Adaptogenic Herbs for Anxiety
"Adaptogen" is the term coined in 1947 by Soviet pharmacologist Nikolai Lazarev to describe a category of botanical agents that increase nonspecific resistance to physical, chemical, biological, and psychological stress while normalizing physiology in either direction (calming an over-aroused state, energizing an exhausted state). The modern definition refined by Panossian requires three criteria: nontoxic at normal doses, broad nonspecific stress resistance, and a normalizing rather than direction-specific effect. Of the dozens of herbs marketed as adaptogens, four have the strongest published clinical evidence for anxiety reduction: ashwagandha (the most-studied, nine-plus RCTs), rhodiola rosea (Soviet-military fatigue-and-anxiety adaptogen), holy basil / tulsi (Ayurvedic everyday adaptogen), and lemon balm (gentler GABAergic herb sometimes classified as a nervine rather than a true adaptogen). This page covers mechanism, evidence, dosing, and the cautions that matter for each.
Table of Contents
- What "Adaptogen" Actually Means
- Shared Mechanism: HPA Axis, Hsp70, Nrf2
- Ashwagandha (Withania somnifera)
- Rhodiola Rosea
- Holy Basil (Tulsi, Ocimum sanctum)
- Lemon Balm (Melissa officinalis)
- Other Adaptogens Worth Knowing
- How to Choose Which Adaptogen
- Stacking and Sequencing
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
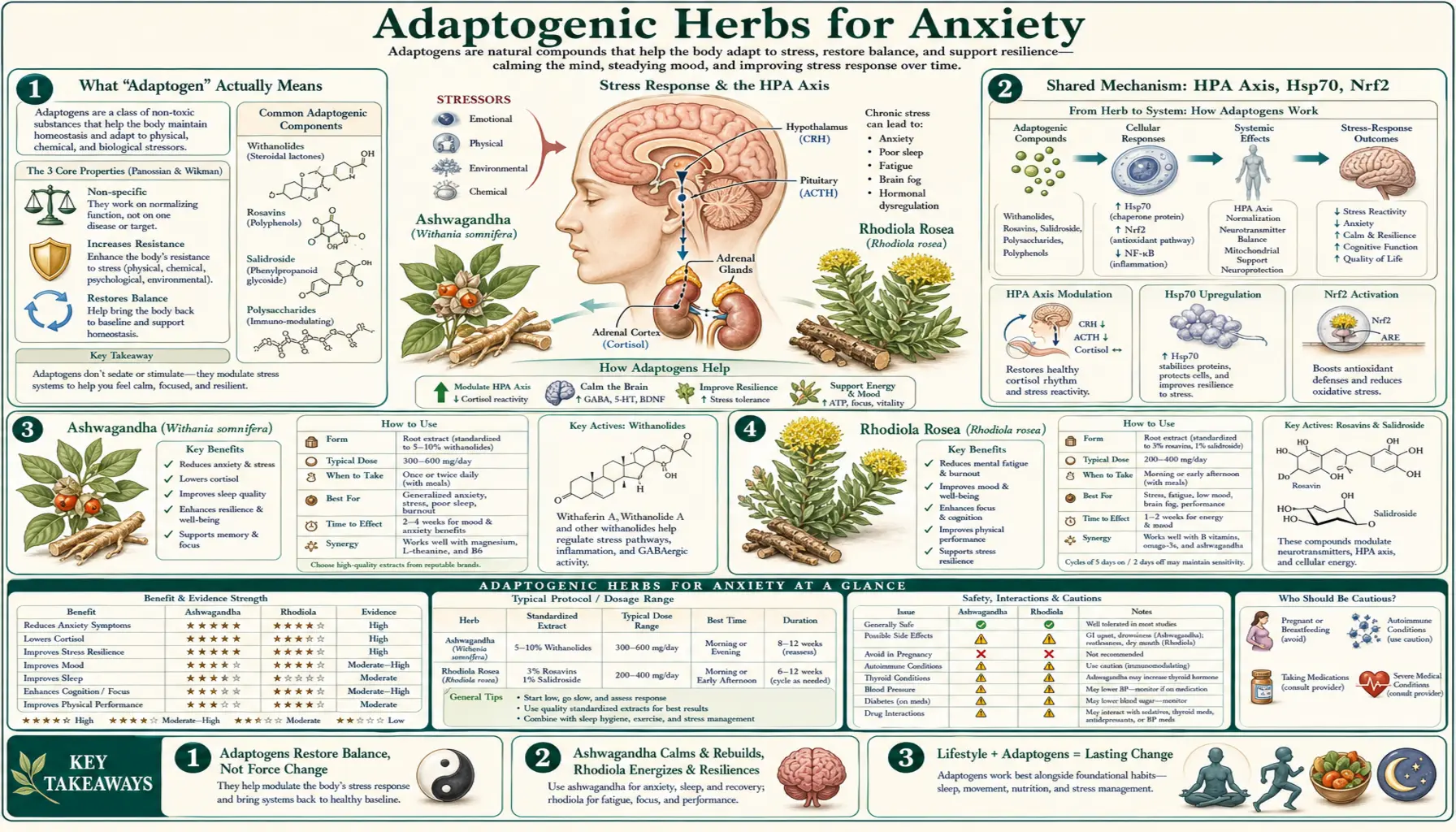
What "Adaptogen" Actually Means
Nikolai Lazarev coined the term adaptogen in 1947 to describe substances that increase the body's "nonspecific resistance" to stressors of all kinds — physical (cold, heat, exertion, hypoxia), chemical (toxins, radiation), biological (infection), and psychological (anxiety, depression, performance demand). Lazarev's student Israel Brekhman refined the concept in the 1960s and led the Soviet research program that screened hundreds of botanicals for adaptogenic activity, ultimately identifying Eleutherococcus senticosus, Rhodiola rosea, and Schisandra chinensis as the three core "Soviet adaptogens" used to support cosmonauts, Olympic athletes, and military personnel.
The modern criteria, formalized by Alexander Panossian in a series of pharmaceutical reviews from 2010 onward, require three properties:
- Nontoxic at normal therapeutic doses — the substance should be safe enough for daily long-term use by healthy individuals.
