Natural Anxiety Relief — Benefits Deep Dive
Anxiety is the most common mental health condition worldwide, affecting roughly 301 million people in the most recent Global Burden of Disease estimate. Pharmaceutical first-line therapy (SSRIs, SNRIs, buspirone, and short-term benzodiazepines) has well-documented efficacy but also a familiar tail of side effects — sexual dysfunction, weight change, emotional blunting, dependence risk, and a discontinuation syndrome that can last months. The four deep-dive pages below cover the natural-medicine modalities with the strongest published evidence base for anxiety reduction: L-theanine and green tea (alpha-wave generation and glutamate modulation), magnesium glycinate (NMDA receptor antagonism and HPA-axis dampening), adaptogenic herbs (ashwagandha, rhodiola, holy basil, and the stress-resilience literature), and the body-based interventions of slow nasal breathing and deliberate cold exposure (vagal tone, locus coeruleus norepinephrine, and dopamine reset).
Deep-Dive Articles
L-Theanine & Green Tea
The non-protein amino acid that gives green tea its distinctive calm-but-alert effect. Mechanism via glutamate-receptor antagonism, GABA and dopamine modulation, alpha-wave generation on EEG (8–13 Hz), and synergy with caffeine to dampen jitteriness. Effective dose 200–400 mg one to three times daily, with the strongest published evidence in acute stress-task studies and chronic generalized anxiety.
Magnesium Glycinate
The form of magnesium with the cleanest gut tolerability for the doses required to influence anxiety. Mechanism via NMDA-receptor antagonism, GABA-A potentiation, calcium-channel modulation, and HPA-axis dampening through cortisol suppression. Why glycinate is preferred over oxide for anxiety, why citrate is preferred for constipation, dosing 200–400 mg elemental magnesium nightly, and the surprisingly large overlap between subclinical hypomagnesemia and treatment-refractory anxiety.
Adaptogenic Herbs
Ashwagandha (the most studied, with at least nine RCTs showing 25–45% cortisol reduction), rhodiola rosea (the Russian-military fatigue-and-anxiety adaptogen), holy basil / tulsi (the Ayurvedic everyday adaptogen), and lemon balm (the gentler GABAergic herb). Mechanism via HPA-axis recalibration, GABAergic activity, and Hsp70 / Nrf2 stress-response activation. Dosing, standardized extracts (KSM-66, Sensoril, SHR-5), and the contraindications that matter.
Breath & Cold Exposure
The two body-based interventions with the strongest acute effect on the autonomic nervous system. Slow nasal breathing (4–6 breaths per minute, extended exhale) raises vagal tone and reduces sympathetic outflow within minutes. Deliberate cold exposure (cold shower, cold plunge, face immersion) triggers the mammalian dive reflex and produces a sustained 250% dopamine and 530% norepinephrine elevation that resets baseline mood for hours. Wim Hof method, physiological sigh, box breathing, and the vagus-nerve research base.
