The Sinclair Stack and Scientific Critique
David Sinclair's daily longevity protocol — widely discussed in his book Lifespan, his podcast appearances, and his Joe Rogan interviews — consists of approximately 1g NMN, 1g resveratrol (suspended in yogurt for fat absorption), 1g metformin, Vitamin D3, a statin, and low-dose aspirin. It is the most cited consumer longevity protocol of the 2020s and has driven hundreds of millions of dollars in supplement sales. This page lays out the protocol, evaluates each component on its actual evidence, identifies the conflicts of interest, contrasts it with more conservative evidence-graded longevity strategies, and provides a framework for thinking through whether (and how much of it) to adopt personally. Spoiler: the protocol is not crazy, but several components are more speculative than the marketing suggests, and a more conservative version based on rigorous evidence costs less and is probably as effective.
Table of Contents
- The Sinclair Protocol as Stated
- Component Critique: NMN
- Component Critique: Resveratrol
- Component Critique: Metformin
- Component Critique: Statin and Low-Dose Aspirin
- Component Critique: Vitamin D3 and TMG
- Conflicts of Interest
- An Evidence-Graded Alternative Stack
- A Framework for Personal Decision Making
- Key Research Papers
- Connections
- Featured Videos
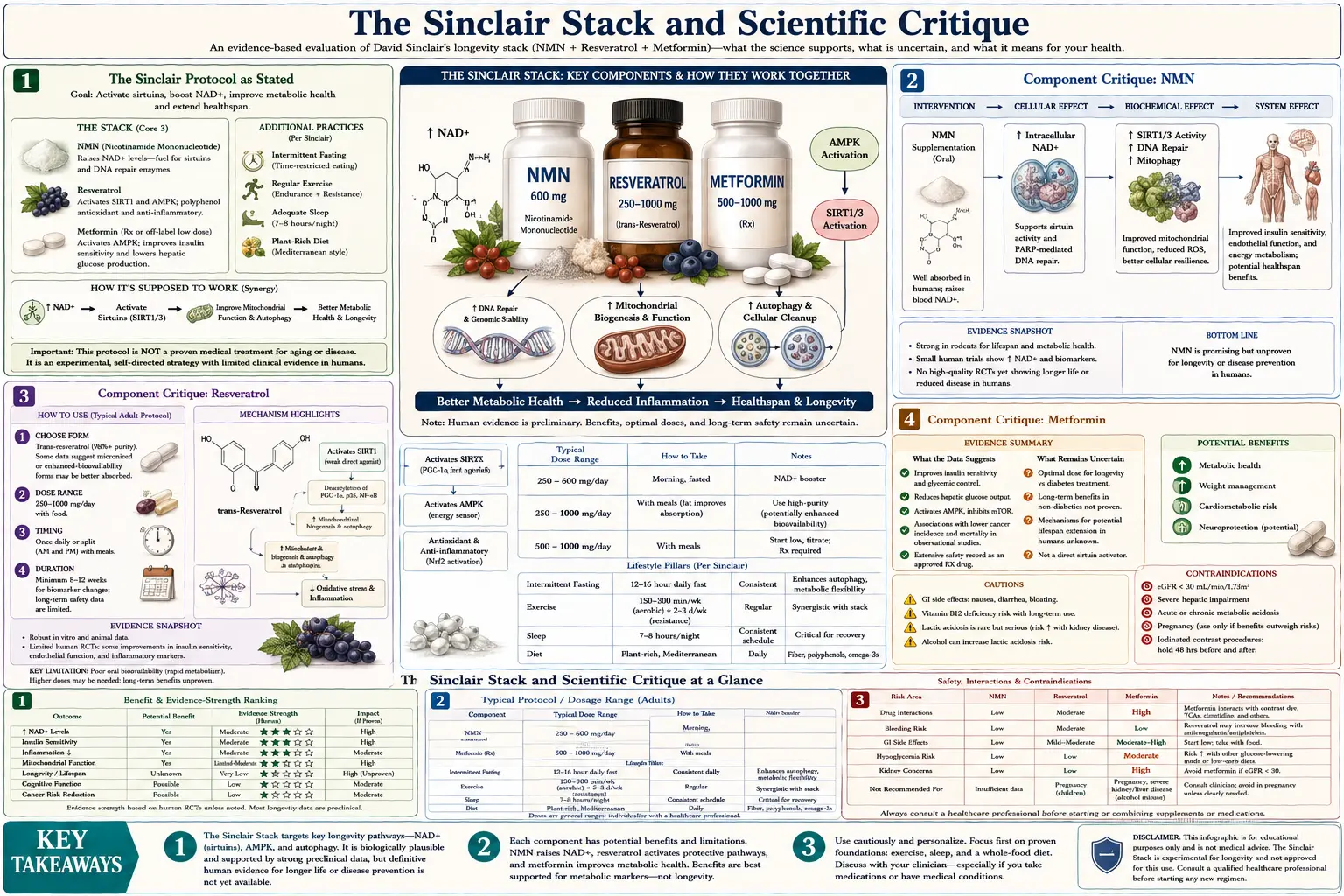
The Sinclair Protocol as Stated
Sinclair has described his personal protocol consistently across interviews and his book. The current published version includes:
- 1 g NMN (nicotinamide mononucleotide), taken in the morning
- 1 g resveratrol, taken in the morning with yogurt or olive oil (fat for absorption)
- 1 g metformin, taken in the evening, skipping on heavy exercise days
- Vitamin D3, dose not always specified (likely 2000–5000 IU)
- Vitamin K2, dose not specified
- Statin (initially atorvastatin, more recently rosuvastatin)
- Low-dose aspirin (typically 81 mg)
- Spermidine, sometimes mentioned
- TMG (trimethylglycine), sometimes mentioned, to support methylation of NAD precursors
- Co-enzyme Q10 and alpha-lipoic acid, less frequently mentioned
The lifestyle complement: time-restricted eating (typically one or two meals per day), plant-heavy diet with reduced animal protein, regular sauna and cold exposure, resistance training, and high-intensity interval training. The lifestyle component is arguably more rigorously evidence-supported than the pharmaceutical component, but receives less attention in popular discussion.
