Caloric Restriction and Mimetics for Longevity
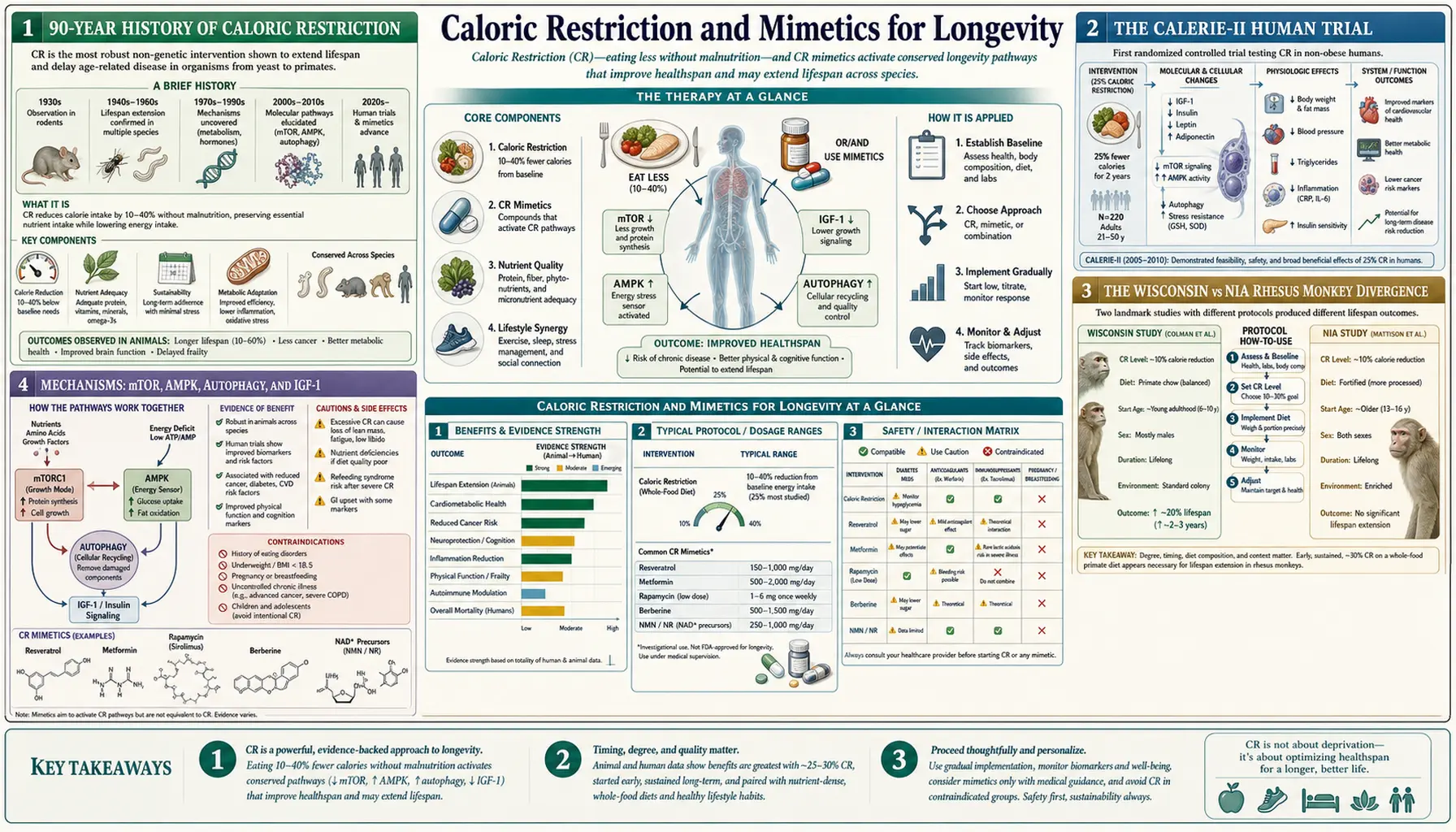
Caloric restriction (CR) — reducing energy intake by 15–40% without malnutrition — is the most reproducible non-genetic intervention for extending lifespan ever discovered. First reported by Clive McCay at Cornell in 1935, it has now been shown to extend lifespan in yeast, worms, flies, fish, rodents, and (with caveats) non-human primates. The CALERIE-II trial showed it improves human cardiometabolic biomarkers and slows the pace of biological aging on epigenetic clocks. Because few people can sustain 15% CR for decades, the field has invested heavily in "CR mimetics" — drugs that reproduce the metabolic signature of CR without the food deprivation. This page walks through the human and animal evidence and the four leading mimetics: rapamycin, metformin, acarbose, and the SGLT2 inhibitors.
