Vitamin E Toxicity: Symptoms, Causes, and Risks
Vitamin E is a fat-soluble antioxidant that the body cannot easily flush away, so unlike the water-soluble vitamins, a large excess can build up — but here is the most important and most reassuring fact: vitamin E toxicity essentially never comes from food. You cannot eat enough almonds, sunflower seeds, or olive oil to harm yourself. The problem comes almost entirely from high-dose supplements — the 400, 800, or 1,000 IU softgels many people once took daily believing more was better. The danger is also not the classic "poisoning" picture of nausea and collapse. Instead, vitamin E in large amounts gently thins the blood: it interferes with the way platelets clump and with vitamin K–dependent clotting, so the real risks are easy bruising and bleeding, a small but measurable increase in the most dangerous kind of stroke (bleeding into the brain), and a magnified effect when it is taken alongside blood-thinning medicines like warfarin or aspirin. Large trials have even linked high-dose vitamin E to a slightly higher overall death rate. None of this means a normal multivitamin or a vitamin-rich diet is dangerous — it means the old "megadose" habit was a mistake. This hub explains what counts as too much, why the harm centers on bleeding, why it is usually silent until something goes wrong, and what to do, with deep-dive pages on each major risk. If you take high-dose vitamin E, especially with any blood thinner, talk to your doctor or pharmacist before stopping or continuing.
Symptom Deep-Dive Pages
Bleeding & Bruising
The most common sign of too much vitamin E — how it impairs platelet clumping and clotting, why bruises appear easily or gums and nose bleed, and when this points to your supplement rather than something else.
Hemorrhagic Stroke Risk
The most serious concern — what large trials found about high-dose vitamin E and bleeding into the brain, how big the risk really is, and why this stroke signal is the strongest reason to avoid megadoses.
Blood-Thinner Interactions
Why vitamin E and medicines like warfarin, aspirin, or clopidogrel are a risky combination, how the effects stack, and the practical rules if you take both.
Table of Contents
- Symptom Deep-Dive Pages
- What Is Vitamin E Toxicity?
- Why Too Much Vitamin E Is Dangerous
- Why It Is Usually Silent
- What Causes Vitamin E Excess
- How It Is Diagnosed
- How Vitamin E Excess Is Managed
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
