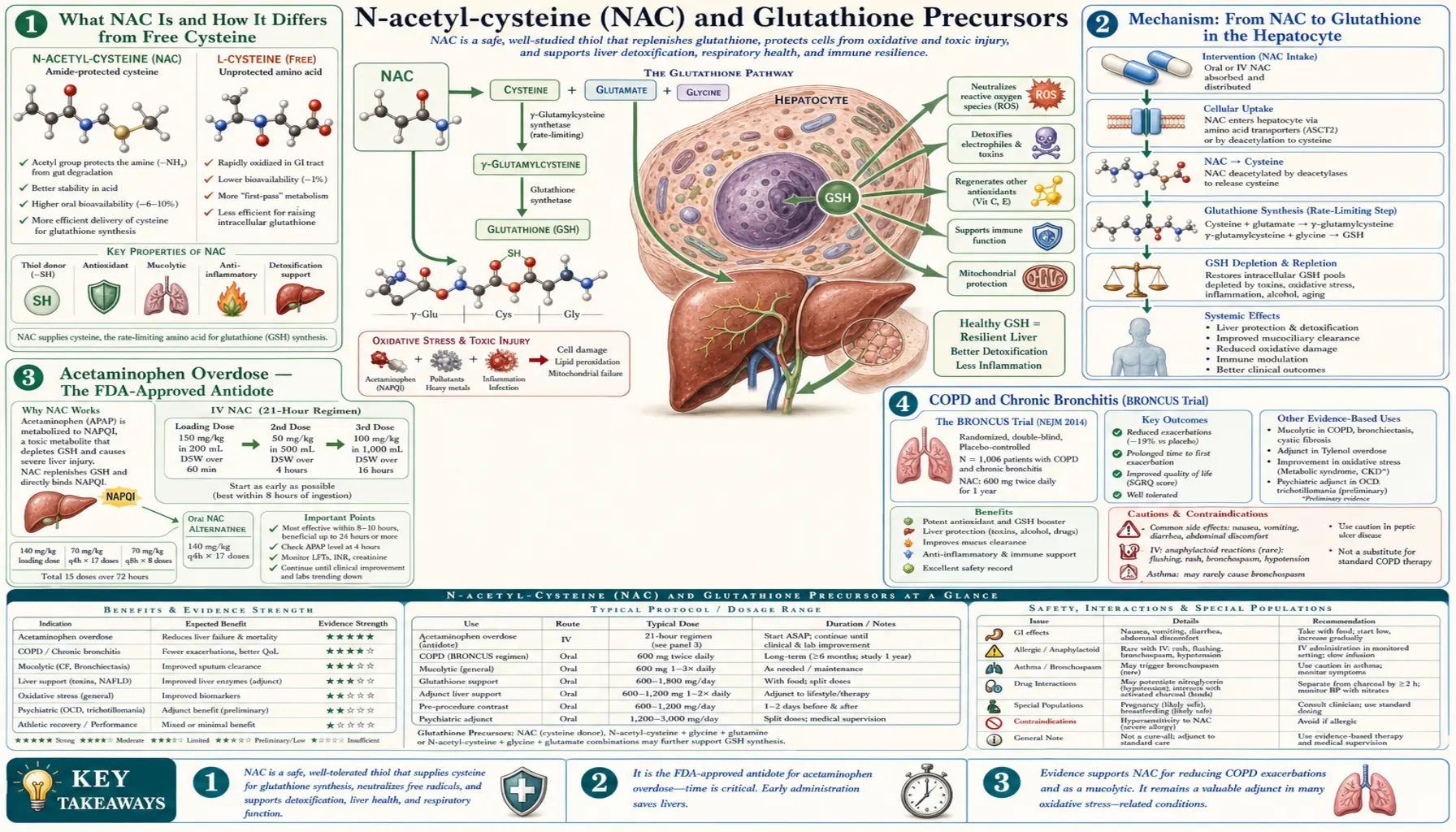
N-acetylcysteine (NAC) is the single most studied supplement for raising tissue glutathione. It supplies the rate-limiting cysteine precursor in an absorbable, oxidation-stable form. As Mucomyst it is an FDA-approved hospital drug for acetaminophen overdose, mucolytic therapy in cystic fibrosis, and contrast-induced nephropathy prophylaxis. As an over-the-counter supplement it has accumulated substantive clinical trial evidence for chronic bronchitis (BRONCUS), polycystic ovary syndrome, obsessive-compulsive disorder, trichotillomania, addiction, and bipolar depression. The FDA-versus-supplement-industry regulatory dispute over NAC's supplement status remains unresolved as of 2026. This deep-dive walks through the mechanism, the established and emerging clinical uses, the dose-response and side-effect profile, and the supporting nutrients (glycine, selenium, B-vitamins) that complete the glutathione synthesis pathway.