Table of Contents
- Deep-Dive Articles
- Why Natural Anxiety Relief Works (and When It Doesn't)
- Research Papers: L-Theanine & Green Tea
- Research Papers: Magnesium Glycinate
- Research Papers: Adaptogenic Herbs
- Research Papers: Breath & Cold Exposure
- Research Papers: Cross-Cutting (HPA Axis, GABA, Vagal Tone)
- External Authoritative Resources
- Connections
- Featured Videos
Why Natural Anxiety Relief Works (and When It Doesn't)
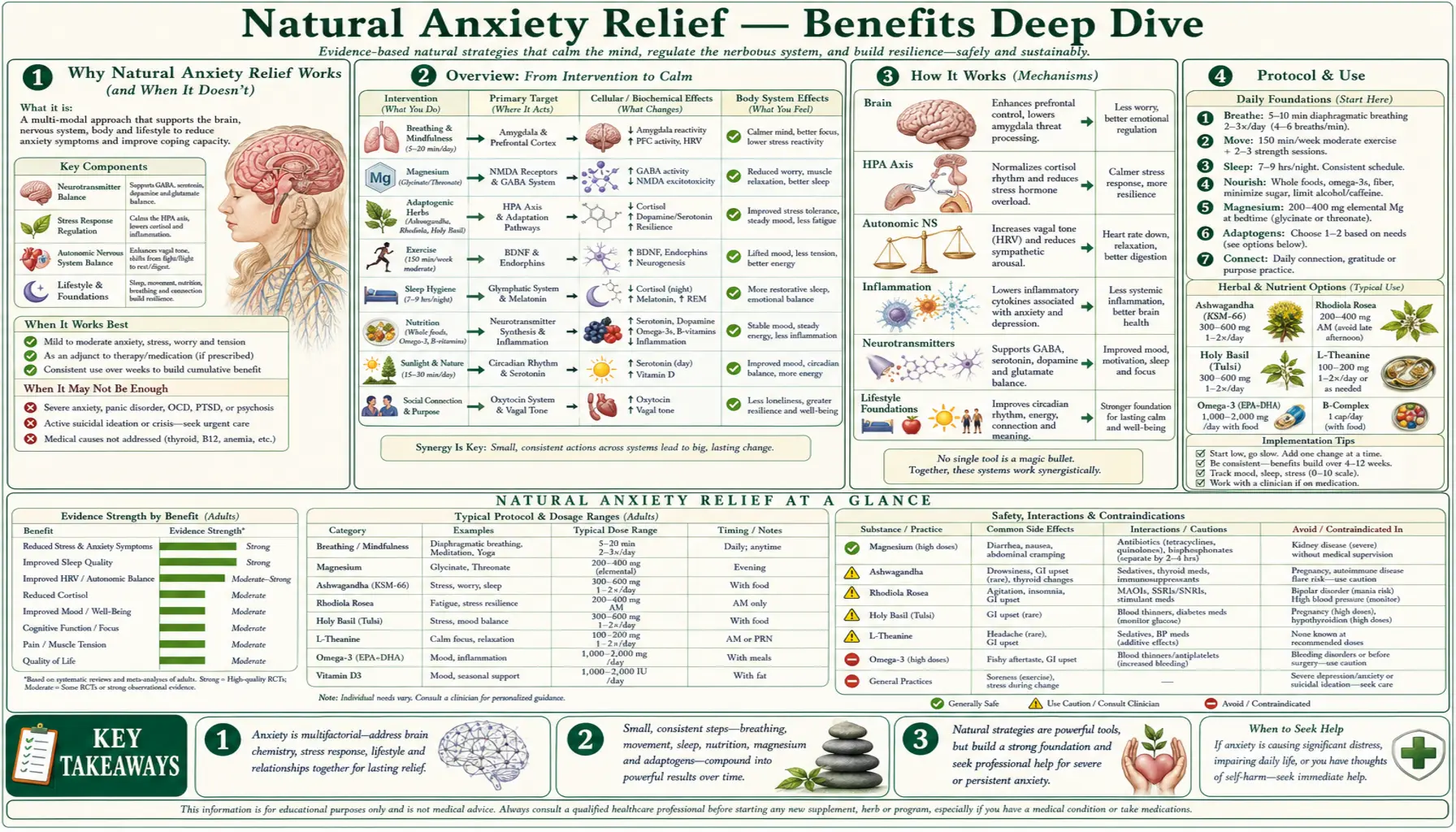
Anxiety is best understood as a disorder of threat-detection calibration. The amygdala, locus coeruleus, hypothalamic-pituitary-adrenal (HPA) axis, sympathetic nervous system, and prefrontal cortex form a circuit that evaluates incoming stimuli for threat and mounts a stereotyped fight-or-flight response when the threat-detection threshold is crossed. In healthy anxiety, that threshold is calibrated to genuine danger. In clinical anxiety disorders, the threshold has been lowered — either by acute stressors (recent trauma, chronic medical illness, substance use) or by chronic structural changes (early-life adversity, persistent inflammation, sleep deprivation, mineral deficiency, or genetic predisposition).