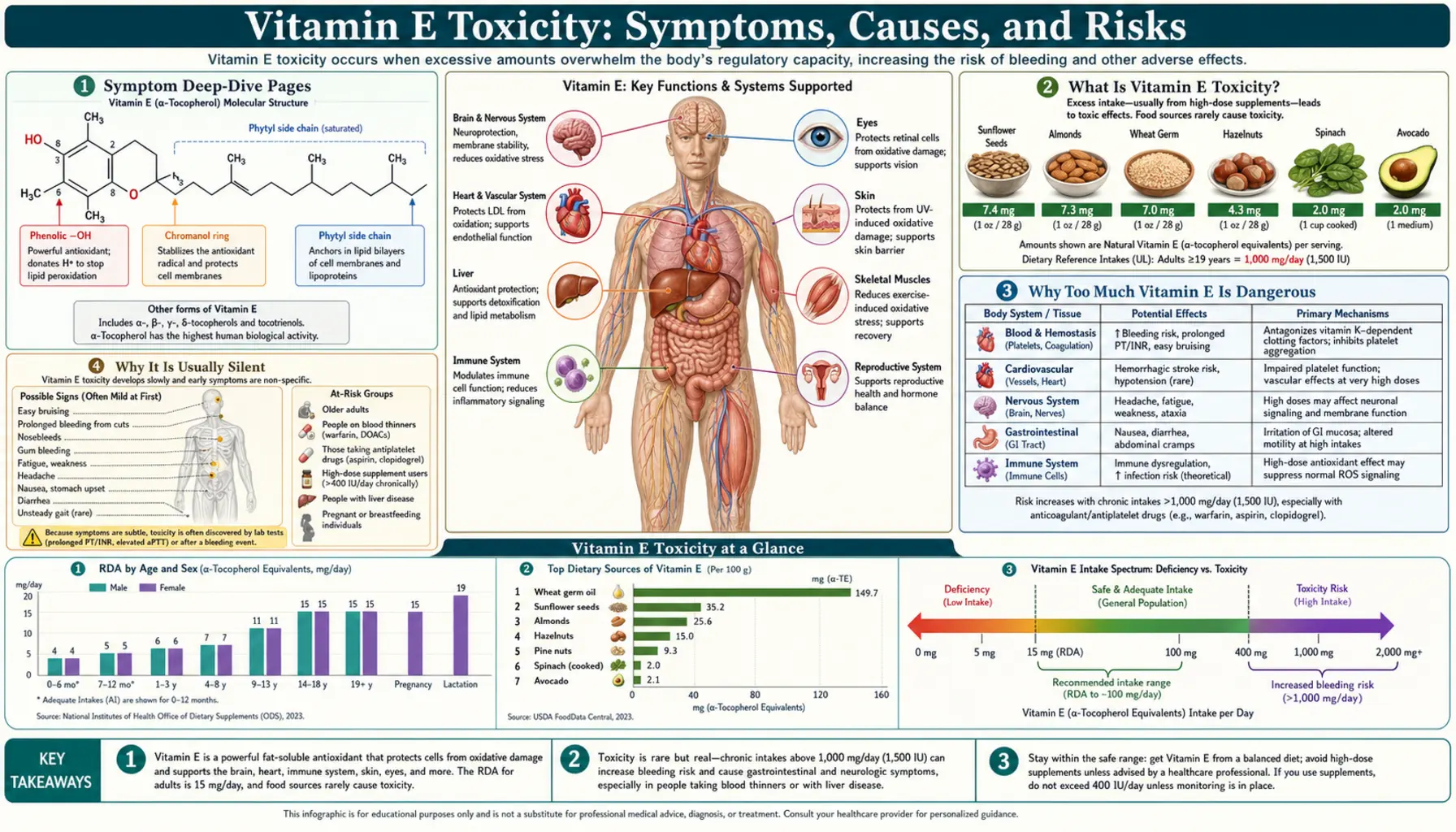
What Is Vitamin E Toxicity?
Vitamin E is the name for a family of eight fat-soluble compounds (four tocopherols and four tocotrienols); the form your body holds onto and the one used in most supplements is alpha-tocopherol. Because it dissolves in fat rather than water, vitamin E is stored in your liver and fatty tissues and is not rapidly excreted in urine the way vitamin C or the B vitamins are. That storage is exactly why a sustained excess is even possible — and why the vitamins most likely to build up to harmful levels are the fat-soluble ones (A, D, E, and K).
That said, the word "toxicity" can be misleading here. Vitamin E does not cause a dramatic acute poisoning. What it causes, at high enough doses over time, is a measurable tendency to bleed — and, in large studies, a small increase in the risk of dying from any cause and of suffering a bleeding stroke. So "vitamin E toxicity" really means the harms of chronic high-dose supplementation, not a single dangerous meal.
To make sense of "too much," it helps to know the reference amounts. The numbers below describe alpha-tocopherol, the active form:
- Recommended Dietary Allowance (RDA): about 15 mg/day for adults (roughly 22 IU of natural vitamin E, or 33 IU of the synthetic form). This is the everyday target, easily met by a normal diet.
- Tolerable Upper Intake Level (UL): 1,000 mg/day of supplemental alpha-tocopherol for adults — equal to about 1,500 IU of natural or 1,100 IU of synthetic vitamin E. The UL is the ceiling that the U.S. Food and Nutrition Board judged unlikely to cause harm; it was set specifically because of the bleeding risk seen at high intakes.
- The gap is enormous. The UL is more than 60 times the RDA. That wide margin is one reason food can never get you into trouble — but it also lulled people into thinking megadose softgels were harmless, which the evidence below challenges.
One nuance worth holding onto: the UL is a regulatory ceiling, not a fully reassuring "safe" line. As the research section explains, some large trials found a small increase in all-cause mortality at supplement doses at or even below the UL (in the range of 400–800 IU/day). The practical takeaway is simpler than the numbers: there is no demonstrated benefit to taking large vitamin E supplements for the general population, and there is some signal of harm, so high-dose vitamin E is best avoided unless a doctor has a specific reason to prescribe it.
