Breath and Cold Exposure for Anxiety
Breath and cold are the two interventions the body uses to talk directly to the autonomic nervous system without a supplement, a pharmaceutical, or a herb in between. Slow nasal breathing at 4–6 breaths per minute, with the exhale longer than the inhale, raises vagal tone and reduces sympathetic outflow within minutes — the mechanism Lehrer and Gevirtz characterized as "resonance frequency breathing" that synchronizes the baroreflex feedback loop. Cold exposure (cold shower, cold plunge, face immersion in ice water) triggers the mammalian dive reflex and produces a sustained 250% dopamine elevation and 530% norepinephrine elevation that persists for hours after the cold stimulus has ended — documented in the Srámek 2000 catecholamine study and replicated since. The combination of breath work and cold exposure is the body-based half of the natural anxiety relief toolkit, with the unique advantage that it is free, available immediately, and works through measurable autonomic mechanisms rather than slow biochemical shifts.
Table of Contents
- The Autonomic Nervous System and Anxiety
- The Vagus Nerve and Polyvagal Theory
- Slow Nasal Breathing: The 6-Breaths-Per-Minute Sweet Spot
- Specific Breathing Techniques (Box, Physiological Sigh, 4-7-8, Wim Hof)
- Cold Exposure: Dive Reflex, Dopamine, and Norepinephrine
- Cold Exposure Protocols (Shower, Plunge, Face Immersion)
- Combining Breath and Cold (Wim Hof Method)
- Clinical Evidence for Anxiety
- Building a Daily Practice
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
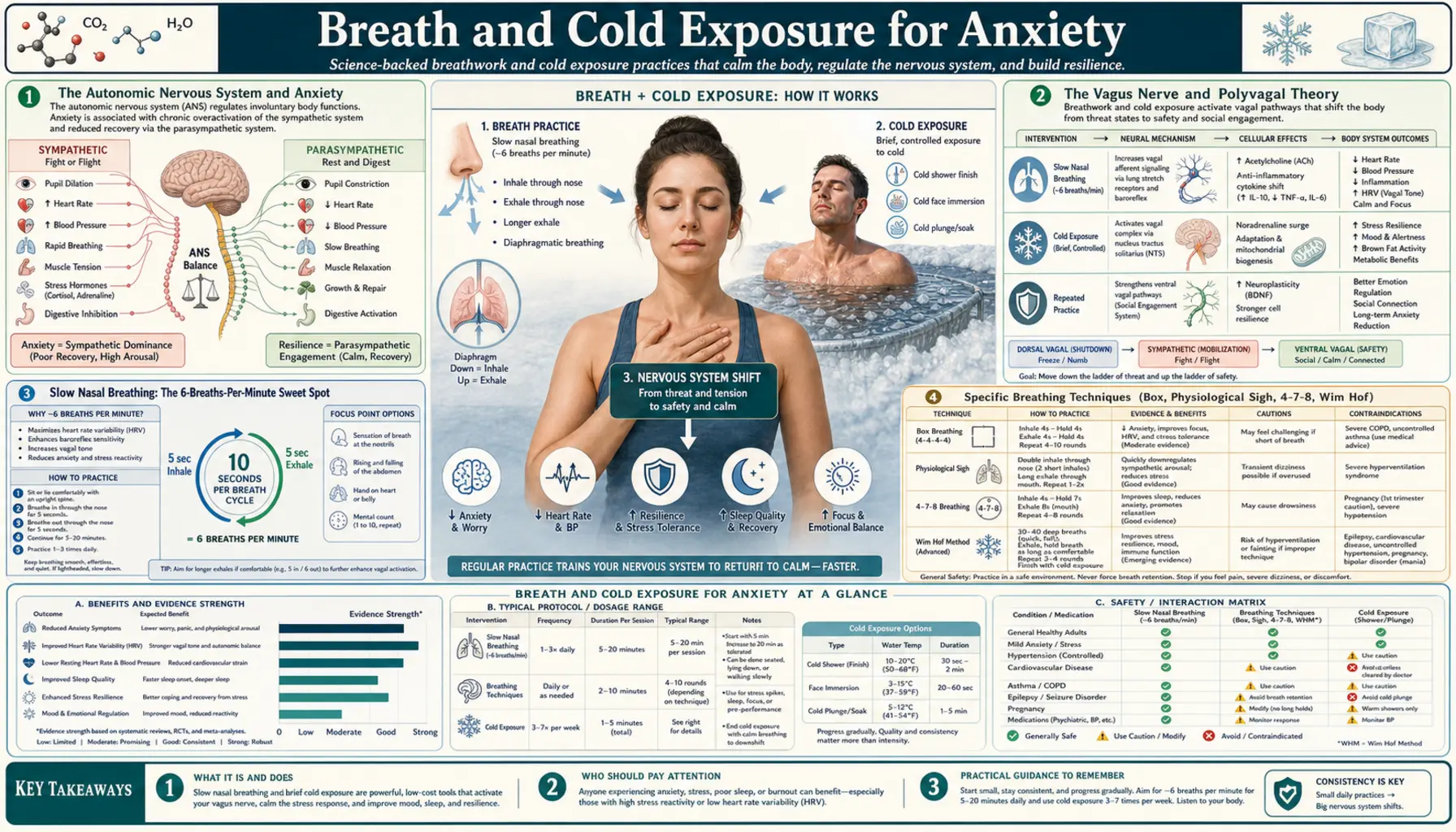
The Autonomic Nervous System and Anxiety
The autonomic nervous system has two branches that operate in dynamic balance:
- Sympathetic nervous system — the "fight or flight" branch. Releases norepinephrine at end organs. Increases heart rate, blood pressure, respiratory rate, pupil diameter, sweat production, blood glucose, and skeletal muscle perfusion. Diverts blood away from the gut and reproductive organs. Triggered acutely by threat detection in the amygdala and by chronic activation in clinical anxiety.
- Parasympathetic nervous system — the "rest and digest" branch. Acts primarily through the vagus nerve, releasing acetylcholine at end organs. Slows heart rate, lowers blood pressure, slows respiration, dilates the gut and reproductive vasculature, and promotes digestion, repair, and recovery.