Table of Contents
- 90-Year History of Caloric Restriction
- The CALERIE-II Human Trial
- The Wisconsin vs NIA Rhesus Monkey Divergence
- Mechanisms: mTOR, AMPK, Autophagy, and IGF-1
- Intermittent Fasting and Time-Restricted Eating
- Rapamycin (mTOR Inhibition)
- Metformin and the TAME Trial
- Acarbose and SGLT2 Inhibitors
- Practical Application and Cautions
- Key Research Papers
- Connections
- Featured Videos
90-Year History of Caloric Restriction
The story begins in 1935 with Clive McCay at the Cornell Nutrition Laboratory. McCay was investigating whether nutrient density could affect rat development, and he discovered something startling: rats fed an essentially complete diet but with calories restricted by approximately 40% lived dramatically longer than ad-libitum-fed controls — up to twice as long for the longest-lived individuals. The restricted rats remained lean, active, and youthful in appearance through ages at which control rats had long since died. The 1935 Journal of Nutrition paper is a foundational document of geroscience.
For the next sixty years, caloric restriction was studied almost exclusively in rodents, where the result is among the most reproducible in all of biology. Restrict calories by 20–40% from a young age in mice or rats, and median lifespan extends by 20–50%, maximum lifespan extends by 10–30%, and the animals show reduced incidence and delayed onset of essentially every major age-related disease — cancer, cardiovascular disease, diabetes, neurodegeneration, and immune decline. The breadth of the phenotype was central to the modern reframing of aging: if a single intervention can simultaneously delay so many seemingly unrelated diseases, then aging itself must have shared upstream drivers that the intervention is hitting.
The next major wave of research extended CR to invertebrates, where the same effect appears: roughly 1.5× to 2× lifespan extension in C. elegans and Drosophila. The evolutionary conservation across yeast (where it was first identified by Leonard Guarente's lab in the late 1990s), worms, flies, and mammals strongly suggests that CR is acting through ancient, conserved nutrient-sensing pathways.
Two large primate trials — the Wisconsin study at the Wisconsin National Primate Research Center, and the NIA study at the National Institute on Aging — began in the late 1980s and have produced partially divergent results. They are the closest thing to a long-term human-relevant CR experiment, and they are discussed in their own section below.
The CALERIE-II Human Trial
The most rigorous human CR study to date is CALERIE-II (Comprehensive Assessment of Long-term Effects of Reducing Intake of Energy, Phase 2), conducted at three sites (Pennington, Tufts, Washington University) under NIH funding. CALERIE-II randomized 220 non-obese adults (BMI 22–28) to either ad-libitum eating or a target of 25% caloric restriction for two years. The actual achieved restriction averaged about 12% (CR is hard to sustain even with intensive support), with a range from 1% to 20% among individual participants.
Headline findings: the CR group lost about 10% of body weight, reduced LDL cholesterol, lowered systolic and diastolic blood pressure, reduced fasting insulin and HOMA-IR (insulin resistance index), reduced markers of systemic inflammation including TNF-alpha and CRP, and improved cardiometabolic risk indicators across the board. Most consequentially for the geroscience field, a 2023 re-analysis by Belsky and colleagues found that the CR group had a slowed pace of biological aging on the DunedinPACE epigenetic clock, by approximately 2–3% over the two-year intervention.