Why Too Much Vitamin E Is Dangerous
If a normal amount of vitamin E is helpful and even a large amount rarely makes you feel sick, why is excess taken seriously? The answer comes down to one theme: bleeding. High-dose vitamin E gently interferes with the body's ability to form clots, and from that single mechanism flow nearly all of its recognized harms.
There are two complementary reasons vitamin E thins the blood, and it helps to picture clotting as a two-part system. The first part is the platelets — tiny cell fragments that rush to a wound and stick together to form the initial plug. The second part is the clotting cascade, a chain of proteins (several of which depend on vitamin K) that reinforces that plug into a stable clot. Vitamin E, in large amounts, dampens both:
- It makes platelets less sticky. Alpha-tocopherol reduces platelet aggregation — the clumping step — so the first plug forms less readily. This is the same kind of effect (though milder) that aspirin produces, which is why the two add together.
- It works against vitamin K. This is the more specific and elegant mechanism. Inside the body, vitamin E can be converted to a compound called tocopheryl quinone, whose shape resembles vitamin K. It can interfere with the vitamin K–dependent enzymes that activate clotting factors II, VII, IX, and X — in effect acting as a mild vitamin K antagonist, the same general lever that the drug warfarin pulls. Laboratory work has shown this quinone has genuine anticlotting activity, and human studies have measured small reductions in vitamin K–dependent clotting markers in people taking high-dose vitamin E.
From this one bleeding tendency, the three concrete dangers follow:
- Easy bruising and bleeding. The most common and visible sign — bruises from minor knocks, bleeding gums, nosebleeds, or bleeding that is slow to stop. This is covered in depth on the Bleeding & Bruising page.
- Hemorrhagic (bleeding) stroke. The most serious concern. A bleeding tendency in the brain's small vessels can, in a small number of people, tip the balance toward a hemorrhagic stroke. Several large trials and a meta-analysis found that high-dose vitamin E modestly increased the risk of this specific (and especially deadly) stroke type, even as it had little effect on the more common clot-type (ischemic) stroke. The Hemorrhagic Stroke Risk page lays out exactly what the studies found and how large the risk really is.
- Amplified blood thinners. Because vitamin E thins the blood on its own, adding it to a prescribed blood thinner — warfarin, aspirin, clopidogrel, or the newer direct oral anticoagulants — can push the combined effect into dangerous territory, raising the risk of a serious bleed. See Blood-Thinner Interactions.
One honest caveat about scale: for a healthy person taking a normal multivitamin, none of this is a meaningful worry — the bleeding effect is dose-dependent and only becomes clinically important at high supplemental doses, or at lower doses when combined with another blood thinner. The danger is real, but it is a danger of megadosing, not of vitamin E itself.
Why It Is Usually Silent
Like many vitamin and electrolyte problems, an excess of vitamin E rarely announces itself. There is no number on a routine panel that doctors watch for vitamin E, no characteristic feeling of being "over-dosed," and often no symptom at all until a bleeding event reveals the problem. A person can take 800 IU a day for years and feel completely normal, while their blood is quietly a little slower to clot than it should be.
Why so quiet? Because the body's clotting system has reserve. A mild, vitamin-E–induced reduction in platelet stickiness and clotting-factor activity usually does not matter day to day — small cuts still stop, and life goes on. The effect only becomes visible when it is unmasked: by a fall or surgery that calls on the clotting system, by another blood thinner that pushes the total effect over the edge, or by the rare but catastrophic event of a brain bleed. In other words, the calm is real, but it is not the same as safety — the margin for error has narrowed without any warning sensation.
This silence is exactly why the safe approach is preventive rather than symptom-driven. You cannot rely on your body to tell you that your vitamin E intake is too high. Instead, the protection comes from knowing what you take and why:
- Read your supplement labels. Add up vitamin E from every source — a standalone vitamin E softgel, a multivitamin, and any "antioxidant," "heart," "eye health," or "anti-aging" formula can each contain it. Doses are often listed in IU; the UL of 1,000 mg corresponds to roughly 1,500 IU natural / 1,100 IU synthetic.