Table of Contents
- What NAC Is and How It Differs from Free Cysteine
- Mechanism: From NAC to Glutathione in the Hepatocyte
- Acetaminophen Overdose — The FDA-Approved Antidote
- COPD and Chronic Bronchitis (BRONCUS Trial)
- Contrast-Induced Nephropathy Prophylaxis
- Psychiatric Uses: OCD, Trichotillomania, Addiction, Bipolar
- PCOS, Fertility, and Metabolic Applications
- Dosing, Timing, and Quality
- Glycine, Selenium, and the Other Synthesis Cofactors
- Cautions, Drug Interactions, and the FDA Regulatory Dispute
- Key Research Papers
- Connections
- Featured Videos
What NAC Is and How It Differs from Free Cysteine
N-acetylcysteine is the amino acid cysteine with an acetyl group attached to the amino nitrogen. The chemical modification is simple but functionally critical — it stabilizes cysteine for oral delivery.
Free cysteine is unstable in plasma and oxygenated solutions. Two cysteine thiols readily form a disulfide bond producing the oxidized dimer cystine, which is poorly absorbed, can precipitate (causing the kidney-stone disease cystinuria), and at high concentration is potentially neurotoxic. Cysteine supplements are therefore poorly bioavailable and have an unfavorable safety profile.
NAC's acetyl group prevents this dimerization during digestion and absorption. After absorption, intestinal and hepatic acylases cleave the acetyl group, releasing free cysteine intracellularly where it can immediately enter the glutathione synthesis pathway. NAC is therefore not itself the active molecule — it is a delivery vehicle for cysteine that bypasses the absorption problems of free cysteine.
An additional consideration: NAC retains some intrinsic antioxidant activity itself through its free thiol group, scavenging hydroxyl radicals and hypochlorous acid directly. This is a minor contribution compared to the downstream glutathione-driven effects, but it explains modest acute effects of NAC in some experimental settings before glutathione synthesis ramps up.
Mechanism: From NAC to Glutathione in the Hepatocyte
The path from a swallowed NAC capsule to elevated tissue glutathione has several steps:
- Absorption — NAC is absorbed through the small intestine with bioavailability of approximately 6-10% for the parent compound. Most NAC is deacetylated in the intestinal mucosa and absorbed as cysteine, raising plasma cysteine within 1-2 hours of dosing.
- First-pass hepatic uptake — the liver extracts a substantial fraction of absorbed cysteine on first pass through portal circulation, where it enters the glutathione synthesis pathway as the rate-limiting substrate for gamma-glutamyl cysteine ligase.
- Hepatic glutathione synthesis — within hours of NAC dosing, hepatic glutathione content increases measurably. This is the basis for the acetaminophen overdose antidote effect, where hepatic glutathione must be restored before NAPQI accumulates to a damaging level.
- Systemic distribution — some cysteine and glutathione cycle out of the liver into systemic circulation as gamma-glutamyl cysteine or cystine, supplying peripheral tissues with substrates for local glutathione synthesis.
- Tissue-specific responses — tissues vary in their responsiveness to NAC. Liver responds robustly. Lungs show measurable effects (relevant to the COPD evidence). Brain crosses the blood-brain barrier modestly, supporting the psychiatric applications. Kidney concentrates cysteine for renal glutathione synthesis (relevant to contrast nephropathy prophylaxis).
The pharmacokinetic profile favors divided dosing — NAC plasma half-life is approximately 6 hours, so twice-daily dosing maintains more consistent cysteine supply than a single large daily dose. The standard regimens in clinical trials reflect this: 600 mg twice daily for chronic bronchitis, 600-1200 mg twice daily for psychiatric indications.