Sinclair has publicly stated that the protocol is his personal choice based on the available evidence, that he does not recommend it to others, and that the evidence is incomplete. Whatever the disclaimers, the protocol has been widely adopted in modified forms by tech executives, the longevity-curious public, and many of his podcast listeners.
Component Critique: NMN
NMN is the headline component of the Sinclair stack. The full critique is on the NAD Boosters page. Briefly:
- Evidence for raising blood NAD+ in humans: yes, multiple trials confirm.
- Evidence for extending mouse lifespan: moderate. Mills et al. 2016 showed mitigated age-associated decline, not formal lifespan trials.
- Evidence for extending human lifespan or healthspan: none.
- Evidence for clinical benefit in any specific endpoint: weak. Yoshino 2021 showed improved muscle insulin sensitivity in prediabetic women, and the magnitude was modest.
- Mechanism of action: probably indirect through conversion to NR or nicotinamide in the gut. The Slc12a8 transporter mechanism is contested.
- Regulatory status: the FDA removed NMN from dietary supplement status in 2022, making US-market NMN regulatory uncertain.
- Cost: $30–$80/month for 1g/day.
Verdict: The biological hypothesis is plausible, the evidence for clinical benefit is thin, and NR is the better-studied, less regulatorily-uncertain alternative at roughly equivalent cost. If supplementing an NAD precursor, NR is the more defensible choice. If NMN, sublingual delivery (Sinclair's reported approach) is not strongly supported by pharmacokinetic data.
Component Critique: Resveratrol
The full critique is on the Sirtuin Activators page. The summary:
- Evidence in cell and mouse studies: extensive but contested. The original Howitz/Baur papers in yeast and obese mice were dramatic. The Pacholec 2010 artifact critique forced a more nuanced view: resveratrol is a substrate-selective SIRT1 activator.
- Evidence in human trials: many small trials of cardiovascular and metabolic biomarkers. Effect sizes are small (~3–5 mmHg blood pressure reduction, ~0.2% HbA1c reduction).
- Lifespan evidence in humans: the InCHIANTI cohort (Semba JAMA Intern Med 2014) found NO association between urinary resveratrol metabolites and mortality over 9 years in 783 older Italians. This is the closest thing to a long-term real-world test of dietary-level resveratrol and is essentially null.
- Product quality: most commercial resveratrol is poorly preserved and contains substantial degraded material. Pterostilbene is the more bioavailable analog.
- Cost: $10–$30/month at 1g/day.