In anxiety disorders, this balance is chronically tipped toward sympathetic dominance. Heart rate variability (HRV) — the beat-to-beat variation in heart rate that reflects vagal tone — is reduced in anxiety, depression, PTSD, and chronic stress. The lower the HRV, the more dominant the sympathetic branch and the higher the subjective sense of being "wired," restless, or unable to settle. Restoring vagal tone is therefore a measurable, mechanistic anxiety intervention.
The unique value of breath and cold as anxiety interventions is that they directly drive the autonomic balance without any pharmacologic intermediary. Breath does so via the vagus nerve's direct innervation of respiratory rhythm generators in the brainstem. Cold does so via afferent trigeminal and vagal signaling from cold-receptor activation. Both produce effects within minutes that can be felt subjectively and measured objectively.
The Vagus Nerve and Polyvagal Theory
The vagus nerve is cranial nerve X, the longest cranial nerve in the body. It is named from the Latin vagus meaning "wandering" — it wanders from the brainstem down through the neck and chest to innervate the heart, lungs, larynx, pharynx, esophagus, stomach, small intestine, proximal colon, liver, pancreas, and spleen. Approximately 80% of vagal fibers are afferent (sensory, carrying information from organs back to the brain); only 20% are efferent (motor, carrying instructions from the brain to organs).
Stephen Porges's polyvagal theory (formally proposed 1994, refined in subsequent work) divides vagal function into two distinct branches with different evolutionary origins:
- The ventral vagal complex — the more recent, myelinated, mammalian branch. Originates in the nucleus ambiguus. Mediates social engagement, vocal prosody, facial expression, and the "calm and connected" state of safe social interaction. Activated by warm social contact, by slow exhale-dominant breathing, and by the "freeze-thaw" of recovery from cold exposure.
- The dorsal vagal complex — the older, unmyelinated, reptilian branch. Originates in the dorsal motor nucleus. Mediates the "freeze" or "shutdown" response when the system is overwhelmed by threat — the parasympathetic equivalent of being "frozen with fear" rather than calmly engaged.
