Vitamin K2 for Bone Health
Vitamin K2 helps bone in one specific, well-understood way: it switches on osteocalcin, a protein that osteoblasts make to help lock calcium into the bone matrix. The molecular story is clean and not controversial. The clinical story is genuinely mixed and worth telling honestly. In Japan, a pharmacologic 45 mg dose of MK-4 (menatetrenone) is an approved osteoporosis drug with trial support for fewer fractures; in Western populations, nutritional-dose trials of MK-7 (around 180 mcg) have produced one strong positive bone-density result and several neutral ones, and the largest trial of high-dose K1 did not prevent fractures. This page lays out the mechanism, the Japanese data, the Western data, and the negative trials side by side — so you can see exactly where the confidence is high and where it is not.
Table of Contents
- How Vitamin K2 Acts on Bone
- Osteocalcin: The Gla Protein at the Center
- Undercarboxylated Osteocalcin as a Risk Marker
- The Japanese MK-4 (Menatetrenone) Osteoporosis Trials
- The Western MK-7 Trials (Nutritional Dose)
- The Negative Trials: ECKO and Emaus
- What the Evidence Actually Supports
- Working With Vitamin D, Calcium, and Magnesium
- Dosing, Forms, and Who Might Benefit
- Cautions (Warfarin First)
- Key Research Papers
- External Resources
- Connections
- Featured Videos
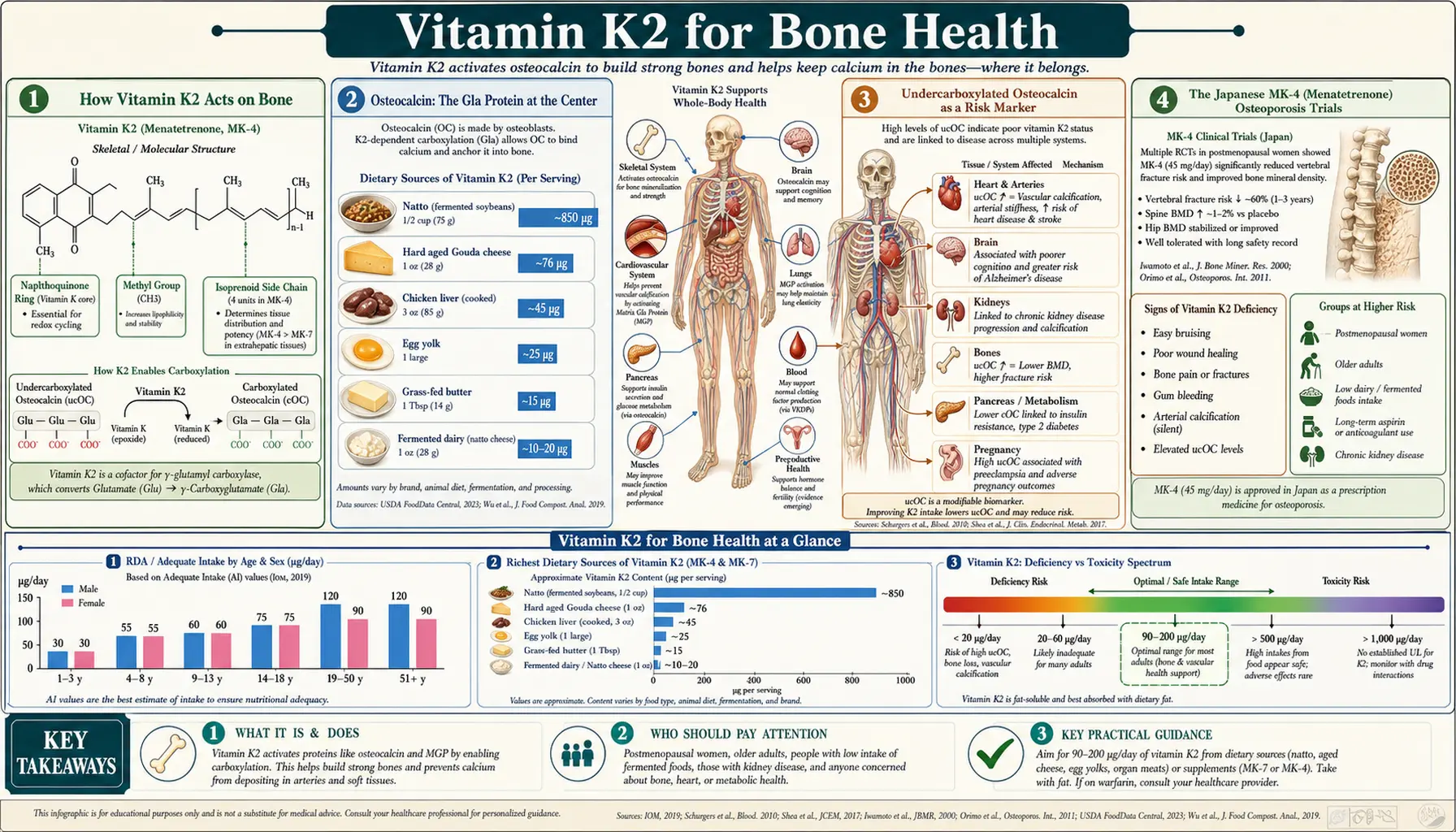
How Vitamin K2 Acts on Bone
Bone is not a static mineral rock; it is a living tissue that is continuously torn down by osteoclasts and rebuilt by osteoblasts. When osteoblasts lay down new bone, they secrete a protein called osteocalcin (also called bone Gla protein). Osteocalcin is the second most abundant protein in bone after collagen, and its job is to help organize and bind calcium into the growing hydroxyapatite crystal lattice.