Pharmacological treatment works at specific points on this circuit. SSRIs increase serotonergic tone in the dorsal raphe-amygdala pathway over a six-to-eight-week induction period. Benzodiazepines acutely amplify GABA-A signaling at the chloride channel. Buspirone is a 5-HT1A partial agonist that takes two to four weeks. Each is effective for the right patient, but each carries a side-effect profile that some patients find unacceptable or cannot tolerate — and roughly one-third of patients with generalized anxiety disorder do not achieve adequate response to first-line pharmacotherapy.
The four natural-medicine modalities covered in this Benefits hub work at parallel points on the same circuit and have published evidence for clinical benefit:
- Amino-acid and nutrient repletion (L-theanine and magnesium glycinate) supplies the molecular substrates required for inhibitory neurotransmission. L-theanine produces a measurable EEG alpha-wave shift within 30–40 minutes of an oral 200 mg dose. Magnesium acts as the physiological NMDA-receptor blocker and is an obligatory cofactor for GABA-A receptor function — the same mechanism leveraged by benzodiazepines, except via the upstream substrate rather than the receptor pharmacology.
- Adaptogenic herbs (ashwagandha, rhodiola, holy basil, lemon balm) act on the HPA axis itself, dampening cortisol output and improving the resilience of the stress response over four-to-twelve-week courses. The best-studied of these, ashwagandha (KSM-66 and Sensoril extracts), has at least nine published RCTs showing 20–45% reduction in morning serum cortisol with concurrent improvement on validated anxiety scales.
- Body-based interventions (slow nasal breathing and deliberate cold exposure) reset the autonomic nervous system through afferent vagal signaling. Slow-paced breathing at 4–6 breaths per minute resonates with the baroreflex feedback loop and increases vagal tone within minutes. Cold exposure activates the mammalian dive reflex, suppresses sympathetic output, and produces a sustained dopamine and norepinephrine elevation that persists for hours after the stimulus has ended.
The clinical reality is that natural anxiety relief works well in three settings: subclinical or mild anxiety where pharmaceutical therapy is not yet indicated; as an adjunct to standard therapy where partial response leaves residual symptoms; and as a bridge during SSRI induction or taper, where 6–8 weeks of subtherapeutic medication coverage can be supplemented with faster-acting natural modalities. It works less well as monotherapy in severe panic disorder, PTSD with acute flashbacks, or anxiety with comorbid psychosis — settings where pharmaceutical intervention is the appropriate first line.
The honest framing is that natural anxiety relief is not a replacement for psychiatric care in moderate-to-severe disease. It is, however, a substantial supplement that addresses underlying physiological dysregulation rather than masking symptoms — and for many patients with mild-to-moderate anxiety, it produces clinically meaningful improvement at lower cost and with fewer side effects than first-line pharmacotherapy.