- Broad nonspecific stress resistance — effects on multiple stressor types, not narrow pharmacology directed at a single receptor or pathway.
- Normalizing effect — the substance should restore homeostasis rather than push physiology in a fixed direction. An adaptogen should calm an over-aroused state and energize an exhausted state, depending on what the body needs.
The category includes both calming adaptogens (ashwagandha, holy basil, schisandra) and stimulating adaptogens (rhodiola, eleuthero, panax ginseng, cordyceps). For anxiety, the calming end of the spectrum is generally more useful, though rhodiola is unusual in being stimulating and anxiolytic at the same time (it reduces fatigue while reducing anxiety in the same dose, a profile particularly well-suited to burnout).
Shared Mechanism: HPA Axis, Hsp70, Nrf2
Adaptogens converge on several shared molecular mechanisms that distinguish them from agents that act at a single receptor:
- HPA axis dampening — the most reproducible finding is reduction in elevated cortisol with normalization of the diurnal cortisol rhythm. Multiple ashwagandha trials show 20–45% reduction in morning serum cortisol after 8–12 weeks of supplementation in stressed adults. Holy basil and rhodiola show similar but smaller effects.
- Heat shock protein 70 (Hsp70) induction — Hsp70 is a molecular chaperone protein that protects cellular protein structure under stress and helps return the cell to homeostasis after the stress passes. Adaptogens upregulate Hsp70 expression in cell-culture and animal-model experiments, a mechanism Panossian has emphasized as a unifying feature of the category.
- Nrf2 antioxidant response element activation — Nrf2 is a transcription factor that activates the body's endogenous antioxidant defenses (glutathione, superoxide dismutase, catalase, NQO1). Several adaptogens, including ashwagandha and rhodiola, activate Nrf2 and increase intracellular glutathione, providing oxidative stress resilience that translates to broader stress tolerance.
- Neurotransmitter modulation — specific adaptogens hit specific neurotransmitter systems. Ashwagandha has direct GABAergic activity at GABA-A and GABA-B receptors. Rhodiola modulates serotonin, dopamine, and norepinephrine. Holy basil has anti-inflammatory effects via NF-kB pathway inhibition. Lemon balm acts at GABA receptors and inhibits GABA transaminase (the enzyme that degrades GABA).