But freshly made osteocalcin cannot bind calcium. It has to be chemically activated first, and that activation is a vitamin-K-dependent carboxylation. The enzyme gamma-glutamyl carboxylase, using vitamin K as an essential cofactor, converts three specific glutamate residues in osteocalcin into gamma-carboxyglutamate (Gla) residues. Each Gla residue carries an extra negative charge; together they form calcium-binding sites that let osteocalcin dock onto hydroxyapatite. Without enough vitamin K, osteocalcin is produced but remains undercarboxylated — present in the blood, but structurally unable to do its calcium-binding job in bone.
Vitamin K2, particularly the long-chain menaquinone MK-7, is especially effective at carboxylating osteocalcin because it circulates for days and reaches bone tissue efficiently. That extra-hepatic reach is the practical reason K2 is discussed for bone more than K1, even though both forms can drive the same carboxylation chemistry. The distinction between the forms is covered on the K2 vs K1 page.
Osteocalcin: The Gla Protein at the Center
Osteocalcin sits at the heart of nearly every claim about K2 and bone, so it is worth understanding precisely what it does and does not do. Carboxylated osteocalcin binds calcium ions and hydroxyapatite, and current understanding is that it helps regulate the maturation, alignment, and size of the mineral crystals in bone — contributing to bone quality (the structural competence of bone) as much as to bone quantity (mineral density measured by DXA). This is an important nuance: several K2 trials have shown effects on bone strength or fracture that are larger than their effects on measured bone mineral density, which fits a quality-over-quantity mechanism.
Osteocalcin has also emerged in research as a possible hormone with roles in glucose metabolism and energy balance, but that is a separate and still-evolving research area; for bone health, the calcium-binding, matrix-organizing role is the relevant one. The carboxylation status of osteocalcin — how much of it is fully activated — depends directly on vitamin K availability, which is why osteocalcin doubles as both a mechanism and a measurable marker of vitamin K sufficiency (Gundberg 2012).