Verdict: Resveratrol at 1g/day has been studied more rigorously than most longevity compounds, and the human evidence does not strongly support a lifespan-extending effect at achievable doses. The InCHIANTI null result is particularly damaging. Pterostilbene at 100–250 mg/day is the more rational stilbenoid choice if any. The yogurt-suspension trick reflects the genuine pharmacokinetic problem (poor oral bioavailability) but does not solve it.
Component Critique: Metformin
The full critique is on the Caloric Restriction and Mimetics page.
- Evidence for clinical benefit in diabetics: very strong. Metformin is first-line for type 2 diabetes for excellent reasons.
- Evidence for mortality benefit in diabetics vs non-diabetic controls: the Bannister 2014 observational data showed lower mortality in metformin-treated diabetics than matched non-diabetics. This is suggestive but observational.
- Evidence for benefit in healthy non-diabetics: limited and mixed. The TAME trial has not yet enrolled patients as of late 2025.
- Exercise interaction: real and concerning. Konopka et al. 2019 showed metformin blunts the cardiometabolic adaptation to exercise in older adults. Sinclair's reported strategy of skipping metformin on heavy exercise days is a rational response.
- Side effects: B12 deficiency with long-term use, GI upset in many users, rare lactic acidosis, generally well-tolerated.
- Cost: generic, very inexpensive ($5–$15/month).
Verdict: Metformin is the most defensible pharmaceutical component of the stack. The evidence is strongest of the small molecules. The exercise interaction is the main caveat, and the cycling strategy addresses it reasonably. Off-label use in healthy adults requires a physician's involvement and is becoming increasingly accepted within longevity medicine practice.
Component Critique: Statin and Low-Dose Aspirin
The statin and aspirin components are interesting because they are not specifically longevity drugs — they are standard cardiovascular preventives.
Statins reliably lower LDL cholesterol by 30–50% depending on dose and agent. In primary prevention populations (no prior cardiovascular event but with risk factors), statins reduce ASCVD events by 20–30% over five years. The absolute mortality benefit in low-to-moderate-risk individuals is modest (~1% over 5 years). In high-risk and secondary prevention populations the benefit is much larger.
The question of whether a 50-something with average cardiovascular risk should take a statin is one of the most discussed in preventive cardiology. Calculators like the ASCVD pooled cohort equations or the PREVENT calculator (2023) provide individualized risk estimates. Sinclair's personal statin use reflects an aggressive primary prevention approach that many cardiologists endorse for adults with elevated apoB or Lp(a).
Low-dose aspirin for primary prevention has lost favor in recent years. The ASPREE trial (Lancet 2018) in healthy older adults found that 100 mg/day aspirin did NOT reduce mortality or cardiovascular events in primary prevention, and DID increase major bleeding events. The 2019 ACC/AHA guideline recommends against routine primary prevention aspirin in most adults. Sinclair's continued use of aspirin is at odds with current guideline recommendations.
Verdict on the cardiovascular components: a statin in adults with elevated cardiovascular risk is well-supported. Aspirin for primary prevention in low-risk adults is not currently recommended and the Sinclair stack is out of step with mainstream guidelines on this point.
Component Critique: Vitamin D3 and TMG
Vitamin D3 at 2000–5000 IU/day is reasonable for most adults living at temperate latitudes or with limited sun exposure. The VITAL trial showed no overall mortality benefit from Vitamin D supplementation, but did show reduced cancer mortality in late follow-up and a reduction in autoimmune disease incidence. Vitamin D's role in immune function, bone health, and muscle function is broader than its skeletal indication. Inexpensive, well-tolerated, defensible component.
TMG (trimethylglycine, betaine) at 500–1000 mg/day is rational on NAD-precursor protocols because methylation of nicotinamide consumes SAM (S-adenosylmethionine), and TMG donates methyl groups via the BHMT pathway. Whether the additional methyl-donor support is necessary in practice is unclear — most well-nourished adults have sufficient methyl groups from dietary choline and folate.
Vitamin K2 (typically as MK-7) at 100–200 mcg/day is reasonable for adults supplementing Vitamin D, to support proper calcium handling. Evidence base is modest but mechanism is sound.
Spermidine, sometimes mentioned, has reasonable mechanistic support (autophagy induction) and one population study (Kiechl, Am J Clin Nutr 2018) showing reduced mortality in Bruneck cohort with higher dietary spermidine. Supplement evidence is weaker.
Verdict: the Vitamin D3, K2, and TMG components are the most defensible parts of the stack, costing little and being well-tolerated. The lifestyle complement (TRE, plant-heavy diet, exercise, sauna) is the strongest evidence-supported component of all.