- BDNF (brain-derived neurotrophic factor) induction — ashwagandha and rhodiola both increase hippocampal BDNF in animal models, a mechanism shared with SSRIs and exercise. BDNF supports neuroplasticity and is reduced in depression and chronic anxiety.
The convergence is biochemically meaningful but clinically diverse — different adaptogens produce different subjective phenotypes despite overlapping mechanisms. Choosing the right adaptogen for a given patient is more art than algorithm, but the descriptions below offer a starting framework.
Ashwagandha (Withania somnifera)
Ashwagandha is the most-studied of all adaptogens for anxiety, with at least nine published randomized controlled trials specifically in anxious or stressed populations. The Indian root (Withania somnifera, family Solanaceae) has been used in Ayurvedic medicine for at least 3,000 years as a rasayana (rejuvenative) for stress, sleep, vigor, and convalescence. The Sanskrit name translates roughly as "smell of horse" — the root has a distinctive earthy odor and the traditional claim was that it imparted the strength of a horse.
Active compounds: the bioactive fraction is composed of withanolides (steroidal lactones), with withaferin A and withanolide A as the most-studied. Standardized extracts are quantified by withanolide percentage:
- KSM-66 (Ixoreal Biomed) — the most-studied commercial extract; root-only, 5% withanolides by HPLC. Used in the majority of recent RCTs.
- Sensoril (Natreon) — root and leaf extract, ≥10% withanolides. Higher potency per gram, but the leaf inclusion raises some traditionalist concerns about a different chemical profile.
- Shoden (Arjuna Natural) — root and leaf extract, 35% withanolides. Even higher potency; used in some newer trials at 240 mg/day.
Clinical evidence for anxiety:
- Chandrasekhar 2012 (Indian Journal of Psychological Medicine) — the landmark trial. 64 adults with chronic stress randomized to 300 mg KSM-66 twice daily vs placebo for 60 days. Results: 44% reduction in Perceived Stress Scale (vs 5.5% placebo), 27.9% reduction in serum cortisol (vs slight increase in placebo), significant improvement on every secondary anxiety measure.
- Lopresti 2019 (Medicine Baltimore) — 60 adults randomized to KSM-66 240 mg/day vs placebo for 60 days. Significant reduction in morning cortisol and Hamilton Anxiety Rating Scale; reduction in DHEA-S in the ashwagandha group.
- Salve 2019 (Cureus) — 60 healthy adults (no anxiety diagnosis), 250–600 mg KSM-66 daily for 60 days. Dose-dependent reduction in stress and improvement in sleep quality. Cortisol reduction at the 600 mg dose.
- Cooley 2009 (PLoS ONE) — naturopathic care including Withania for GAD vs psychotherapy; significant improvement in the herbal group, comparable to psychotherapy.
Dosing: 300–600 mg KSM-66 twice daily (so 600–1,200 mg total), or 240 mg Sensoril once daily. Standard practice is to start at the lower end for 2 weeks, then increase if tolerated. Take with food. Onset of subjective effect is gradual — 2–3 weeks is typical for first noticeable benefit; 6–8 weeks for full effect. Some practitioners cycle ashwagandha (8 weeks on, 2 weeks off) but there is no published evidence that cycling is necessary.
Cautions specific to ashwagandha: pregnancy and breastfeeding (traditional contraindication, theoretical risk); hyperthyroidism (ashwagandha can raise T3/T4 modestly — usually beneficial in hypothyroid patients but problematic in hyperthyroidism); autoimmune disease (immunomodulatory, theoretical concern of stimulating autoimmunity though no consistent clinical signal); the rare LiverTox-classified hepatotoxicity reports (very uncommon, generally with Sensoril or higher-potency extracts at supratherapeutic doses).
Rhodiola Rosea
Rhodiola rosea (golden root, arctic root) is a succulent flowering plant native to high-altitude regions of the Arctic and the mountains of Europe, Asia, and North America. The bioactive root has been used in Russian, Scandinavian, and Inuit traditional medicine for fatigue, altitude resilience, depression, and impotence. The Soviet research program in the 1960s–1980s identified rhodiola as one of the three core "Soviet adaptogens" alongside eleuthero and schisandra, and it was widely used by Soviet cosmonauts, Olympic athletes, and military personnel.