Acetaminophen Overdose — The FDA-Approved Antidote
Acetaminophen overdose is the leading cause of acute liver failure in the United States, with approximately 100,000 calls to poison control annually and 500-1,000 deaths despite available antidote. The biochemistry has been precisely mapped:
Therapeutic-dose acetaminophen is cleared 90% by glucuronidation and sulfation. Only 5-10% goes through CYP2E1, generating the reactive intermediate N-acetyl-p-benzoquinone-imine (NAPQI). NAPQI is immediately quenched by hepatic glutathione, forming a non-toxic conjugate excreted in urine. In overdose (typically >7.5 g acute or >4 g chronic in adults; less in children), the conjugation pathways saturate, more acetaminophen flows through CYP2E1, NAPQI production accelerates, and hepatic glutathione drops. When glutathione falls below approximately 30% of normal, free NAPQI begins arylating hepatocyte proteins, causing centrilobular hepatic necrosis. Without intervention, mortality from severe overdose approaches 25-30%.
NAC is the antidote because it supplies cysteine for accelerated glutathione resynthesis, restoring NAPQI quenching capacity. NAC is most effective if given within 8 hours of ingestion, with progressively reduced efficacy out to 24 hours. The Rumack-Matthew nomogram is used to determine which patients need treatment based on the serum acetaminophen level at 4 hours post-ingestion.
The standard treatment regimens:
- Oral protocol (72-hour Prescott) — 140 mg/kg loading dose, then 70 mg/kg every 4 hours for 17 doses (total 1,330 mg/kg over 72 hours). High dose; nausea and vomiting are common.
- Intravenous protocol (21-hour Smilkstein) — 150 mg/kg loading over 60 minutes, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours (total 300 mg/kg over 21 hours). Faster, but small risk of anaphylactoid reaction at the loading infusion.
NAC works. With timely administration mortality drops from 25-30% to under 5%. This is one of the cleanest cause-and-effect pharmacology stories in clinical toxicology — depleted glutathione causes the injury, restoring glutathione precursor reverses the cascade.
COPD and Chronic Bronchitis (BRONCUS Trial)
The lung evidence for NAC has accumulated over four decades. NAC has direct mucolytic properties (its free thiol breaks the disulfide bonds in viscous airway mucus) plus indirect glutathione-mediated antioxidant effects that may reduce the chronic oxidative damage that drives COPD progression.
The BRONCUS trial (Bronchitis Randomized On NAC Cost-Utility Study) — Decramer et al., Lancet 2005 — randomized 523 COPD patients to NAC 600 mg/day or placebo for 3 years. Results:
- No effect on the primary endpoint of FEV1 decline (the conventional COPD progression marker)
- Significant reduction in COPD exacerbations in the subgroup not using inhaled corticosteroids
- Reduced hyperinflation
- Improved quality-of-life scores
The subsequent PANTHEON trial (Zheng et al., Lancet Respiratory Medicine 2014) in 1,006 Chinese COPD patients used a higher dose — 600 mg twice daily — for 1 year and found a more definitive 22% reduction in exacerbations across the whole population. The HIACE trial in Hong Kong (Tse et al. 2014) confirmed similar benefits at the higher dose.
The current evidence supports NAC 600 mg twice daily (1,200 mg/day total) for symptomatic COPD or chronic bronchitis with frequent exacerbations. It is part of the ERS/ATS COPD guidelines as an adjunct option, particularly for patients with chronic bronchitis phenotype and frequent exacerbations. For pulmonology context, see our COPD page.
Outside COPD, NAC has been studied in idiopathic pulmonary fibrosis with mixed results (the IFIGENIA trial showed benefit, but the more rigorous PANTHER-IPF trial showed no benefit) and in cystic fibrosis where it complements but does not replace standard mucolytic therapy.
Contrast-Induced Nephropathy Prophylaxis
Iodinated contrast media (used in CT scans and cardiac catheterization) can precipitate acute kidney injury, particularly in patients with pre-existing chronic kidney disease, diabetes, or volume depletion. The mechanism involves direct renal tubular toxicity and oxidative stress at the renal medulla.
NAC was investigated as prophylaxis based on the rationale that boosting renal glutathione should mitigate the oxidative injury. The Tepel 2000 NEJM trial was the original positive study (600 mg twice daily orally for 4 doses bracketing contrast exposure). Many subsequent trials and meta-analyses produced inconsistent results, and the definitive PRESERVE trial (Weisbord 2018 NEJM, 5,000 patients) showed no benefit of NAC over placebo for the primary endpoint of death, dialysis, or sustained renal impairment.