Conflicts of Interest
Any evaluation of the Sinclair stack must acknowledge the financial conflicts that have surrounded its dissemination. These are publicly disclosed but worth stating clearly.
- Sirtris Pharmaceuticals: Sinclair co-founded Sirtris in 2004 to develop synthetic STACs based on his lab's work. GSK acquired Sirtris in 2008 for $720M, of which Sinclair received a substantial share. GSK shut down the Sirtris division after the SRT2104 and related compounds failed to meet endpoints in trials.
- OvaScience: Sinclair co-founded this fertility company in 2012; the company was later acquired and renamed Millendo Therapeutics.
- InsideTracker: Sinclair has been a scientific advisor and equity holder.
- Tally Health: epigenetic-clock company co-founded by Sinclair, sells DNA methylation aging tests and NMN-based supplement products. Direct financial interest in NMN sales.
- Metro International Biotech: longevity-focused biotech with Sinclair involvement.
- Various consumer NMN brands: Sinclair has had advisory or equity relationships with multiple NMN supplement companies.
None of these conflicts mean Sinclair is wrong about NMN or the broader stack. They do mean that his publicly stated personal protocol is also, in effect, a sales pitch for products he has financial interest in. This pattern was sharply criticized by Charles Brenner in the New York Times and elsewhere, particularly around the 2023 Cell paper on epigenetic age reversal, which was followed shortly by Tally Health product launches.
The fair takeaway is not that Sinclair's science is fraudulent — it is not — but that his role as the public face of a stack he profits from creates a structural incentive to overstate the evidence. Independent academics like Charles Brenner, Luigi Fontana, and Matt Kaeberlein have publicly disagreed with multiple aspects of the protocol and the supporting claims.
An Evidence-Graded Alternative Stack
What does a longevity stack look like if built strictly from the rigorous evidence rather than the popular narrative? A reasonable evidence-graded version, organized by strength of evidence:
Tier 1 (strongly evidence-supported, low cost, low risk):
- Vitamin D3 2000–5000 IU/day with Vitamin K2 MK-7 100 mcg/day
- Omega-3 fatty acids (EPA+DHA 1–2 g/day) from fish or algae oil
- Time-restricted eating, 10–12 hour eating window
- Resistance training 2–3 sessions/week, 90+ minutes/week of moderate aerobic activity
- Sleep optimization (7–9 hours, consistent timing)
- Mediterranean diet pattern with high vegetable, legume, fish, and olive oil intake
- Adequate protein (1.0–1.2 g/kg in adults over 50, especially around resistance training)
Tier 2 (moderate evidence, modest cost, low risk):
- Statin for adults with elevated cardiovascular risk (use a risk calculator)
- Glycine 1–3 g/day (extends rodent lifespan, supports sleep, methylation)
- Creatine 5 g/day (supports muscle preservation and cognition)
- Magnesium glycinate 200–400 mg/day if dietary intake is low
- NR or NMN at 500 mg–1 g/day (substrate logic, modest human evidence)
Tier 3 (mechanistic plausibility, weaker direct evidence, requires physician oversight):
- Metformin 500 mg–1 g/day in non-diabetic adults (TAME hypothesis, observational data)
- Low-dose intermittent rapamycin (5 mg weekly) under physician supervision
- Acarbose with high-carbohydrate meals (postprandial glucose control)
- Pterostilbene 100–250 mg/day (sirtuin substrate logic)
- Spermidine 1–5 mg/day (autophagy induction)
Tier 4 (more speculative; consider only with strong personal indication):
- Apigenin 25–100 mg/day (CD38 inhibition)
- Senolytic protocols (quercetin + dasatinib, or fisetin pulse dosing)
- Hormonal optimization (testosterone, growth hormone, thyroid) where deficient
- Peptide protocols (BPC-157, TB-500, MOTS-c, etc.)
The Tier 1 interventions cost under $50/month combined and have the strongest evidence. Tiers 2 and 3 add another $50–$150/month. Tier 4 is where costs escalate dramatically (hundreds to thousands per month) and where evidence is weakest. A rational longevity stack should max out Tier 1 before considering Tier 2, and so on.
A Framework for Personal Decision Making
For any specific compound in the stack (or any longevity intervention generally), ask:
- What is the proposed mechanism? Is it linked to a known hallmark of aging? Can the proponent name it in one sentence?