- Tell every clinician what you take. Surgeons, dentists, and anyone prescribing a blood thinner need to know about high-dose vitamin E specifically, because it changes bleeding risk. It is commonly stopped before surgery.
- Be most cautious if you are already on a blood thinner — this is the setting where a "silent" vitamin E effect most often turns into a real bleed.
The take-home is the opposite of reassuring quiet: feeling fine is not evidence that a high-dose habit is safe. With vitamin E, the dose on the bottle tells you more than how you feel.
What Causes Vitamin E Excess
Vitamin E excess has, in practice, essentially one cause: supplements. Unlike many minerals, there is no common medical condition or hormone problem that pushes vitamin E up on its own. Here is what actually drives high intake, from most to least relevant.
- High-dose single-vitamin supplements — the number-one cause. For decades vitamin E was marketed as a heart-protective, anti-aging antioxidant, and softgels of 400, 800, even 1,000 IU were taken daily by millions. A single 1,000 IU capsule already approaches or exceeds the UL, and these were often taken on top of other sources. This megadose habit — not diet — is the origin of nearly every documented harm.
- Stacking from multiple products. A surprisingly common, hidden route. Vitamin E turns up in multivitamins, "antioxidant complexes," combined eye-health formulas (such as some macular-degeneration blends), skin and hair supplements, and heart formulas. Someone taking several of these can unknowingly add up to a large daily total even without a dedicated high-dose E capsule.
- The mistaken belief that "more is better." Because vitamin E is an antioxidant and antioxidants sound healthy, people have assumed that large doses must be extra-protective. The large trials summarized below firmly contradict this: higher doses did not deliver the hoped-for protection against heart disease or cancer, and at the high end they were associated with a small increase in mortality and in hemorrhagic stroke.
- Food — essentially never a cause. This is the crucial reassurance. Vitamin E–rich whole foods — almonds, sunflower seeds, hazelnuts, peanuts, wheat germ, spinach and other greens, avocado, and vegetable oils — provide modest amounts (a generous handful of almonds gives only around 7–8 mg, about half a day's RDA). There is no realistic way to eat enough to reach toxic intakes. A diet rich in these foods is healthy and carries none of the supplement risks; see Vitamin E Food Sources, Almonds, and Spinach.
- Topical vitamin E — not a source of internal excess. Vitamin E oil applied to skin (a common skin-care ingredient) is not absorbed in amounts that affect the whole body, so it does not contribute to systemic toxicity. Its main downside is the occasional skin allergy.
The pattern is the opposite of vitamins where diet and disease drive the level: with vitamin E, the question to ask is never "what is my body doing?" but simply "how much am I swallowing, from how many bottles?"
How It Is Diagnosed
There is no routine, widely ordered blood test that screens for vitamin E excess the way a metabolic panel screens for potassium or calcium. A serum alpha-tocopherol level can be measured, but it is a specialized test used mainly to investigate deficiency (or rare fat-absorption disorders), and it correlates poorly with the bleeding risk that actually matters at high intakes. In real life, vitamin E excess is recognized not by a lab number but by putting the pieces together: a high-dose supplement habit plus a bleeding tendency.
The practical diagnostic path looks like this:
- The medication and supplement history is the key step. When someone presents with unexplained bruising, frequent nosebleeds, bleeding gums, or a more serious bleed, a careful clinician asks specifically about all supplements — including the ones people forget to mention because they seem harmless. Discovering 800 or 1,000 IU of vitamin E daily, or several products that each contain it, often explains the picture.
- Coagulation testing measures the effect, not the vitamin. Rather than measuring vitamin E itself, doctors assess how the blood is clotting. A coagulation panel — including prothrombin time (PT) and its standardized version, the INR — can reveal a prolonged clotting time, reflecting the vitamin K–dependent effect. This is especially important in anyone taking warfarin, where vitamin E can push the INR higher. See the Coagulation Panel page for what PT/INR mean.
- A confirmatory clue: the problem improves when the supplement stops. Because vitamin E is not a drug with a precise antidote, one of the most telling signs is that an unexplained bleeding tendency resolves over days to weeks after high-dose vitamin E is discontinued (sometimes helped along by vitamin K). A bleeding tendency that clears after stopping the supplement strongly implicates it.