The therapeutic implication is that simply "activating the parasympathetic system" is not sufficient or even desirable — the goal of anxiety intervention is specifically to activate the ventral vagal complex (calm and engaged) while de-escalating both sympathetic over-arousal and the freeze response. Slow nasal breathing with extended exhale is the most direct lever for ventral vagal activation. Cold face immersion specifically (the "mammalian dive reflex") is also primarily a ventral vagal stimulus.
Polyvagal theory has critics in academic neuroscience — the strict ventral-vs-dorsal anatomical distinction is more fluid than Porges's clinical framework implies. But the practical observation that slow breathing and cold exposure produce calm-and-engaged states (rather than sedation or shutdown) is robust and well-replicated.
Slow Nasal Breathing: The 6-Breaths-Per-Minute Sweet Spot
Normal resting respiratory rate in adults is approximately 12–20 breaths per minute. In anxiety, it commonly rises to 18–25 breaths per minute, often with shallow chest expansion and occasional sighing. Deliberately slowing the breath to 6 breaths per minute (5-second inhale, 5-second exhale) produces a striking acute physiological effect that has been replicated in multiple labs:
- Heart rate variability increases — specifically the high-frequency (HF) component that reflects parasympathetic tone
- Baroreflex sensitivity increases — the responsiveness of the cardiovascular feedback loop that maintains blood pressure homeostasis
- Systolic blood pressure decreases by 5–10 mmHg in most subjects
- Subjective anxiety scores decrease within 5–10 minutes of starting the practice
- EEG alpha-wave power increases — the same alpha-shift that L-theanine produces, here via autonomic feedback to cortex
The reason 6 breaths per minute specifically is the sweet spot is mechanistic. The baroreflex feedback loop — the system that detects blood pressure fluctuations and adjusts heart rate to compensate — has a characteristic resonance frequency of approximately 0.1 Hz, which corresponds to 6 cycles per minute. When breathing matches this frequency, the natural oscillation of heart rate (faster on inhale, slower on exhale) entrains with the baroreflex loop, producing maximum HRV amplitude and maximum vagal activation. Lehrer's heart rate variability biofeedback (HRVB) protocol uses this resonance-frequency breathing as the core training stimulus.
For practical anxiety relief, the basic protocol is:
- Sit upright (not slouched) or stand. Posture matters because diaphragmatic expansion is restricted in a slouched position.
- Breathe through the nose only (mouth closed). Nasal breathing produces nitric oxide release that improves pulmonary perfusion, slows respiration naturally, and engages diaphragmatic rather than chest expansion.
- Inhale slowly for 4–5 seconds, expanding the belly rather than the chest. The diaphragm should descend visibly.
- Exhale slowly for 6–7 seconds, slightly longer than the inhale. The longer exhale preferentially activates the parasympathetic branch.
- Do not hold the breath at top or bottom (basic practice). The pause is optional and not needed for the anxiety effect.
- Continue for 5–10 minutes. The acute anxiolytic effect is usually obvious by minute 3–5.
The hard part is doing this when actually anxious. In acute anxiety, the chest is tight, the respiratory rate is elevated, and the urge is to gasp or hyperventilate. Slowing the breath against that drive feels unnatural and produces transient air hunger. Practicing daily when calm (5–10 minutes before bed, on waking, or as a midday reset) builds the muscle memory and confidence to deploy the practice in acute anxiety.
Specific Breathing Techniques (Box, Physiological Sigh, 4-7-8, Wim Hof)
- Box breathing (4-4-4-4) — used by US Navy SEALs and special forces for combat anxiety control. Inhale 4, hold 4, exhale 4, hold 4. Repeat for 5 minutes. Produces a measured calm without the drowsiness of longer-exhale techniques. Best for situations where alert performance is needed (presentations, interviews, surgery).
- Physiological sigh — the body's built-in stress-relief breath, characterized recently by Andrew Huberman's Stanford lab and Mark Krasnow's lab. Two quick nasal inhales (the second one stacks on top of the first) followed by one long mouth exhale. Re-inflates collapsed alveoli, off-loads accumulated CO2, and produces an acute drop in subjective anxiety. The Balban 2023 Cell Reports Medicine trial showed cyclic sighing (5 minutes daily) produced greater anxiety reduction than mindfulness meditation in healthy adults. Useful as an in-the-moment reset — 2–3 cycles produce a noticeable shift.