Important caveats: CALERIE-II did not measure mortality (the trial was far too short and the participants too healthy at baseline). The biological-aging slowdown is suggestive but small. Some bone-density loss was observed in the CR group, raising concerns about long-term skeletal health on sustained restriction. And the very fact that participants achieved only 12% restriction despite intensive intervention illustrates the central practical problem with CR as a human longevity strategy — sustainability.
The Wisconsin vs NIA Rhesus Monkey Divergence
The two large CR primate trials — both in rhesus macaques, both running for thirty-plus years — have produced partially divergent results that have generated extensive interpretation debate.
The Wisconsin trial, led by Richard Weindruch and Ricki Colman, started in 1989 and reported in Science in 2009 that 30% CR reduced age-related deaths from cancer, cardiovascular disease, and diabetes, and modestly extended both median and maximum lifespan. The CR monkeys also showed reduced sarcopenia and better preserved brain volume on MRI.
The NIA trial, led by Donald Ingram and Julie Mattison, also started in the late 1980s and reported in Nature in 2012 that 30% CR did not significantly extend lifespan in their cohort, although it did reduce age-related disease incidence and improve some metabolic biomarkers. Maximum lifespan effects, if any, were modest.
What explains the divergence? Several factors have been proposed, all credible:
- Diet composition: the Wisconsin diet was higher in sucrose; the NIA diet was based on natural ingredients including fish meal and was lower in sucrose. The NIA control monkeys may already have been on a relatively restricted, nutrient-dense diet (effectively a mild CR comparator).
- Feeding protocol: NIA controls were portion-controlled, not truly ad libitum; Wisconsin controls were fed more freely. This narrowed the actual difference between groups in the NIA study.
- Genetic background: the two cohorts came from different breeding colonies with different baseline lifespans.
- Onset age: NIA included both juvenile and adult-onset CR groups; Wisconsin started with adults.
A joint 2017 re-analysis by both teams concluded that the trials were ultimately consistent with each other and with the broader CR literature, that CR reduces age-related disease in primates, that lifespan effects depend strongly on the comparator diet, and that the "magic" of CR is at least partly about avoiding overnutrition rather than restriction per se. The pragmatic takeaway for humans is that moderate CR, plus a high-quality diet, plus avoiding the Western pattern of constant grazing on hyperpalatable food, captures most of the benefit without the suffering.
Mechanisms: mTOR, AMPK, Autophagy, and IGF-1
The molecular signature of caloric restriction is well-mapped and converges on four interlocking systems.
- mTOR inhibition: amino acid deprivation (and especially low leucine and methionine) suppresses mTORC1 activity. mTORC1 is the master signal that says "build proteins, store fat, grow." When suppressed, the cell stops building and starts recycling. Pharmacologic mTOR inhibition with rapamycin reproduces a major slice of the CR phenotype.
- AMPK activation: low ATP/AMP ratio activates AMPK, which is the cellular "low fuel" alarm. AMPK switches off anabolic processes (lipid synthesis, protein synthesis, gluconeogenesis) and switches on catabolic processes (fatty acid oxidation, glucose uptake, autophagy). Metformin and berberine are the canonical AMPK activators.
- Autophagy upregulation: both mTOR inhibition and AMPK activation converge on autophagy — the cellular recycling system that breaks down damaged organelles and aggregated proteins. Autophagy declines with age, and reactivating it is increasingly recognized as a unifying mechanism behind CR's broad health benefits. Spermidine, rapamycin, and fasting are the most direct autophagy activators.
- IGF-1 / Growth Hormone reduction: CR reduces circulating IGF-1 by 15–40% in animals (much less in humans, where protein restriction matters more than caloric restriction for IGF-1). Low IGF-1 signaling in tissues activates the FOXO family of stress-response transcription factors, which upregulate antioxidant and DNA-repair genes.
The four pathways are heavily interconnected and partially redundant. This is why no single drug perfectly mimics CR — CR hits all four simultaneously, while rapamycin mostly hits mTOR, metformin mostly hits AMPK, and so on.