Active compounds: rosavins (specifically rosavin, rosin, and rosarin — a group unique to R. rosea within the genus) and salidroside. The most-studied commercial extract is SHR-5 (Swedish Herbal Institute), standardized to 3% rosavins and 1% salidroside.
Clinical evidence for anxiety:
- Bystritsky 2008 (Journal of Alternative and Complementary Medicine) — 10 adults with DSM-IV GAD, open-label pilot of 340 mg rhodiola daily for 10 weeks. Significant improvement on Hamilton Anxiety Scale and Four-Dimensional Anxiety and Depression Scale.
- Cropley 2015 (Phytotherapy Research) — 81 mildly anxious adults randomized to 200 mg WS®1375 rhodiola extract twice daily vs no treatment for 14 days. Significant reduction in stress, anger, confusion, and depression; significant improvement on subjective mood scales.
- Olsson 2009 (Planta Medica) — 60 burnout-syndrome patients randomized to 576 mg SHR-5 daily vs placebo for 28 days. Significant improvement on burnout, fatigue, attention, and salivary cortisol awakening response.
- Mao 2015 (Phytomedicine) — rhodiola vs sertraline (Zoloft) for mild-to-moderate depression. Rhodiola produced smaller benefit than sertraline but with substantially fewer side effects; for some patients the benefit/burden tradeoff favored rhodiola.
Dosing: 200–600 mg SHR-5 or equivalent extract daily, divided morning and early afternoon (NOT evening — rhodiola is mildly stimulating and can disrupt sleep if taken late). Onset of subjective effect is unusually fast for an adaptogen — many patients notice benefit within 3–7 days, particularly the reduction in fatigue and brain fog. Full anxiety effect typically takes 2–4 weeks.
Clinical phenotype: rhodiola is uniquely suited to the burnout-and-anxiety presentation — the patient who is exhausted, anxious, sleeping poorly, brain-fogged, and unable to recover from chronic stress. The Olsson burnout trial captures this population perfectly. For pure anxiety without fatigue, other adaptogens (ashwagandha, holy basil) are usually a better first choice.
Cautions specific to rhodiola: bipolar disorder (rhodiola can precipitate hypomanic episodes in susceptible individuals, similar to other antidepressant-like agents); pregnancy and breastfeeding (insufficient data); MAO inhibitor interaction (theoretical, due to mild MAOI activity of some constituents); evening dosing (can cause insomnia — take before 2 PM).
Holy Basil (Tulsi, Ocimum sanctum)
Holy basil, called tulsi in Sanskrit, is venerated in Hindu tradition as the earthly manifestation of the goddess Lakshmi and is grown in courtyards of Hindu households across India. Distinct from culinary basil (Ocimum basilicum), holy basil (Ocimum sanctum, also called Ocimum tenuiflorum) is used both ritually and medicinally as a daily adaptogen for stress, infection resilience, blood sugar control, and general vitality.
Active compounds: eugenol (the same volatile oil that gives clove its character), ursolic acid, rosmarinic acid, and a complex of triterpenes and flavonoids. Standardized extracts are typically quantified by ursolic acid content.
Clinical evidence for anxiety:
- Saxena 2012 (Evidence-Based Complementary and Alternative Medicine) — the OciBest trial. 158 adults with stress-related symptoms randomized to OciBest 1200 mg/day (a proprietary holy basil extract) vs placebo for 6 weeks. Results: 39% reduction in symptom severity score (vs 14% placebo); significant improvement in forgetfulness, sleep, exhaustion, and sexual symptoms.
- Bhattacharyya 2008 (Nepal Medical College Journal) — 35 patients with GAD given 500 mg tulsi twice daily for 60 days. Significant reduction on Hamilton Anxiety Scale, with anxiety, stress, depression scores all decreasing.
- Cohen 2014 (Journal of Ayurveda and Integrative Medicine) — comprehensive review of tulsi clinical data across stress, immune, metabolic, and cognitive outcomes. Concludes tulsi is a "herb for all reasons" with multi-target benefit and excellent safety record.
Dosing: 500 mg standardized extract twice daily, or 1–2 g of dried leaf as tea (steep covered, 5–10 minutes), or fresh leaves chewed (the traditional method). Available as capsules, tincture, loose leaf tea, and ready-to-drink bottled preparations. Onset is gradual; 4–6 weeks for noticeable anxiety reduction.