Undercarboxylated Osteocalcin as a Risk Marker
Because undercarboxylated osteocalcin (ucOC) rises when vitamin K is insufficient, it can be measured in blood as a functional marker of vitamin K status — often more sensitive than measuring vitamin K itself. Several observational studies have found that higher ucOC (or a higher ratio of undercarboxylated to carboxylated osteocalcin) is associated with lower bone mineral density and higher hip-fracture risk in older adults, and controlled studies show that vitamin K supplementation reliably drives ucOC down (Binkley 2002). This gives K2's bone story a solid biomarker chain: more vitamin K → more carboxylated osteocalcin → a marker that tracks in the right direction.
The honest caveat is that a biomarker moving in the right direction is not the same as a fracture being prevented. ucOC responds to supplementation dependably; whether normalizing it translates into fewer real-world fractures in well-nourished people is exactly the question the clinical trials below were built to answer — and they do not all agree.
The Japanese MK-4 (Menatetrenone) Osteoporosis Trials
The strongest clinical evidence for vitamin K2 and bone comes from Japan, where MK-4 (menatetrenone) at a pharmacologic dose of 45 mg per day (typically 15 mg three times daily) is an approved osteoporosis treatment marketed as Glakay. This is a drug dose — roughly 250 times the amount of K2 you would get from a K2-rich diet — not a nutritional supplement dose, and that distinction matters enormously when reading the results.
The pivotal trial by Shiraki and colleagues (2000) randomized postmenopausal women with osteoporosis to 45 mg/day MK-4 or control. Over two years, the MK-4 group sustained lumbar bone mineral density while the control group lost it, and there were fewer new vertebral fractures in the treated group. Subsequent Japanese trials and the review by Iwamoto (2006) reported similar patterns — MK-4 appeared to reduce fracture incidence and preserve bone strength, sometimes with only modest effects on measured BMD, again pointing to a bone-quality mechanism.
Cockayne and colleagues (2006) pooled the available randomized trials in a meta-analysis and found that vitamin K supplementation was associated with reduced fractures, including a substantial reduction in hip and vertebral fractures. But they explicitly noted that the finding was driven by the Japanese MK-4 trials, several of which had methodological limitations (open-label designs, smaller sizes), and cautioned against over-reading the pooled number. So the fair summary of the Japanese data is: real, repeatedly positive, but obtained with a high pharmacologic dose in a specific population and with trials that would not all meet modern rigor standards.
The Western MK-7 Trials (Nutritional Dose)
Western research has focused on the long-acting menaquinone MK-7 at nutritional doses (around 180 mcg/day), because MK-7 is far more potent per microgram than MK-4 at raising carboxylation and stays in the blood for days. The standout study is the three-year randomized, placebo-controlled trial by Knapen and colleagues (2013): 244 healthy postmenopausal women took 180 mcg/day MK-7 or placebo. The MK-7 group had significantly less age-related decline in bone mineral density at the lumbar spine and femoral neck, and measures of bone strength (from DXA-derived geometry) were better preserved. An earlier Knapen study (2007) had similarly shown MK-7 improved hip bone geometry indices.
This is genuinely encouraging: a well-designed, adequately long RCT at a realistic supplement dose showing a bone-density benefit. It is the single best piece of Western evidence for K2 and bone. But one positive three-year trial in healthy (not osteoporotic) women, measuring bone density rather than fractures, is not the same as proof that K2 prevents fractures across the population — and the next section explains why that caution is warranted.
The Negative Trials: ECKO and Emaus
A responsible account of K2 and bone has to include the trials that did not show benefit, because they are real and they matter.
- ECKO trial (Cheung 2008) — 440 postmenopausal women with osteopenia received 5 mg/day of vitamin K1 or placebo for 2 to 4 years. This used K1 rather than K2, but at a high dose. The primary result was clear: vitamin K1 did not protect bone mineral density at the lumbar spine or hip. There were exploratory hints of fewer fractures and cancers, but these were secondary findings the authors themselves flagged as hypothesis-generating, not conclusions. On its main bone-density endpoint, ECKO was negative.