Intermittent Fasting and Time-Restricted Eating
The most practical adaptation of CR for humans is not chronic restriction but periodic fasting. The two dominant formats are intermittent fasting (alternate-day eating, or 5:2 patterns with two low-calorie days per week) and time-restricted eating (TRE: compressing all eating into a 6–10 hour window). Both produce many of the metabolic adaptations of CR without requiring sustained calorie counting.
The mechanism is largely circadian. Mammalian metabolism is rhythmic, and constant snacking from 6 am to 11 pm overrides the night-time period during which insulin should fall, growth hormone should pulse, and autophagy should activate. A 12–16-hour overnight fast restores those rhythms even if total daily calories are unchanged. Satchin Panda's lab at the Salk Institute has shown in mice that time-restricted feeding without calorie restriction prevents diet-induced obesity, fatty liver, and metabolic dysfunction.
Human trials have been mixed. Early small studies suggested TRE produced weight loss and metabolic improvement beyond what calorie reduction alone explained. A larger 2022 NEJM trial (Liu et al.) randomized obese adults to either 8-hour TRE plus 25% calorie restriction, or 25% calorie restriction alone, and found no additional benefit from the TRE component — suggesting calorie deficit, not meal timing, drives most of the weight loss. However, TRE may still confer non-weight-related benefits (better insulin sensitivity, improved sleep, lower blood pressure) that are not captured by weight-focused trials.
Practical recommendations: a 12–14 hour overnight fast (finish dinner by 7 pm, breakfast at 7–9 am) is well tolerated, restores circadian metabolism, and produces measurable insulin sensitivity improvement in most people. Longer fasts (16+ hours) may activate autophagy more strongly but become difficult to sustain socially and risk lean-mass loss if not paired with adequate protein intake during the eating window. Multi-day fasting (3–5 days) periodically — popularized by Valter Longo's Fasting-Mimicking Diet — produces a strong autophagy and stem-cell-regeneration signal but should be done under supervision in older or medicated individuals.
Rapamycin (mTOR Inhibition)
Rapamycin is the strongest pharmaceutical lifespan extender ever identified in mammals. Originally isolated from a soil bacterium on Easter Island (Rapa Nui) in 1972, it was developed as an immunosuppressant to prevent organ transplant rejection. In 2009, the NIA Interventions Testing Program reported in Nature that rapamycin extended median lifespan in genetically heterogeneous mice by 9–14% in males and females, even when started at 600 days of age (roughly equivalent to age 60 in humans). This was the first pharmaceutical to robustly extend lifespan in a mammal when started in middle age.
Mechanism: rapamycin binds FKBP12 and the complex inhibits mTORC1, which is the central nutrient-sensing kinase. Reduced mTORC1 activity suppresses protein synthesis, activates autophagy, and reduces senescent-cell burden — many of the same effects as caloric restriction but achievable without dietary change.
Open questions in humans: the dose and schedule used to extend mouse lifespan (continuous low-dose oral rapamycin) is different from clinical transplant dosing (high daily dose). Intermittent dosing protocols (5 mg weekly, or 1–6 mg weekly with 1–3 week pulses) appear in off-label longevity practice and have been associated with improved immune function in older adults in small trials (Mannick et al., 2014, 2018) using the rapamycin analog everolimus. Side effects at low dose are usually mild — transient mouth sores, mild lipid elevation, occasional glucose dysregulation. Side effects at transplant doses include nephrotoxicity and immunosuppression and are not relevant to longevity dosing.
The PEARL trial (Participatory Evaluation of Aging with Rapamycin for Longevity) is a 2022–2025 randomized, placebo-controlled trial in healthy adults using low-dose intermittent rapamycin and tracking aging biomarkers. Results are expected to be the first reasonably rigorous human longevity-endpoint data on rapamycin.