- Ruling out other causes. Bleeding and bruising have many explanations — other medications (aspirin, anticoagulants), liver disease, low platelets, vitamin K deficiency, and inherited clotting disorders among them. Part of diagnosis is making sure vitamin E is the cause and not a coincidence, which is why the full picture (dose, timing, other drugs, and clotting tests) matters more than any single result.
The bottom line: do not expect a "vitamin E level" to be the answer. The diagnosis is usually clinical — a high-dose habit plus a bleeding problem, supported by clotting tests — and the most useful single action is often simply a careful review of everything a person is taking.
How Vitamin E Excess Is Managed
The good news is that managing vitamin E excess is usually straightforward, because the body slowly clears stored vitamin E once the intake stops, and the bleeding effect is reversible. The cornerstone is simple: stop the source.
- Discontinue the high-dose supplement. This is the single most important step and is appropriate for almost everyone — there is no general-population benefit to high-dose vitamin E that would justify continuing it. Stop the dedicated softgel and review every other product (multivitamins, antioxidant blends, eye-health formulas) so the total intake drops to ordinary dietary levels. Because vitamin E is fat-soluble and stored, the bleeding tendency eases over days to a few weeks rather than instantly, as tissue stores fall.
- Address active bleeding directly. Minor issues (the occasional bruise or nosebleed) usually need nothing more than stopping the supplement and ordinary first aid. A significant or ongoing bleed is treated on its own merits, in a medical setting.
- Vitamin K when clotting is impaired. Because much of vitamin E's effect works against vitamin K, giving vitamin K can help restore normal clotting — particularly when the PT/INR is prolonged or bleeding is significant. This is a medical decision, not a do-it-yourself fix, and it is especially delicate in people taking warfarin (whose entire treatment is built around vitamin K).
- Coordinate carefully with any blood thinner. For someone on warfarin, aspirin, clopidogrel, or a direct oral anticoagulant, both starting and stopping high-dose vitamin E can shift bleeding risk, so changes should be made with the prescribing clinician, often with INR re-checks for warfarin users. Never adjust an anticoagulant on your own to "make room" for a supplement. The Blood-Thinner Interactions page covers this in detail.
- Plan ahead for surgery and dental work. High-dose vitamin E is commonly stopped a couple of weeks before planned procedures to reduce bleeding risk — tell your surgeon, anesthetist, and dentist what you take.
What you generally do not need is dramatic intervention: there is no dialysis or chelation for vitamin E. The contrast with the Deficiency side is instructive — there the goal is to raise intake, here it is simply to lower it back to what food provides. For most people, "stop the megadose and eat a normal, vitamin-E–rich diet" is the entire treatment.
When to Seek Care / Red Flags
Because vitamin E excess is usually silent, the most useful "red flag" is often a situation rather than a feeling: if you take high-dose vitamin E — especially together with a blood thinner — that alone is a reason to review it with a doctor or pharmacist, even if you feel completely well. Beyond that, certain symptoms mean bleeding may be a genuine problem and warrant prompt attention. Seek emergency care immediately for any sign of serious or brain bleeding:
- A sudden, severe "thunderclap" headache, the worst of your life — a possible sign of bleeding in or around the brain.
- Sudden weakness or numbness on one side, trouble speaking, vision loss, confusion, or loss of coordination — warning signs of a stroke, including the hemorrhagic (bleeding) type. Call emergency services at once; do not wait.
- Bleeding that will not stop, or a large/expanding bruise after a minor injury.
- Blood in the stool (red or black, tarry) or vomit (red or coffee-ground colored), or coughing or vomiting blood — possible internal bleeding.
- Pink, red, or brown urine, or unusually heavy menstrual bleeding.
Contact your doctor (not necessarily an emergency, but soon) if you notice easy or unexplained bruising, frequent nosebleeds, or bleeding gums that are new for you — particularly if you take high-dose vitamin E, are on any blood thinner, or have a procedure coming up. People at higher risk — anyone combining vitamin E with warfarin, aspirin, clopidogrel, or a direct oral anticoagulant, those with liver disease or a known clotting disorder, and anyone scheduled for surgery — should have a low threshold to get checked, because in these settings a quiet bleeding tendency is most likely to become a real bleed. For the broader stroke picture, see Stroke.