Current professional society guidelines (ACR, KDIGO) no longer routinely recommend NAC for contrast nephropathy prophylaxis. Adequate IV hydration with isotonic saline before and after contrast remains the only well-supported preventive intervention. This is a useful cautionary example — positive small trials do not always replicate in large rigorous trials, and the appropriate humility about NAC's benefits in some indications.
Psychiatric Uses: OCD, Trichotillomania, Addiction, Bipolar
The psychiatric NAC literature is the most actively expanding area. The proposed mechanism centers on NAC's effect on the cystine-glutamate antiporter in the brain — restoring glutamate homeostasis in pathways implicated in compulsive behaviors and reward dysregulation. Notable trials:
Trichotillomania (compulsive hair-pulling) — Grant et al. Archives of General Psychiatry 2009 randomized 50 patients to NAC 1,200-2,400 mg/day or placebo for 12 weeks. The NAC group showed significant reduction in hair-pulling symptoms (56% responder rate vs 16% placebo). This is the strongest psychiatric trial for NAC and led to its adoption as a reasonable evidence-based intervention.
Obsessive-compulsive disorder — multiple small RCTs (Afshar 2012, Sarris 2015) of NAC 2,400-3,000 mg/day as augmentation to SSRI showed reduction in YBOCS scores. The augmentation effect is modest but useful in treatment-resistant cases. NAC is included in some treatment-resistant OCD algorithms.
Bipolar depression — Berk et al. Biological Psychiatry 2008 randomized 75 bipolar depression patients to NAC 2,000 mg/day or placebo as adjunct to standard treatment for 24 weeks. The NAC group showed significant improvement in MADRS depression scores. Multiple follow-up trials have generally supported this finding, though a large 2019 trial (CARMS) was negative.
Schizophrenia (negative symptoms) — Berk et al. Biological Psychiatry 2008 (second 2008 paper) randomized 140 schizophrenia patients to NAC 2,000 mg/day or placebo for 24 weeks. The NAC group showed improvement in negative symptoms (PANSS negative subscale). Multiple replications including the NAC-1 and NAC-2 trials.
Cocaine and cannabis dependence — small trials show NAC reduces craving and may help maintain abstinence. The proposed mechanism is the same glutamate-homeostasis pathway. Not standard of care, but a reasonable adjunct in resistant cases.
Autism spectrum disorder — small trials (Hardan 2012, Ghanizadeh 2013) of NAC 900-2,700 mg/day in children with autism showed modest reduction in irritability and stereotypy on parent-rated scales.
The aggregate psychiatric evidence is moderate but consistent enough that NAC is now a routine adjunct in functional and integrative psychiatry, and increasingly considered in academic psychiatry for treatment-resistant cases.
PCOS, Fertility, and Metabolic Applications
Polycystic ovary syndrome (PCOS) features insulin resistance, hyperandrogenism, oligo-ovulation, and chronic low-grade oxidative stress. NAC has been studied as an insulin-sensitizing and ovulation-supporting intervention with reasonable evidence base. The 2017 Cochrane review of NAC for PCOS pooled 8 RCTs and found:
- NAC increased ovulation rate compared to placebo and was comparable to metformin
- NAC plus clomiphene increased ovulation and pregnancy rates over clomiphene alone in clomiphene-resistant patients
- Modest improvements in insulin sensitivity (HOMA-IR) and lipid profiles
- No safety signals
Typical PCOS regimen: NAC 1,200-1,800 mg/day, often combined with inositol (myo-inositol 2 g twice daily). This combination is widely used in reproductive endocrinology, especially in patients who do not tolerate metformin.
For broader insulin resistance and metabolic syndrome, NAC has shown reductions in HOMA-IR and improvements in oxidative stress biomarkers. The 2021 GlyNAC trial by Kumar et al. in older adults with insulin resistance is the standout result — restoration of glutathione, mitochondrial function, insulin sensitivity, body composition, and gait speed in 24 weeks. The combination of glycine plus NAC outperformed historical NAC-monotherapy data, supporting the hypothesis that glycine is co-rate-limiting in aged tissues.
Dosing, Timing, and Quality
Dose-response data across the indications:
- Acetaminophen overdose — oral 1,330 mg/kg over 72 hours or IV 300 mg/kg over 21 hours. Hospital protocol; do not self-administer.