- 4-7-8 breathing — popularized by integrative physician Andrew Weil. Inhale 4, hold 7, exhale 8. Repeat 4 cycles. The prolonged breath hold and long exhale produce strong parasympathetic activation. Best for sleep onset — many users fall asleep within minutes of completing one round in bed.
- Wim Hof breathing — named for the Dutch extreme-cold athlete. Cycles of 30–40 deep rapid breaths (hyperventilation, alkalinizing blood) followed by a prolonged exhale-and-hold. Produces a profound altered state and acute reduction in inflammatory markers (Kox 2014 PNAS). Not strictly anxiolytic — the hyperventilation phase can trigger anxiety in susceptible individuals. Best paired with cold exposure (see below).
- Sudarshan Kriya yogic breathing (SKY) — multi-phase yogic technique combining slow, medium, and fast rhythmic breathing. Brown and Gerbarg 2005 found significant benefit in depression and anxiety. Requires instruction (typically a course offered by the Art of Living Foundation) and 30–45 minutes per session. Higher commitment than other techniques but with stronger evidence in clinical populations.
- Alternate nostril breathing (Nadi Shodhana) — pranayama technique from yoga. Close right nostril with thumb, inhale through left; close left nostril, exhale through right; inhale through right; close right, exhale through left. The forced nasal-only breathing and rhythmic alternation produce parasympathetic activation. Useful as a brief reset practice (3–5 minutes).
For most anxiety patients, starting with 5 minutes of basic slow nasal breathing (5-second inhale, 5-second exhale) daily is sufficient. Add box breathing for acute situations, physiological sigh for in-the-moment resets, and 4-7-8 for sleep onset.
Cold Exposure: Dive Reflex, Dopamine, and Norepinephrine
Deliberate cold exposure — cold shower, cold plunge, cold face immersion, ice bath — produces an acute and surprisingly sustained shift in neurochemistry and autonomic tone. The Srámek 2000 European Journal of Applied Physiology study, the foundational catecholamine paper, immersed healthy volunteers in 14°C water for one hour and measured plasma neurochemistry. Results:
- Norepinephrine increased by approximately 530% from baseline
- Dopamine increased by approximately 250% from baseline
- Elevations persisted for hours after the cold exposure ended
- No significant elevation in cortisol — the cold response is catecholamine-dominant, not glucocorticoid-dominant
The norepinephrine surge is initially counterintuitive for an anxiety intervention — norepinephrine is the same neurotransmitter responsible for the sympathetic arousal in panic attacks. The difference is the context: cold-induced norepinephrine release happens against a backdrop of voluntary, controlled exposure to a non-threatening stressor, with a parasympathetic rebound that follows. The result is a "primed but calm" state, with elevated mood, sharper cognition, and reduced baseline anxiety for hours afterward.
The dopamine elevation is the more durable mood effect. Unlike norepinephrine, which is rapidly cleared, dopamine's elevated baseline persists for 4–6 hours after a single cold exposure, producing the well-known "high" or "afterglow" reported by cold plungers. This is not a placebo effect — the dopamine elevation has been documented in catecholamine assays and is consistent across studies.
The autonomic mechanism involves the mammalian dive reflex: cold receptors on the face and forehead, mediated by the trigeminal nerve, trigger an automatic parasympathetic response that slows heart rate, constricts peripheral blood vessels, and redirects blood to the brain and heart. The reflex is preserved across mammals and is most powerfully triggered by cold water on the upper face, particularly the area between and around the eyes. Even a simple practice of submerging the face in cold water for 30 seconds activates this reflex and can abort an acute panic episode in some individuals.