- Emaus 2010 — 334 early-menopausal Norwegian women received 360 mcg/day MK-7 (double the usual supplement dose) or placebo for one year. MK-7 did not influence bone loss. This is a direct nutritional-dose MK-7 trial in a Western population that came out neutral.
So we have a real tension: the three-year Knapen MK-7 trial was positive, the one-year Emaus MK-7 trial was neutral, and the high-dose K1 ECKO trial was negative for bone density. Trial length (bone changes are slow), the form of vitamin K, baseline bone status, and background vitamin K intake in the diet all plausibly contribute to the differences — but the bottom line is that Western nutritional-dose K2 has not delivered a consistent, fracture-level bone benefit.
What the Evidence Actually Supports
Putting the pieces together honestly:
- Mechanism — high confidence. K2 carboxylates osteocalcin; undercarboxylated osteocalcin is a valid marker of insufficiency; supplementation reliably improves it. This part is not in dispute.
- Pharmacologic MK-4 (45 mg) for osteoporosis — moderate confidence, mostly Japanese. Repeatedly positive for fracture and bone-strength endpoints, but at a drug dose, in a specific population, with trials of variable rigor. It is a licensed osteoporosis drug in Japan, not a food-level intervention.
- Nutritional MK-7 (~180 mcg) for bone — promising but unsettled. One strong positive 3-year density trial; other trials neutral. No large Western fracture-endpoint trial has confirmed it.
- K2 as a stand-alone fracture-prevention therapy in well-nourished Western adults — not established. The consistent, guideline-grade fracture reduction seen with, say, bisphosphonates has not been demonstrated for nutritional K2.
A reasonable, honest position: vitamin K2 is a plausible and low-risk contributor to bone health, best viewed as part of a complete bone-nutrition picture (adequate protein, calcium, vitamin D, magnesium, weight-bearing exercise) rather than as a proven fracture drug on its own — unless you are in the specific Japanese pharmacologic-MK-4 context. See our Osteoporosis page for the broader treatment landscape.
Working With Vitamin D, Calcium, and Magnesium
Vitamin K2 does not work in isolation, and the most sensible framing of its bone role is as one member of a cooperating group of nutrients:
- Vitamin D increases the body's production of osteocalcin (and matrix Gla protein), effectively creating more substrate for K2 to activate. Vitamin D also drives intestinal calcium absorption. The combined-therapy trial by Ushiroyama (2002) found K2 plus D3 supported bone density in postmenopausal women better than either alone in their comparison. See Vitamin D3 for bone health.
- Calcium is the mineral being managed. Osteocalcin and the whole K2 story are about handling calcium well; K2 does not replace adequate calcium intake. See Calcium for bone health.
- Magnesium is a cofactor in bone metabolism and vitamin D activation and is commonly under-consumed. See Magnesium.
The practical implication is that supplementing K2 while neglecting protein, calcium, vitamin D, magnesium, and exercise is unlikely to do much; K2's contribution is real but modest and depends on the rest of the foundation being in place.
Dosing, Forms, and Who Might Benefit
- MK-7 (nutritional): most Western trials and supplements use 90–200 mcg/day, with 180 mcg being the dose in the positive Knapen bone trial. MK-7 is fat-soluble — take it with a meal containing some fat for absorption.
- MK-4 (pharmacologic): the Japanese osteoporosis regimen is 45 mg/day (15 mg three times daily). This is a prescription-level dose used under medical care, not a general supplement recommendation. MK-4 clears quickly, which is why it is dosed multiple times per day.
- Food-first: natto is by far the richest dietary MK-7 source; aged cheeses, egg yolk, and animal foods contribute smaller amounts. Details are on the Sources & MK-4 vs MK-7 page.
- Who might reasonably consider it: postmenopausal women and older adults focused on bone quality, people with low dietary vitamin K, and (in Japan, under a physician) osteoporosis patients prescribed menatetrenone. It is not a substitute for evaluation and standard therapy in established osteoporosis.