- What is the evidence in mice? Has it extended lifespan in the NIA ITP or comparable rigorous trial? Or only in disease-model mice?
- What is the human pharmacokinetic evidence? Does the oral dose actually deliver the compound to the target tissue?
- What is the human clinical biomarker evidence? Has it improved validated aging biomarkers (epigenetic clocks, telomere length, IGF-1, inflammatory markers) in randomized trials?
- What is the human endpoint evidence? Has it reduced cardiovascular events, cancer, cognitive decline, or all-cause mortality?
- What are the conflicts of interest? Does the principal advocate have direct financial stake in supplement sales?
- What are the realistic downside risks? What is the worst plausible side effect, and how often does it occur?
- What is the cost, and what would the same money buy in Tier 1 interventions?
Most longevity supplements that pass questions 1 and 2 fail questions 4 and 5. That is not necessarily a reason to avoid them — medicine routinely uses biomarker-supported interventions before endpoint trials — but it is a reason to be measured about the claims and conservative about the cost.
The closing recommendation: build a rigorous Tier 1 foundation (exercise, sleep, diet, Vitamin D, omega-3, time-restricted eating). Layer in Tier 2 selectively where lab markers (e.g. elevated apoB, low NAD+) support the addition. Consider Tier 3 with physician involvement and clear personal rationale. Treat Tier 4 as experimentation rather than evidence-based medicine.
Key Research Papers
- Sinclair DA, LaPlante MD. Lifespan: Why We Age — and Why We Don't Have To. 2019 (book; not peer-reviewed but lays out the framework) PubMed: Sinclair related work
- Yang H et al. Loss of epigenetic information as a cause of mammalian aging. Cell 2023; 186:305–326 (Sinclair ICE mouse) — PubMed PMID: 36638792
- Lu Y et al. Reprogramming to recover youthful epigenetic information and restore vision (Sinclair lab OSK reprogramming). Nature 2020; 588:124–129 — PubMed PMID: 33268865
- Brenner C. A science-based review of the world's best-selling NMN supplements (critical perspective). Cell Metab 2022; 34:1–3 PubMed: Brenner NMN critique
- Semba RD et al. Resveratrol levels and all-cause mortality in older community-dwelling adults. JAMA Intern Med 2014; 174:1077–1084 — Search PubMed
- Bannister CA et al. Can people with type 2 diabetes live longer than those without? Diabetes Obes Metab 2014; 16:1165–1173 — PubMed PMID: 25041462
- Konopka AR et al. Metformin inhibits mitochondrial adaptations to aerobic exercise training in older adults. Aging Cell 2019; 18:e12880 — PubMed PMID: 30548390
- McNeil JJ et al. Effect of aspirin on all-cause mortality in the healthy elderly (ASPREE). N Engl J Med 2018; 379:1519–1528 — PubMed PMID: 30221595
- Manson JE et al. Vitamin D supplements and prevention of cancer and cardiovascular disease (VITAL). N Engl J Med 2019; 380:33–44 — PubMed PMID: 30415629
- Kiechl S et al. Higher spermidine intake is linked to lower mortality (Bruneck cohort). Am J Clin Nutr 2018; 108:371–380 — Search PubMed
- Belsky DW et al. Decoding the pace of biological aging from a six-CpG DNA methylation algorithm (DunedinPACE). eLife 2022; 11:e73420 — PubMed PMID: 35029144
- Waziry R et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging. Nat Aging 2023; 3:248–257 — PubMed PMID: 37118425
- Yoshino M et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science 2021; 372:1224–1229 — PubMed PMID: 33888596
- Dollerup OL et al. A randomized placebo-controlled clinical trial of nicotinamide riboside in obese men. Am J Clin Nutr 2018; 108:343–353 — Search PubMed
- Mannick JB et al. Targeting the biology of ageing with mTOR inhibitors to improve immune function in older adults. Lancet Healthy Longev 2021; 2:e250–e262 — PubMed PMID: 33977284
Connections
- Benefits Deep Dive (Hub)
- Caloric Restriction and Mimetics
- NAD Boosters
- Sirtuin Activators
- Longevity Protocols (Main)
- NMN (Nicotinamide Mononucleotide)
- NR (Nicotinamide Riboside)
- Resveratrol
- Metformin
- Rapamycin
- Vitamin D3
- Vitamin K2
- Spermidine
- Creatine
- Senolytics
- Intermittent Fasting