Cold Exposure Protocols (Shower, Plunge, Face Immersion)
| Protocol | Temperature | Duration | Best Use |
|---|---|---|---|
| Face immersion (bowl of ice water) | 10–15°C (50–60°F) | 30 seconds, 3 reps | Acute panic abort, in-the-moment anxiety reset |
| Cold shower (end of hot shower) | As cold as tap delivers, typically 15–20°C | 30 sec → 1 min → 2 min over weeks | Daily practice, lowest barrier to entry |
| Cold plunge / ice bath | 10–15°C (50–59°F) | 2–5 minutes | 2–3x/week deliberate stress training |
| Outdoor cold water swim | 5–15°C (varies by season) | 5–15 minutes | Community / social practice, mood booster |
For most patients starting out, the "end of shower" cold finish is the lowest-barrier entry: end a normal hot shower by turning the temperature as cold as the tap delivers, for 30 seconds initially, working up to 2 minutes over several weeks. This requires no equipment, no time commitment beyond the shower already happening, and produces meaningful catecholamine and mood effects within 2–3 weeks of daily practice.
For acute anxiety abort — an unfolding panic attack, a wave of overwhelming anxiety — the face immersion technique is fastest. Fill a large bowl with cold tap water plus 4–6 ice cubes. Submerge the entire face (forehead through chin) for 30 seconds while holding the breath. The mammalian dive reflex activates within 5–10 seconds. Repeat 2–3 times. This is the technique recommended in DBT (dialectical behavior therapy) as a TIP (Temperature, Intense exercise, Paced breathing) distress tolerance skill.
For the more committed practitioner, a cold plunge tub or a converted chest freezer (the popular DIY approach) allows full-body immersion at 10–15°C. The Andrew Huberman framework recommends approximately 11 minutes of total cold exposure per week, distributed across 2–4 sessions, as the dose that delivers the durable mood, metabolic, and resilience benefits without producing excessive sympathetic burden.
Combining Breath and Cold (Wim Hof Method)
The Dutch extreme-cold athlete Wim Hof formalized a protocol that combines structured hyperventilation breathing with deliberate cold exposure. The Wim Hof Method has three pillars: breathing technique, gradual cold exposure, and committed mindset. The 2014 PNAS paper by Kox and colleagues at Radboud University documented that trained Wim Hof practitioners can voluntarily attenuate the innate immune response to bacterial endotoxin — a striking finding that demonstrates the autonomic nervous system can be deliberately influenced beyond what was previously thought possible.
The basic Wim Hof breathing protocol:
- Sit or lie comfortably
- 30–40 deep cycles of full inhale and passive exhale (hyperventilation phase)
- At the end of the 30th–40th cycle, fully exhale and hold the breath at empty (retention)
- Hold as long as comfortable (typically 60–120 seconds for beginners, much longer with practice)
- Take a full recovery inhale and hold at top for 15 seconds
- Repeat the cycle 3–4 times total
This is followed by cold exposure (cold shower, plunge, or ice bath). The combination produces a distinctive subjective experience — calm euphoria, sharp mental clarity, and elevated mood that persists for hours.
The method is not for everyone with anxiety. The hyperventilation phase can trigger panic in susceptible individuals, particularly those with a history of panic disorder. It should NEVER be performed in water (drowning risk from the breath-hold) or while driving. Start with the breathing alone, in a safe seated position, before combining with cold exposure. If the hyperventilation provokes anxiety rather than calm, switch to box breathing or slow nasal breathing instead.
Clinical Evidence for Anxiety
The clinical evidence for breath and cold as anxiety interventions has grown substantially in the last decade. Key trials:
- Zaccaro 2018 (Frontiers in Human Neuroscience) — systematic review of slow breathing interventions across psychophysiology. Consistent positive findings on HRV, vagal tone, and subjective anxiety across 15 studies.
- Balban 2023 (Cell Reports Medicine) — landmark Stanford trial comparing 5 minutes daily of cyclic sighing vs box breathing vs cyclic hyperventilation vs mindfulness meditation in 108 healthy adults over 28 days. Cyclic sighing produced the largest improvement in mood and reduction in respiratory rate. All breath-work groups outperformed mindfulness meditation on these outcomes.
- Lehrer / Gevirtz 2014 (Frontiers in Psychology) — review of HRV biofeedback for anxiety, depression, asthma, IBS, and PTSD. Resonance frequency breathing (~6 bpm) is the most-studied intervention; consistent positive findings across conditions.