Cautions (Warfarin First)
- Warfarin and other vitamin-K-antagonist anticoagulants (Coumadin, acenocoumarol, phenprocoumon) — this is the critical one. Vitamin K, including K2, directly opposes how these drugs work. Adding a K2 supplement can lower the INR and raise clotting risk, and changing your K intake up or down destabilizes anticoagulation. Do not start any vitamin K/K2 supplement while on warfarin without your prescriber's involvement. (The newer anticoagulants — apixaban, rivaroxaban, dabigatran — do not work through vitamin K and are not affected in this way, but confirm with your clinician.)
- Not a replacement for osteoporosis treatment — if you have diagnosed osteoporosis or a prior fragility fracture, K2 is at most adjunctive; it does not substitute for evaluation and guideline-based therapy.
- Generally well tolerated — nutritional-dose K2 has an excellent safety record with no established toxic upper limit, and even the 45 mg MK-4 drug dose is well tolerated. The main real-world hazard is the warfarin interaction above.
- Pregnancy/lactation and specific conditions — supplement use should be discussed with a clinician; food sources are fine.
Key Research Papers
- Gundberg CM, Lian JB, Booth SL (2012). Vitamin K-dependent carboxylation of osteocalcin: friend or foe? Advances in Nutrition. — PubMed 22516722
- Binkley NC et al. (2002). A high phylloquinone intake is required to achieve maximal osteocalcin gamma-carboxylation. Am J Clin Nutr. — PubMed 12399278
- Shiraki M et al. (2000). Vitamin K2 (menatetrenone) effectively prevents fractures and sustains lumbar bone mineral density in osteoporosis. J Bone Miner Res. — PubMed 10750566
- Iwamoto J et al. (2006). Menatetrenone (vitamin K2) and bone quality in the treatment of postmenopausal osteoporosis. Nutrition Reviews. — PubMed 17274493
- Cockayne S et al. (2006). Vitamin K and the prevention of fractures: systematic review and meta-analysis of RCTs. Arch Intern Med. — PubMed 16801507
- Knapen MHJ et al. (2013). Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporosis International. — PubMed 23525894
- Knapen MHJ et al. (2007). Vitamin K2 supplementation improves hip bone geometry and bone strength indices in postmenopausal women. Osteoporosis International. — PubMed 17287908
- Cheung AM et al. (2008). Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial). PLoS Medicine. — PubMed 18922041
- Emaus N et al. (2010). Vitamin K2 supplementation does not influence bone loss in early menopausal women. Osteoporosis International. — PubMed 19937427
- Booth SL et al. (2000). Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density. Am J Clin Nutr. — PubMed 10799384
- Ushiroyama T et al. (2002). Effect of continuous combined therapy with vitamin K2 and vitamin D3 on bone mineral density. Maturitas. — PubMed 11886767
- Vermeer C (2012). Vitamin K: the effect on health beyond coagulation — an overview. Food & Nutrition Research. — PubMed 22489224
PubMed Topic Searches
- PubMed: K2 & bone mineral density
- PubMed: undercarboxylated osteocalcin & fracture
- PubMed: menatetrenone (MK-4) & osteoporosis
- PubMed: MK-7 bone RCTs
- PubMed: K + D + calcium for bone
External Resources
- Linus Pauling Institute — Vitamin K (bone section)
- NIH ODS — Vitamin K Fact Sheet (Health Professionals)
- NIH Osteoporosis and Related Bone Diseases Resource Center
- MedlinePlus — Vitamin K (uses and interactions)
Connections
- Vitamin K2 Benefits Hub
- Vitamin K2 (Main Page)
- K2 & Arterial Calcification
- K2 vs K1 & the Calcium Paradox
- Sources & MK-4 vs MK-7
- Vitamin K (Benefits) — Bone Health
- Vitamin D3 for Bone Health
- Calcium for Bone Health
- Magnesium
- Osteoporosis
- Osteoporosis (Orthopedics)
- Natto
- Eggs
- Organ Meats
- All Vitamins