Clinical phenotype: holy basil is best suited to the patient who wants a daily everyday adaptogen, particularly one drawn to Ayurvedic traditions or who enjoys ritual tea. It is gentle, well-tolerated, and has the broadest "general wellness" profile of the adaptogens covered here, with additional benefits in blood sugar regulation, oral health, and respiratory infection prevention.
Cautions specific to holy basil: hypoglycemia (holy basil can lower fasting blood glucose; monitor in diabetic patients on hypoglycemic medication); hypothyroidism (animal studies suggest possible thyroid suppression at very high doses; clinical relevance unclear in humans); bleeding risk (mild antiplatelet effect; caution with anticoagulants); pregnancy (traditional use in pregnancy but limited modern safety data).
Lemon Balm (Melissa officinalis)
Lemon balm is a perennial herb in the mint family with a distinct lemony aroma. Native to southern Europe and the Mediterranean basin, it has been used since at least the era of Theophrastus and Dioscorides as a calming herb, sleep aid, and digestive remedy. The 11th-century Persian physician Avicenna wrote that lemon balm "causeth the heart to be merry." Modern use focuses on anxiety, sleep-onset insomnia, and cognitive performance under stress.
Strictly speaking, lemon balm is a nervine (a calming herb that acts on the nervous system) rather than a true adaptogen, but it is included here because of its strong evidence base for anxiety and its frequent inclusion in adaptogenic formulas.
Active compounds: rosmarinic acid (the dominant phenolic acid), citral, geraniol, and a small amount of essential oil. Mechanism is primarily through GABAergic activity — rosmarinic acid inhibits GABA transaminase, the enzyme that degrades GABA, thereby raising synaptic GABA levels.
Clinical evidence for anxiety:
- Kennedy 2003 (Phytotherapy Research) — the foundational modern lemon balm trial. 18 healthy volunteers given 600 mg lemon balm extract or placebo before a Defined Intensity Stressor Simulation. Lemon balm significantly improved both alertness and calmness self-ratings.
- Cases 2011 (Mediterranean Journal of Nutrition and Metabolism) — 20 anxious adults given 600 mg lemon balm extract daily for 15 days. Significant reduction on Hamilton Anxiety Scale, with measurable improvements in anxiety, anxiety-associated insomnia, and quality of life.
- Akhondzadeh 2003 (Journal of Neurology, Neurosurgery, and Psychiatry) — lemon balm for mild-to-moderate Alzheimer's agitation. 4 months of 60 drops/day produced significant cognitive improvement and reduction in agitation.
- Pukka herbal tea blends — widely sold formulas combining lemon balm with chamomile, passionflower, and lavender. Multiple small studies of these blends suggest measurable reduction in subjective anxiety.
Dosing: 300–600 mg standardized extract twice daily, or 1–2 tsp dried leaf as tea (steep covered, 10 minutes), 2–3 cups daily. Tincture: 2–6 mL three times daily of 1:5 alcohol extract. Onset is unusually fast for a herbal anxiolytic — many patients notice acute calming within 30–60 minutes of a tea or capsule.
Clinical phenotype: lemon balm is best suited to mild daily anxiety, sleep-onset insomnia, and patients who want a herbal anxiolytic gentle enough for daytime use without sedation. It is the most child-friendly herbal anxiolytic and is widely used in pediatric practice for childhood anxiety, sleep onset issues, and exam stress.
Cautions specific to lemon balm: hypothyroidism (very high doses may suppress TSH; clinically rare at normal supplementation but worth knowing); pregnancy (traditional use but limited modern data, conservative approach); sedative interactions (additive with benzodiazepines and alcohol, though clinically mild).
Other Adaptogens Worth Knowing
- Eleuthero (Eleutherococcus senticosus, formerly "Siberian ginseng") — the original Soviet adaptogen. Stimulating, used for fatigue resilience and immune support. Less specifically anxiolytic than ashwagandha or holy basil; sometimes overstimulating in anxious patients.
- Schisandra (Schisandra chinensis) — Chinese five-flavor berry. Adaptogenic with mild anxiolytic effect; particularly used in traditional Chinese medicine for liver support and stress resilience.