- Brown and Gerbarg 2005 (Journal of Alternative and Complementary Medicine) — Sudarshan Kriya yogic breathing for depression and anxiety. Significant benefit in clinical populations.
- Buijze 2016 (PLoS ONE) — randomized controlled trial of daily 30–90 second cold shower finish in 3,018 Dutch adults over 30 days. 29% reduction in workplace absenteeism in the cold-shower group vs control. Self-rated quality of life and energy improved.
- Kox 2014 (PNAS) — Wim Hof Method training (breathing + cold + meditation) reduced inflammatory response to bacterial endotoxin in 12 trained vs 12 untrained subjects. The first rigorous demonstration that voluntary autonomic modulation can influence the innate immune response.
- van Tulleken 2018 (BMJ Case Reports) — case report of weekly open-water cold swimming as treatment for treatment-resistant major depressive disorder in a 24-year-old woman. Sustained remission of symptoms with gradual discontinuation of fluoxetine. Anecdotal but suggests cold exposure may be a meaningful intervention even in serious mood disorders.
- Yankouskaya 2023 (Biology) — functional MRI study of cold-water immersion. 5-minute immersion produced reduced functional connectivity in default-mode-network regions associated with rumination, and increased connectivity in attention-control networks — consistent with the subjective "clear-headed" effect.
The combined evidence base supports breath and cold as legitimate, mechanistically-grounded interventions for anxiety. Effect sizes are small-to-moderate, but the interventions are free, available immediately, and produce acute effects measurable in minutes rather than weeks.
Building a Daily Practice
For most patients, building a sustainable daily practice matters more than any specific technique. A workable starter protocol:
- Morning, on waking — 5 minutes of slow nasal breathing at 6 breaths per minute. Sit upright in bed or in a chair. Set a timer.
- End of morning shower — finish with 30 seconds of cold water, working up to 1–2 minutes over weeks.
- Midday — 1–2 physiological sighs as a reset between work blocks (takes 10 seconds, no equipment needed).
- Acute anxiety — box breathing (4-4-4-4) for 2–3 minutes, or face immersion in cold water if breathing alone is not enough.
- Sleep onset — 4-7-8 breathing in bed, 4 cycles, then transition to normal relaxed breath.
For the more committed practitioner, adding a weekly cold plunge (2–5 minutes at 10–15°C, 2–3 sessions per week) and a longer (15–20 minute) breathwork practice once or twice per week deepens the autonomic recalibration. The Wim Hof Method is one option for the structured longer practice; Sudarshan Kriya is another with stronger clinical-trial evidence.
The hardest part is consistency. Anxiety patients in particular tend to abandon practices that don't produce immediate dramatic relief. The first 2–3 weeks of daily breath and cold practice often produce modest benefit; the cumulative effect over 8–12 weeks is substantially larger as the autonomic baseline shifts. Tracking subjective anxiety on a 0–10 scale daily, with a weekly average, provides the longitudinal feedback that maintains motivation through the early plateau.
Cautions and Contraindications
Cold exposure cautions:
- Cardiovascular disease — cold exposure produces an acute pressor response (blood pressure spike) and increases cardiac afterload. Patients with uncontrolled hypertension, coronary disease, recent myocardial infarction, arrhythmias (particularly atrial fibrillation), or significant heart failure should not undertake cold plunge or full-body cold exposure without cardiologist clearance. Face immersion alone is generally tolerated.
- Raynaud's phenomenon — cold can trigger painful vasospasm. Avoid full-body cold; brief face immersion may be tolerated.
- Pregnancy — conservative practice is to avoid full-body cold immersion during pregnancy, particularly in the third trimester. Brief cool showers are acceptable.
- Cold urticaria — rare condition in which cold exposure provokes urticarial wheals or even anaphylaxis. Contraindication.
- Cold shock and drowning risk — uncontrolled cold water immersion can produce involuntary gasping, hyperventilation, and drowning. Always have a safe exit, never immerse alone in deep water as a beginner, and never combine breath-hold practices (Wim Hof) with water immersion without supervision.