Research Papers: L-Theanine & Green Tea
- Nobre AC et al. (2008). L-theanine, a natural constituent in tea, and its effect on mental state. Asia Pacific Journal of Clinical Nutrition. — PubMed: Nobre alpha-wave EEG
- Williams JL et al. (2020). The effects of green tea amino acid L-theanine on mental health. Plant Foods for Human Nutrition. — PubMed: Williams systematic review
- Hidese S et al. (2019). Effects of L-theanine administration on stress-related symptoms and cognitive function. Nutrients. — PubMed: Hidese Nutrients 2019
- Kimura K et al. (2007). L-theanine reduces psychological and physiological stress responses. Biological Psychology. — PubMed: Kimura stress response
- Lardner AL (2014). Neurobiological effects of the green tea constituent theanine. Nutritional Neuroscience. — PubMed: Lardner mechanism review
- Owen GN et al. (2008). The combined effects of L-theanine and caffeine on cognitive performance and mood. Nutritional Neuroscience. — PubMed: Owen L-theanine + caffeine
- Yoto A et al. (2012). Effects of L-theanine or caffeine intake on changes in blood pressure under physical and psychological stresses. Journal of Physiological Anthropology. — PubMed: Yoto BP and stress
- Sarris J et al. (2019). L-theanine in the adjunctive treatment of generalized anxiety disorder. Journal of Psychiatric Research. — PubMed: Sarris GAD adjunctive
- Lu K et al. (2004). The acute effects of L-theanine in comparison with alprazolam on anticipatory anxiety. Human Psychopharmacology. — PubMed: Lu vs alprazolam
- Higashiyama A et al. (2011). Effects of L-theanine on attention and reaction time response. Journal of Functional Foods. — PubMed: Higashiyama attention
Research Papers: Magnesium Glycinate
- Boyle NB et al. (2017). The effects of magnesium supplementation on subjective anxiety and stress: a systematic review. Nutrients. — PubMed: Boyle systematic review
- Pickering G et al. (2020). Magnesium status and stress: the vicious circle concept revisited. Nutrients. — PubMed: Pickering stress cycle
- Sartori SB et al. (2012). Magnesium deficiency induces anxiety and HPA axis dysregulation. Neuropharmacology. — PubMed: Sartori HPA dysregulation
- Eby GA, Eby KL (2010). Magnesium for treatment-resistant depression: a review and hypothesis. Medical Hypotheses. — PubMed: Eby treatment-resistant
- De Baaij JHF et al. (2015). Magnesium in man: implications for health and disease. Physiological Reviews. — PubMed: De Baaij comprehensive
- Tarleton EK et al. (2017). Role of magnesium supplementation in the treatment of depression: a randomized clinical trial. PLoS ONE. — PubMed: Tarleton RCT
- Jacka FN et al. (2009). Association between magnesium intake and depression and anxiety. Australian and New Zealand Journal of Psychiatry. — PubMed: Jacka population data
- Cuciureanu MD, Vink R (2011). Magnesium and stress. In Magnesium in the Central Nervous System. — PubMed: Cuciureanu chapter
- Slutsky I et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron. — PubMed: Slutsky L-threonate
- Walker AF et al. (2003). Mg citrate found more bioavailable than other Mg preparations. Magnesium Research. — PubMed: Walker bioavailability
Research Papers: Adaptogenic Herbs
- Chandrasekhar K et al. (2012). Prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety. Indian Journal of Psychological Medicine. — PubMed: Chandrasekhar 2012
- Lopresti AL et al. (2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract. Medicine (Baltimore). — PubMed: Lopresti KSM-66
- Salve J et al. (2019). Adaptogenic and anxiolytic effects of ashwagandha root extract in healthy adults. Cureus. — PubMed: Salve healthy adults
- Panossian A, Wikman G (2010). Effects of adaptogens on the central nervous system and the molecular mechanisms associated with their stress-protective activity. Pharmaceuticals (Basel). — PubMed: Panossian mechanisms
- Cropley M et al. (2015). The effects of Rhodiola rosea L. extract on anxiety, stress, cognition and other mood symptoms. Phytotherapy Research. — PubMed: Cropley rhodiola
- Bystritsky A et al. (2008). A pilot study of Rhodiola rosea for generalized anxiety disorder. Journal of Alternative and Complementary Medicine. — PubMed: Bystritsky GAD pilot