- COPD / chronic bronchitis — 600 mg twice daily; the PANTHEON 1,200 mg/day dose performed better than the BRONCUS 600 mg/day dose.
- PCOS — 1,200-1,800 mg/day divided into 2-3 doses.
- OCD / trichotillomania / bipolar depression — 1,200-2,400 mg/day starting at 600 mg twice daily, titrating up.
- Antiaging / general antioxidant — 600 mg once daily is reasonable for healthy adults; 600 mg twice daily for those with documented glutathione deficiency or significant oxidative stress.
- GlyNAC protocol — 100 mg/kg/day glycine + 100 mg/kg/day NAC, both divided into two daily doses, for 16-24 weeks. For a 70 kg adult this is 7 g of each per day — a substantial dose.
Quality considerations: NAC is one of the most adulterated supplement categories. The pharmaceutical-grade material used in clinical trials is white powder, faintly sulfurous odor. The cheapest internet-sourced NAC may be off-color (yellow tinge from oxidation), strong sulfurous odor, or below labeled potency. Reputable brands (USP-verified, NSF-certified, or sold by hospital pharmacies as Mucomyst-equivalent) are worth the price difference. Capsules generally tolerate better than powder because the sulfurous taste is masked.
Timing: NAC is moderately better tolerated with food (less GI upset) but can be taken on an empty stomach. The half-life of approximately 6 hours supports twice-daily dosing for clinical indications.
Glycine, Selenium, and the Other Synthesis Cofactors
Cysteine is the rate-limiting substrate for glutathione synthesis in most physiological conditions, but it is not the only substrate or cofactor. The complete pathway requires:
- Glycine — the second amino acid added by glutathione synthetase. Sekhar's work shows glycine is co-rate-limiting in older adults and many chronic disease states. Dietary glycine intake averages 3-5 g/day in Western diets but optimal intake for glutathione synthesis may be 5-15 g/day. Bone broth, gelatin, collagen powder, and pure glycine powder (5-10 g/day) are practical sources. Glycine also has independent benefits for sleep, blood-sugar regulation, and renal function.
- Glutamate — abundant in dietary protein; rarely limiting.
- Selenium — cofactor for glutathione peroxidase activity. The selenium status of US populations is generally adequate (200-watt-deficient areas have been mineralized by industrial agriculture); the RDA is 55 mcg/day and most adults consume 100-200 mcg from typical diets. Selenium-rich foods include Brazil nuts (1-2 per day provides 100-200 mcg), seafood, organ meats, and selenium-enriched yeast. Supplemental selenium 100-200 mcg/day is reasonable in known deficiency or high-oxidant-load states; chronic intake >400 mcg/day risks selenosis (hair loss, brittle nails, garlicky breath).
- NADPH — generated by the pentose phosphate pathway (G6PD enzyme). Not directly supplemented, but supported by adequate niacin status and glucose-6-phosphate availability.
- B-vitamins (especially B2 riboflavin, B6, B12, folate) — required for the transsulfuration pathway (homocysteine to cysteine via cystathionine beta-synthase, which is B6-dependent) and for general one-carbon metabolism. A B-complex with bioavailable forms (methylfolate, methylcobalamin, P5P) supports the upstream pathway.
- Magnesium — cofactor for multiple enzymes in glutathione synthesis and recycling.
The most efficient supplementation strategy for someone targeting glutathione is therefore not just NAC monotherapy but a stack: NAC 600 mg twice daily, glycine 5-10 g/day, B-complex with methylated forms, selenium 100-200 mcg/day (or 1-2 Brazil nuts), and adequate magnesium. Whole-food sources (whey protein, bone broth, allium vegetables for sulfur amino acids) further support the pathway.
Cautions, Drug Interactions, and the FDA Regulatory Dispute
- GI upset — the most common side effect (5-10% of users). Nausea, dyspepsia, occasionally diarrhea. Take with food and start at lower doses to acclimate.
- Sulfurous taste / odor — intrinsic to NAC; capsules minimize the issue compared to powders or effervescent tablets.
- Asthma / bronchospasm — nebulized NAC (Mucomyst) can trigger bronchospasm in susceptible patients; co-administer bronchodilator. Oral NAC does not cause this.