- Hypothermia risk — the Tipton 2017 review ("Cold water immersion: kill or cure?") details the genuine risks of prolonged cold immersion. Follow established time limits and warm gradually after exposure.
Breathwork cautions:
- Pregnancy — avoid breath retention (the hold phases of Wim Hof, 4-7-8, and box breathing) during pregnancy. Slow nasal breathing is fine.
- Epilepsy / seizure disorder — the Wim Hof hyperventilation phase can lower the seizure threshold. Stick to slow breathing.
- Severe COPD or asthma — modify any breath-hold techniques. Slow nasal breathing is fine and often beneficial.
- Panic disorder with respiratory subtype — some panic patients are highly sensitive to breath sensations and can trigger panic by focusing on respiration. Start with very brief practices (1–2 minutes) and a supportive setting.
- Cardiovascular disease — the breath-hold phases of Wim Hof and 4-7-8 produce transient pressure shifts. Slow nasal breathing is generally beneficial; breath-hold techniques warrant cardiologist input in established cardiac disease.
- Never perform breath-hold techniques in water — drowning risk from breath-hold-induced loss of consciousness.
- Never perform breath-hold techniques while driving or operating machinery.
For the great majority of anxiety patients without cardiovascular contraindications, breath and cold are among the lowest-risk, highest-yield anxiety interventions available, with mechanistic backing and growing clinical evidence base. They are most powerful when integrated into daily life as small consistent practices rather than treated as occasional "treatments."
Key Research Papers
- Zaccaro A, Piarulli A, Laurino M et al. (2018). How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Frontiers in Human Neuroscience. — PMID: 30245619
- Balban MY, Neri E, Kogon MM et al. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Reports Medicine. — PMID: 36630953
- Lehrer PM, Gevirtz R (2014). Heart rate variability biofeedback: how and why does it work? Frontiers in Psychology. — PMID: 25101026
- Russo MA, Santarelli DM, O'Rourke D (2017). The physiological effects of slow breathing in the healthy human. Breathe. — PMID: 29209423
- Kox M, van Eijk LT, Zwaag J et al. (2014). Voluntary activation of the sympathetic nervous system and attenuation of the innate immune response in humans. PNAS. — PMID: 24799686
- Buijze GA, Sierevelt IN, van der Heijden BC et al. (2016). The effect of cold showering on health and work: a randomized controlled trial. PLoS ONE. — PMID: 27631616
- Srámek P, Simecková M, Janský L et al. (2000). Human physiological responses to immersion into water of different temperatures. European Journal of Applied Physiology. — PMID: 10751106
- Brown RP, Gerbarg PL (2005). Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression: part II. Clinical applications and guidelines. Journal of Alternative and Complementary Medicine. — PMID: 16131297
- Porges SW (2007). The polyvagal perspective. Biological Psychology. — PMID: 17049418
- Tipton MJ, Collier N, Massey H et al. (2017). Cold water immersion: kill or cure? Experimental Physiology. — PMID: 28833689
- van Tulleken C, Tipton M, Massey H, Harper CM (2018). Open water swimming as a treatment for major depressive disorder. BMJ Case Reports. — PMID: 30131418
- Bordoni B, Purgol S, Bizzarri A et al. (2018). The influence of breathing on the central nervous system. Cureus. — Search PubMed
- Yankouskaya A, Williamson R, Stacey C et al. (2023). Short-term head-out whole-body cold-water immersion facilitates positive affect and increases interaction between large-scale brain networks. Biology. — Search PubMed
PubMed Topic Searches
- PubMed: Slow breathing / vagal tone
- PubMed: HRV biofeedback / anxiety
- PubMed: Cold water immersion / mood
- PubMed: Wim Hof Method
- PubMed: Polyvagal theory / vagus
Connections
- Natural Anxiety Relief Hub
- Natural Anxiety Relief Benefits
- L-Theanine and Green Tea
- Magnesium Glycinate
- Adaptogenic Herbs
- Stress Management
- Sleep Hygiene
- Cold Exposure
- Breathing Techniques
- Meditation
- Exercise
- Hypertension
- Psychiatric Conditions
- Heart Rate Variability
- All Remedies