- Saxena RC et al. (2012). Efficacy of an Extract of Ocimum tenuiflorum (OciBest) in the Management of General Stress. Evidence-Based Complementary and Alternative Medicine. — PubMed: Saxena holy basil
- Cohen MM (2014). Tulsi - Ocimum sanctum: A herb for all reasons. Journal of Ayurveda and Integrative Medicine. — PubMed: Cohen tulsi review
- Kennedy DO et al. (2003). Anxiolytic effects of a combination of Melissa officinalis and Valeriana officinalis during laboratory induced stress. Phytotherapy Research. — PubMed: Kennedy lemon balm
- Speers AB et al. (2021). Effects of Withania somnifera (ashwagandha) on stress and the stress-related neuropsychiatric disorders. Current Neuropharmacology. — PubMed: Speers comprehensive review
Research Papers: Breath & Cold Exposure
- Zaccaro A et al. (2018). How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Frontiers in Human Neuroscience. — PubMed: Zaccaro systematic review
- Balban MY et al. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine. — PubMed: Balban cyclic sighing
- Lehrer PM, Gevirtz R (2014). Heart rate variability biofeedback: how and why does it work? Frontiers in Psychology. — PubMed: Lehrer HRV biofeedback
- Russo MA et al. (2017). The physiological effects of slow breathing in the healthy human. Breathe. — PubMed: Russo slow breathing
- Kox M et al. (2014). Voluntary activation of the sympathetic nervous system and attenuation of the innate immune response in humans. PNAS. — PubMed: Kox Wim Hof PNAS
- Buijze GA et al. (2016). The effect of cold showering on health and work: a randomized controlled trial. PLoS ONE. — PubMed: Buijze cold shower RCT
- Srámek P et al. (2000). Human physiological responses to immersion into water of different temperatures. European Journal of Applied Physiology. — PubMed: Sramek cold immersion catecholamines
- Brown RP, Gerbarg PL (2005). Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression. Journal of Alternative and Complementary Medicine. — PubMed: Brown Sudarshan Kriya
- Bordoni B et al. (2018). The influence of breathing on the central nervous system. Cureus. — PubMed: Bordoni breathing CNS
- Tipton MJ et al. (2017). Cold water immersion: kill or cure? Experimental Physiology. — PubMed: Tipton cold water risks
Research Papers: Cross-Cutting (HPA Axis, GABA, Vagal Tone)
- Bandelow B et al. (2017). Treatment of anxiety disorders. Dialogues in Clinical Neuroscience. — PubMed: Bandelow treatment overview
- Lydiard RB (2003). The role of GABA in anxiety disorders. Journal of Clinical Psychiatry. — PubMed: Lydiard GABA
- Stein DJ et al. (2017). Generalized anxiety disorder. NEJM. — PubMed: Stein NEJM GAD
- Heim C, Nemeroff CB (2001). The role of childhood trauma in the neurobiology of mood and anxiety disorders. Biological Psychiatry. — PubMed: Heim early adversity
- Porges SW (2007). The polyvagal perspective. Biological Psychology. — PubMed: Porges polyvagal theory
- Sarris J et al. (2013). Lifestyle medicine for depression. BMC Psychiatry. — PubMed: Sarris lifestyle medicine
- Chaudhary R et al. (2019). Inflammation and anxiety. Journal of Neuroinflammation. — PubMed: Inflammation and anxiety
- Carpenter LL et al. (2007). Vagus nerve stimulation: a new tool for brain research and therapy. Biological Psychiatry. — PubMed: VNS biological psychiatry
- Foster JA, McVey Neufeld KA (2013). Gut-brain axis: how the microbiome influences anxiety and depression. Trends in Neurosciences. — PubMed: Foster gut-brain axis
- Ravindran AV et al. (2016). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 5. Complementary and alternative medicine treatments. Canadian Journal of Psychiatry. — PubMed: CANMAT CAM guidelines
External Authoritative Resources
- NIH National Center for Complementary and Integrative Health — Anxiety at a Glance
- NIH Office of Dietary Supplements — Magnesium Fact Sheet (Health Professionals)
- Linus Pauling Institute — Magnesium Micronutrient Information Center
- NCBI Bookshelf — Ashwagandha (Withania somnifera) (LiverTox monograph)
- PubMed — All research on natural anxiety treatment supplements
Connections
- Natural Anxiety Relief (Main Page)
- L-Theanine and Green Tea
- Magnesium Glycinate
- Adaptogenic Herbs
- Breath and Cold Exposure
- All Remedies
- Magnesium
- L-Theanine
- Ashwagandha
- Rhodiola Rosea
- Holy Basil (Tulsi)
- Lemon Balm
- Psychiatric Conditions
- Stress Management
- Sleep Hygiene