Metformin and the TAME Trial
Metformin is the most prescribed type 2 diabetes drug in the world, used by over 150 million people. Observational studies starting in the 2010s noted that diabetic patients on metformin had lower all-cause mortality not just than other diabetics but, strikingly, than non-diabetics in matched cohorts — suggesting an anti-aging effect beyond glucose control. The most cited paper (Bannister, Diabetes Obes Metab 2014) reported that metformin-treated diabetics had a 15% lower mortality than non-diabetic matched controls over five years of follow-up.
Mechanism: metformin partially inhibits mitochondrial Complex I, which lowers cellular ATP and activates AMPK. AMPK in turn inhibits mTORC1 and activates autophagy. Metformin also reduces hepatic gluconeogenesis (its glucose-lowering mechanism), alters the gut microbiome, reduces inflammation, and may have direct effects on the DNA damage response.
The TAME trial (Targeting Aging with Metformin), proposed by Nir Barzilai at Albert Einstein and the American Federation for Aging Research, would be the first FDA-recognized trial with "aging" as the endpoint. Design: ~3,000 adults aged 65–79, randomized to metformin or placebo, primary composite endpoint of cardiovascular events, cancer, cognitive decline, and death over six years. As of late 2025 the trial has not yet enrolled patients because of funding hurdles, but the regulatory pathway it would establish — FDA acceptance of a composite aging endpoint — is itself a major contribution.
Caveats: a 2019 study (Konopka et al.) suggested metformin blunts the cardiometabolic benefits of exercise in older adults. Long-term metformin use is associated with B12 deficiency. The MILES trial (Metformin in Longevity Study) found mixed effects on muscle-tissue gene expression in older adults. The bottom line for healthy non-diabetic people considering metformin off-label for longevity: the evidence is more suggestive than definitive, and the exercise interaction is a real concern for active individuals.
Acarbose and SGLT2 Inhibitors
Two other diabetes drugs have shown longevity signals worth noting.
Acarbose is an alpha-glucosidase inhibitor that blocks carbohydrate digestion in the gut, blunting postprandial glucose spikes. In the NIA Interventions Testing Program, acarbose extended median male mouse lifespan by 22% and female mouse lifespan by 5% (Strong et al., Aging Cell 2016). The sex-specific effect is notable and unexplained. Acarbose mimics CR by reducing absorbed calories and flattening the glucose-insulin response, and is well-tolerated except for gas and bloating from undigested carbohydrate reaching the colon.
SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) lower glucose by causing renal glucose excretion. In the EMPA-REG OUTCOME trial and subsequent SGLT2-inhibitor cardiovascular outcome trials, these drugs reduced cardiovascular death by ~30% in type 2 diabetics with established cardiovascular disease — an effect size unprecedented for a glucose-lowering drug. The mechanism is thought to include reduced cardiac preload, mild ketosis, and possibly direct cardioprotection. Empagliflozin extended median male mouse lifespan in the ITP in 2024 reporting. The drug class is now standard for diabetic patients with heart failure or chronic kidney disease.
Whether non-diabetic adults should take SGLT2 inhibitors for longevity is open. The cardiac benefit is well-established only in patients with existing cardiovascular or renal disease. The cost is meaningful ($500+ per month in the US until generics arrive). Side effects include genital yeast infections, volume depletion, and rare diabetic ketoacidosis even in mildly hyperglycemic patients.
Practical Application and Cautions
What can a non-specialist actually do with this body of evidence?
- Stop overnutrition. The strongest signal from CR research is that the modern Western pattern of constant high-calorie eating is itself an aging accelerant. Eating to approximate satiety rather than fullness, reducing portion sizes, and eliminating snacking between meals captures much of the "CR mimetic" benefit at zero cost.
- Time-restricted eating: compress eating to a 10–12 hour window. Most evidence-supported intervention with the lowest implementation cost.
- Periodic longer fasts: a 24–72 hour fast quarterly, or a 5-day Fasting-Mimicking Diet annually, activates autophagy and stem-cell turnover. Not appropriate for low-BMI, pregnant, or medicated individuals without supervision.