Key Research Papers
- Miller ER 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E (2005). Meta-Analysis: High-Dosage Vitamin E Supplementation May Increase All-Cause Mortality. Annals of Internal Medicine;142(1):37-46. — DOI: 10.7326/0003-4819-142-1-200501040-00110
- Abner EL, Schmitt FA, Mendiondo MS, Marcum JL, Kryscio RJ (2011). Vitamin E and All-Cause Mortality: A Meta-Analysis. Current Aging Science;4(2):158-170. — DOI: 10.2174/1874609811104020158
- Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C (2012). Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database of Systematic Reviews;(3):CD007176. — DOI: 10.1002/14651858.CD007176.pub2
- Sesso HD, Buring JE, Christen WG, et al. (2008). Vitamins E and C in the Prevention of Cardiovascular Disease in Men: The Physicians' Health Study II Randomized Controlled Trial. JAMA;300(18):2123-2133. — DOI: 10.1001/jama.2008.600
- Lonn E, Bosch J, Yusuf S, et al. (HOPE and HOPE-TOO Trial Investigators) (2005). Effects of Long-term Vitamin E Supplementation on Cardiovascular Events and Cancer. JAMA;293(11):1338-1347. — DOI: 10.1001/jama.293.11.1338
- Schürks M, Glynn RJ, Rist PM, Tzourio C, Kurth T (2010). Effects of vitamin E on stroke subtypes: meta-analysis of randomised controlled trials. BMJ;341:c5702. — DOI: 10.1136/bmj.c5702
- Leppälä JM, Virtamo J, Fogelholm R, et al. (2000). Controlled Trial of Alpha-Tocopherol and Beta-Carotene Supplements on Stroke Incidence and Mortality in Male Smokers. Arteriosclerosis, Thrombosis, and Vascular Biology;20(1):230-235. — DOI: 10.1161/01.ATV.20.1.230
- Klein EA, Thompson IM Jr, Tangen CM, et al. (2011). Vitamin E and the Risk of Prostate Cancer: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA;306(14):1549-1556. — DOI: 10.1001/jama.2011.1437
- Booth SL, Golly I, Sacheck JM, et al. (2004). Effect of vitamin E supplementation on vitamin K status in adults with normal coagulation status. American Journal of Clinical Nutrition;80(1):143-148. — DOI: 10.1093/ajcn/80.1.143
- Dowd P, Zheng ZB (1995). On the mechanism of the anticlotting action of vitamin E quinone. Proceedings of the National Academy of Sciences;92(18):8171-8175. — DOI: 10.1073/pnas.92.18.8171
- Traber MG (2014). Vitamin E Inadequacy in Humans: Causes and Consequences. Advances in Nutrition;5(5):503-514. — DOI: 10.3945/an.114.006254
- Corrigan JJ Jr, Marcus FI (1974). Coagulopathy associated with vitamin E ingestion (a classic case of warfarin potentiation by high-dose vitamin E). JAMA;230(9):1300-1301. — PubMed
PubMed Topic Searches
- PubMed — High-dose vitamin E supplementation and all-cause mortality
- PubMed — Vitamin E and hemorrhagic stroke risk
- PubMed — Vitamin E, warfarin, and anticoagulant interaction
- PubMed — Vitamin E, platelet aggregation, and vitamin K–dependent clotting
- PubMed — Alpha-tocopherol upper intake level and toxicity
Connections
- Vitamin E Toxicity: Bleeding & Bruising
- Vitamin E Toxicity: Hemorrhagic Stroke Risk
- Vitamin E Toxicity: Blood-Thinner Interactions
- Vitamin E Overview
- Vitamin E Deficiency Hub
- Vitamin E Benefits Hub
- Vitamin E Food Sources
- Vitamin K
- Vitamin K2
- Coagulation Panel (PT / INR)
- Stroke
- Almonds
- Spinach
- Olive Oil