- Panax ginseng — the most-traded adaptogen historically. More stimulating than calming; can worsen anxiety in some patients. Better for cognitive performance and fatigue than for anxiety.
- American ginseng (Panax quinquefolius) — gentler than Asian ginseng; modest evidence for cognitive support and mood; not specifically anti-anxiety.
- Cordyceps — medicinal fungus with adaptogenic profile. Best evidence for exercise performance and immune modulation; modest mood benefit.
- Reishi (Ganoderma lucidum) — medicinal mushroom. Calming, with traditional use for "shen" (spirit) disturbance. Some evidence for sleep and anxiety; widely used in formulas.
- Bacopa monnieri — Ayurvedic herb. Best evidence for cognitive support and reducing anxiety associated with cognitive demand (test anxiety, public speaking); 8–12 weeks for full effect.
- Mucuna pruriens — velvet bean, source of natural L-DOPA. Used for mood and motivation; can worsen anxiety in some patients due to dopaminergic effect.
For most patients with primary anxiety, the four lead adaptogens covered above (ashwagandha, rhodiola, holy basil, lemon balm) cover the relevant clinical phenotypes. Adding more herbs to the differential rarely improves matching and may introduce confusion.
How to Choose Which Adaptogen
| Patient Phenotype | First-Line Adaptogen | Why |
|---|---|---|
| High cortisol, wired and tired, sleep disturbance | Ashwagandha | Strongest cortisol-reduction evidence; calming, restores sleep |
| Burnout, exhausted, brain fog, anxious | Rhodiola | Energizing and anxiolytic simultaneously; fast onset |
| Daily generalized anxiety, otherwise healthy | Holy basil | Gentle, well-tolerated, broad adaptogenic profile |
| Sleep-onset anxiety, acute calming needed | Lemon balm | Fast-onset GABAergic; good for situational and acute anxiety |
| Hyperthyroidism present | Holy basil or lemon balm | Avoid ashwagandha (mild thyroid stimulation) |
| Bipolar history | Holy basil or lemon balm | Avoid rhodiola (can precipitate hypomania) |
| Pediatric anxiety | Lemon balm (tea or tincture) | Best safety record in pediatric use; gentle |
Stacking and Sequencing
Adaptogens generally combine well with each other and with other natural anxiolytics. Common stacks:
- Ashwagandha + magnesium glycinate — foundational stack for chronic stress with anxiety and sleep disturbance. 600 mg KSM-66 divided AM and lunch + 300–400 mg Mg glycinate at bedtime.
- Rhodiola + L-theanine — rhodiola (morning) for energy and HPA recalibration plus L-theanine for moment-to-moment calming. Excellent for the high-functioning anxious patient who can't afford to slow down.
- Ashwagandha + holy basil — complementary adaptogens, often combined in formulas. 300 mg ashwagandha + 500 mg holy basil daily.
- Holy basil tea + lemon balm tea (alternating) — the gentle daily ritual approach for mild anxiety. Holy basil morning, lemon balm evening.
- Adaptogen + SSRI — generally safe and synergistic, but watch for serotonin syndrome if combining rhodiola or holy basil at high doses with SSRIs and SNRIs (theoretical, rare in practice). Add adaptogen 4 weeks after SSRI is stable.
Avoid stacking multiple stimulating adaptogens (rhodiola + eleuthero + panax ginseng) — the combination is usually overstimulating and can worsen anxiety in susceptible patients.
Cautions and Drug Interactions
- Pregnancy and breastfeeding — data are limited for all of these herbs. Conservative approach is to avoid adaptogens during pregnancy and breastfeeding except under specific naturopathic or midwife supervision.
- Hyperthyroidism — avoid ashwagandha. Holy basil and lemon balm are acceptable; rhodiola is acceptable but watch for jitteriness.
- Bipolar disorder — avoid rhodiola (can precipitate hypomanic episodes). Other adaptogens generally safe.
- Autoimmune disease — theoretical concern with ashwagandha (immunomodulatory); discuss with prescriber if on immunosuppressants.
- Surgery — stop all adaptogens 2 weeks before surgery (theoretical bleeding risk with holy basil, theoretical sedative interaction with ashwagandha).
- Pediatric use — lemon balm is well-studied in children; ashwagandha has some pediatric data; rhodiola and holy basil have limited pediatric data. Consult pediatrician before use under age 12.