- Protein adequacy: lean mass preservation matters more in older adults than CR. Most longevity researchers now recommend 1.0–1.2 g protein per kg body weight in adults over 50, even though this slightly elevates IGF-1, because sarcopenia kills more people than the IGF-1 differential.
- Pharmaceutical mimetics: rapamycin and metformin are both used off-label for longevity. Both require physician supervision, baseline labs, periodic monitoring, and an honest conversation about uncertain evidence vs known side effects. Acarbose is cheap and well-tolerated and may be the most evidence-supported option for non-diabetics looking to flatten postprandial glucose.
Cautions: caloric restriction is contraindicated in low-BMI individuals, anyone with active eating disorders, frail older adults at risk of sarcopenia, pregnancy, growing children, and athletes during heavy training cycles. Long-term CR causes bone density loss and cold intolerance. Rapamycin and metformin require a physician's involvement. None of these interventions has been demonstrated to extend human lifespan — the strongest evidence is for healthspan extension and biomarker improvement.
Key Research Papers
- McCay CM, Crowell MF, Maynard LA. The effect of retarded growth upon the length of life span and upon the ultimate body size. J Nutr 1935; (the founding paper) PubMed: McCay 1935
- Colman RJ et al. Caloric restriction delays disease onset and mortality in rhesus monkeys. Science 2009; 325:201–204 — PubMed PMID: 19590001
- Mattison JA et al. Impact of caloric restriction on health and survival in rhesus monkeys from the NIA study. Nature 2012; 489:318–321 — PubMed PMID: 22932268
- Mattison JA et al. Caloric restriction improves health and survival of rhesus monkeys. Nat Commun 2017; 8:14063 — PubMed PMID: 28094793
- Kraus WE et al. (CALERIE-II) 2 years of calorie restriction and cardiometabolic risk. Lancet Diabetes Endocrinol 2019; 7:673–683 — PubMed PMID: 31303390
- Waziry R et al. Effect of long-term caloric restriction on DNA methylation measures of biological aging in healthy adults from the CALERIE trial. Nat Aging 2023; 3:248–257 — PubMed PMID: 37118425
- Harrison DE et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature 2009; 460:392–395 — PubMed PMID: 19587680
- Mannick JB et al. mTOR inhibition improves immune function in the elderly. Sci Transl Med 2014; 6:268ra179 — PubMed PMID: 25540326
- Bannister CA et al. Can people with type 2 diabetes live longer than those without? A comparison of mortality in people initiated with metformin or sulphonylurea monotherapy and matched, non-diabetic controls. Diabetes Obes Metab 2014; 16:1165–1173 — PubMed PMID: 25041462
- Barzilai N et al. Metformin as a tool to target aging. Cell Metab 2016; 23:1060–1065 (TAME rationale) — PubMed PMID: 27304501
- Strong R et al. Longer lifespan in male mice treated with a weakly estrogenic agonist, an antioxidant, an alpha-glucosidase inhibitor or a Nrf2-inducer. Aging Cell 2016; 15:872–884 — Search PubMed
- Liu D et al. Calorie restriction with or without time-restricted eating in weight loss. N Engl J Med 2022; 386:1495–1504 — PubMed PMID: 35443107
- Madeo F et al. Spermidine in health and disease. Science 2018; 359:eaan2788 — PubMed PMID: 29371440
- Longo VD, Mattson MP. Fasting: molecular mechanisms and clinical applications. Cell Metab 2014; 19:181–192 — PubMed PMID: 24440038
- Mitchell SJ et al. Daily fasting improves health and survival in male mice independent of diet composition and calories. Cell Metab 2019; 29:221–228 — Search PubMed
Connections
- Benefits Deep Dive (Hub)
- NAD Boosters
- Sirtuin Activators
- Sinclair Stack and Critique
- Longevity Protocols (Main)
- Intermittent Fasting
- Autophagy
- Metformin
- Rapamycin
- Berberine
- Spermidine
- Type 2 Diabetes
- Coronary Artery Disease
- HbA1c
- Fasting Insulin