- Anaphylactoid reaction with IV NAC — approximately 0.2% risk during loading infusion for acetaminophen overdose protocol. Slower infusion rate reduces risk. Oral NAC has no analogous risk.
- Drug interactions: nitroglycerin — NAC potentiates the hypotensive and headache effects of nitrates; patients on nitrates should be cautious.
- Drug interactions: activated charcoal — in acetaminophen overdose, charcoal absorbs NAC and reduces its bioavailability if given simultaneously. Separate by 1-2 hours.
- Drug interactions: anticoagulants — theoretical potentiation of warfarin through cysteine effects on coagulation; monitor INR closely if combining at high doses.
- Bipolar I disorder — rare reports of NAC precipitating mania in initial weeks; introduce gradually under psychiatric supervision.
- Pregnancy — NAC is used in pregnancy for acetaminophen overdose without harm; routine high-dose supplementation outside that indication has limited data.
- Chemotherapy — theoretical concern that NAC could blunt oxidant-mediated antitumor effects of cisplatin, doxorubicin; discuss with oncologist before use during active chemo.
- FDA regulatory dispute — in 2020 the FDA sent warning letters classifying NAC as a drug (because it was approved as Mucomyst before any DSHEA supplement marketing) and not a legitimate dietary supplement. After industry pushback and litigation, the FDA in 2022 announced enforcement discretion allowing NAC to remain sold as a supplement pending rulemaking. As of 2026 the supplement status is preserved by enforcement discretion but the formal regulatory question remains unresolved. Major retailers (Amazon initially) briefly pulled NAC then restored it. Current consumer access is unimpeded but the regulatory backdrop is unstable.
Key Research Papers
- Prescott LF et al. (1979). Intravenous N-acetylcysteine: the treatment of choice for paracetamol poisoning. BMJ. — PubMed
- Smilkstein MJ et al. (1988). Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. NEJM. — PubMed
- Decramer M et al. (2005). Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost-Utility Study, BRONCUS). Lancet. — PubMed
- Zheng JP et al. (2014). Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON). Lancet Respiratory Medicine. — PubMed
- Tepel M et al. (2000). Prevention of radiographic-contrast-agent-induced reductions in renal function by acetylcysteine. NEJM. — PubMed
- Weisbord SD et al. (2018). Outcomes after angiography with sodium bicarbonate and acetylcysteine (PRESERVE). NEJM. — PubMed
- Grant JE et al. (2009). N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Archives of General Psychiatry. — PubMed
- Berk M et al. (2008). N-acetyl cysteine as a glutathione precursor for schizophrenia — a double-blind, randomized, placebo-controlled trial. Biological Psychiatry. — PubMed
- Berk M et al. (2008). N-acetyl cysteine for depressive symptoms in bipolar disorder — a double-blind randomized placebo-controlled trial. Biological Psychiatry. — PubMed
- Thakker D et al. (2015). N-acetylcysteine for polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled clinical trials. Obstetrics & Gynecology International. — PubMed
- Kumar P et al. (2021). GlyNAC supplementation in older adults improves glutathione deficiency. Clinical and Translational Medicine. — PubMed
- Aldini G et al. (2018). N-Acetylcysteine as an antioxidant and disulphide breaking agent: the reasons why. Free Radical Research. — PubMed
PubMed Topic Searches
- PubMed: NAC clinical trials
- PubMed: NAC for COPD
- PubMed: NAC psychiatric uses
- PubMed: NAC for acetaminophen OD
- PubMed: GlyNAC for aging
Connections
- NAC and Kidney Health — the renal half of the NAC evidence base — contrast-induced nephropathy from Tepel 2000 through the PRESERVE and ACT trials, chronic kidney disease, hemodialysis, and cystine stone prevention.
- NAC and Lung Health — the same molecule in the airways instead of the kidney — mucolytic disulfide-bond cleavage, the BRONCUS and PANTHEON COPD trials, IPF, and the Rumack-Matthew acetaminophen protocol.
- Oxidative Stress Hub
- Oxidative Stress Benefits Hub
- Glutathione Master Antioxidant
- Polyphenol Foods
- Mitochondrial Health
- Cysteine
- Glycine
- Selenium
- Vitamin B6
- Vitamin B2 (Riboflavin)
- COPD
- PCOS
- Hepatology (Liver Disease)
- Psychiatry
- Detoxification