- SSRI / SNRI interactions — theoretical serotonin syndrome with rhodiola and holy basil at high doses; in practice this is rare but worth knowing.
- Hypoglycemia interactions — holy basil can lower blood glucose; ashwagandha may also; adjust diabetes medications if needed.
- Sedative interactions — lemon balm and ashwagandha can potentiate benzodiazepines, alcohol, and sleep medications. Usually clinically mild but worth knowing.
- Quality and contamination — adaptogen quality varies dramatically by manufacturer. Buy USP, ConsumerLab, or NSF certified products from reputable brands. Avoid bulk powders from unknown sources due to heavy metal and pesticide contamination risk (particularly relevant for ashwagandha, where Indian agriculture has documented heavy metal issues).
Key Research Papers
- Chandrasekhar K, Kapoor J, Anishetty S (2012). A prospective, randomized double-blind, placebo-controlled study of safety and efficacy of a high-concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety in adults. Indian Journal of Psychological Medicine. — PMID: 23439798
- Lopresti AL, Smith SJ, Malvi H, Kodgule R (2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha (Withania somnifera) extract: A randomized, double-blind, placebo-controlled study. Medicine (Baltimore). — PMID: 31517876
- Salve J, Pate S, Debnath K, Langade D (2019). Adaptogenic and anxiolytic effects of ashwagandha root extract in healthy adults: a double-blind, randomized, placebo-controlled clinical study. Cureus. — PMID: 32021735
- Panossian A, Wikman G (2010). Effects of adaptogens on the central nervous system and the molecular mechanisms associated with their stress-protective activity. Pharmaceuticals (Basel). — PMID: 27713248
- Cropley M, Banks AP, Boyle J (2015). The effects of Rhodiola rosea L. extract on anxiety, stress, cognition and other mood symptoms. Phytotherapy Research. — PMID: 26502953
- Bystritsky A, Kerwin L, Feusner JD (2008). A pilot study of Rhodiola rosea (Rhodax) for generalized anxiety disorder. Journal of Alternative and Complementary Medicine. — PMID: 18307390
- Olsson EM, von Schéele B, Panossian AG (2009). A randomised, double-blind, placebo-controlled, parallel-group study of the standardised extract SHR-5 of the roots of Rhodiola rosea in the treatment of subjects with stress-related fatigue. Planta Medica. — PMID: 19016404
- Saxena RC, Singh R, Kumar P et al. (2012). Efficacy of an Extract of Ocimum tenuiflorum (OciBest) in the Management of General Stress. Evidence-Based Complementary and Alternative Medicine. — Search PubMed
- Cohen MM (2014). Tulsi - Ocimum sanctum: A herb for all reasons. Journal of Ayurveda and Integrative Medicine. — PMID: 25624701
- Kennedy DO, Little W, Scholey AB (2004). Attenuation of laboratory-induced stress in humans after acute administration of Melissa officinalis (lemon balm). Psychosomatic Medicine. — PMID: 15272110
- Cases J, Ibarra A, Feuillere N et al. (2011). Pilot trial of Melissa officinalis L. leaf extract in the treatment of volunteers suffering from mild-to-moderate anxiety disorders and sleep disturbances. Mediterranean Journal of Nutrition and Metabolism. — PMID: 22207903
- Speers AB, Cabey KA, Soumyanath A, Wright KM (2021). Effects of Withania somnifera (ashwagandha) on stress and the stress-related neuropsychiatric disorders. Current Neuropharmacology. — PMID: 34254920
PubMed Topic Searches
- PubMed: Ashwagandha anxiety / cortisol
- PubMed: Rhodiola anxiety / burnout
- PubMed: Holy basil / tulsi anxiety
- PubMed: Lemon balm anxiety
- PubMed: Adaptogen HPA axis
Connections
- Natural Anxiety Relief Hub
- Natural Anxiety Relief Benefits
- L-Theanine and Green Tea
- Magnesium Glycinate
- Breath and Cold Exposure
- Ashwagandha
- Rhodiola Rosea
- Holy Basil (Tulsi)
- Lemon Balm
- Passionflower
- Bacopa Monnieri
- Schisandra
- Reishi
- Stress Management
- All Remedies